Saddle Joint Degeneration | Beak Ligament Failure | Grind Test | Eaton-Littler Staging
- Saddle joint anatomy - unique biaxial motion allows opposition and circumduction
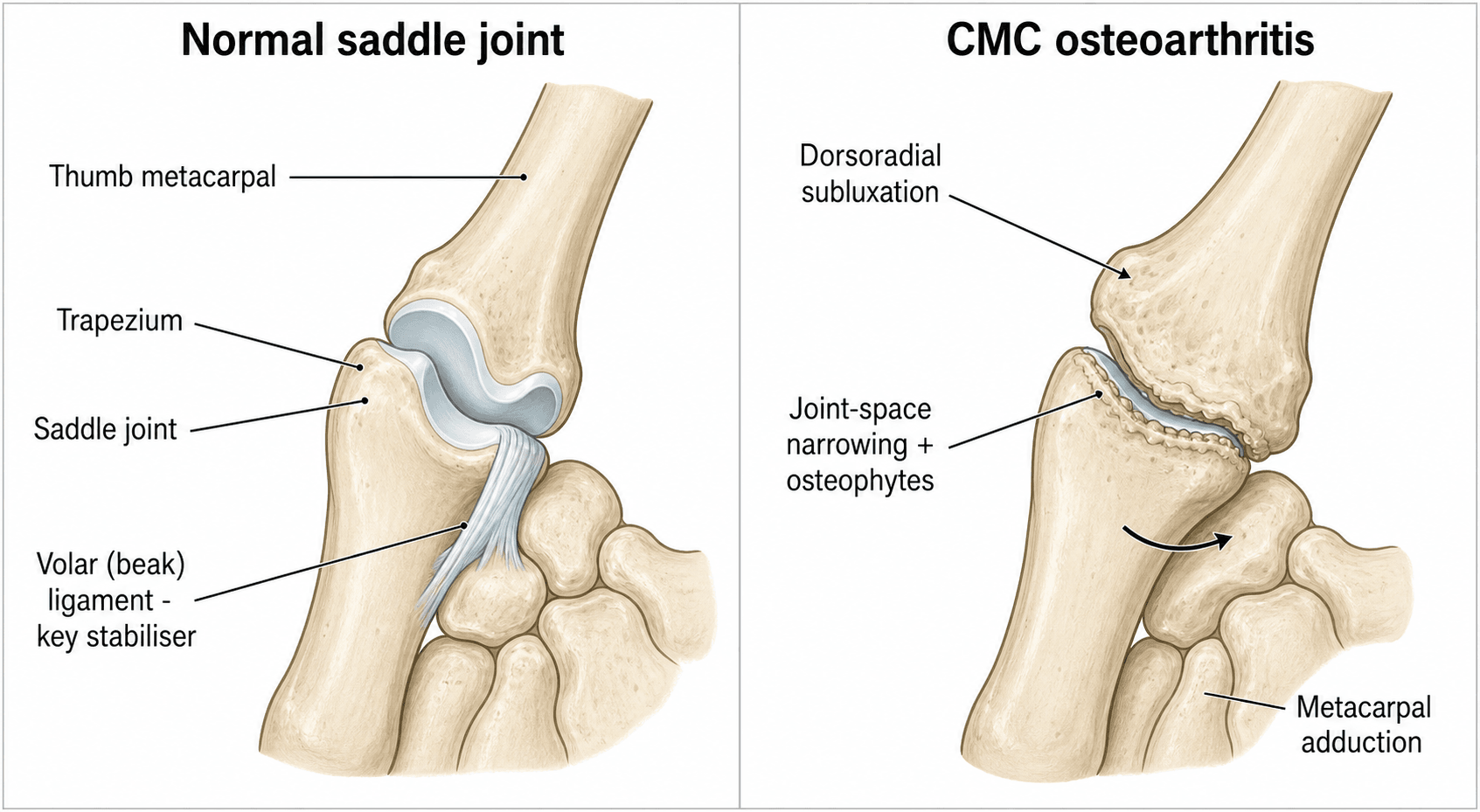
- Anterior oblique (beak) ligament is primary stabilizer - failure leads to subluxation
- Grind test is pathognomonic - axial compression with rotation reproduces pain
- Eaton-Littler staging guides treatment - Stage I-II conservative, III-IV surgical
- Trapeziectomy with LRTI is gold standard - 90%+ satisfaction, preserves motion
- CMC arthroplasty emerging option - preserves height but higher complication rate
- “CMC arthritis is the most common site of hand osteoarthritis
- “Anterior oblique ligament (beak ligament) is the key primary restraint
- “Grind test positive = pain with axial load and rotation of thumb metacarpal
- “Stage IV includes scaphotrapezial-trapezoid (STT) joint involvement
- “LRTI = Ligament Reconstruction and Tendon Interposition
- “FCR is most commonly used donor tendon for LRTI
The CMC joint is a saddle joint (sellar joint) with reciprocally curved surfaces allowing biaxial motion. This unique anatomy permits opposition and circumduction but creates high contact stresses predisposing to arthritis.
The anterior oblique ligament (AOL), also called the beak ligament, is the primary restraint to dorsoradial subluxation. Its attenuation or failure is the initial pathologic step leading to progressive arthritis.
Stage I-II can be treated conservatively. Stage III has isolated CMC arthritis requiring trapeziectomy plus or minus LRTI. Stage IV involves the STT joint and may require extended procedures like arthrodesis.
Trapeziectomy with LRTI remains the gold standard with over 90% patient satisfaction. Simple trapeziectomy alone has higher subsidence rates. CMC arthroplasty is emerging but has higher revision rates.
- Radiographic Findings
- Widening of joint space, no narrowing, synovitis
- First-Line Treatment
- Splinting, NSAIDs, activity modification, steroid injection
- Surgical Options
- Arthroscopic synovectomy (rarely indicated)
- Radiographic Findings
- Joint space narrowing, osteophytes less than 2mm
- First-Line Treatment
- Splinting, NSAIDs, steroid injection, trial of 3-6 months
- Surgical Options
- Trapeziectomy with LRTI, ligament reconstruction alone
- Radiographic Findings
- Severe narrowing, osteophytes greater than 2mm, sclerosis
- First-Line Treatment
- Surgery if conservative fails
- Surgical Options
- Trapeziectomy with LRTI (gold standard), CMC arthroplasty, arthrodesis
- Radiographic Findings
- Pantrapezial arthritis, STT joint involved
- First-Line Treatment
- Surgery addressing all involved joints
- Surgical Options
- Trapeziectomy with LRTI, STT fusion, complete arthrodesis
FCRFCR SLIP - Donor Tendon
Hook:FCR SLIP is the most common donor - half the tendon used, wrist flexion preserved
Overview and Epidemiology
Thumb carpometacarpal (CMC) arthritis, also known as trapeziometacarpal osteoarthritis or basilar joint arthritis, is the most common site of osteoarthritis in the hand. It affects the articulation between the first metacarpal and the trapezium.
- Prevalence increases with age - affects up to 33% of postmenopausal women
- Female to male ratio approximately 15:1
- Bilateral involvement in 40-70% of cases
- Most common symptomatic presentation is Stage II-III disease
- Female sex (hormonal factors, ligamentous laxity)
- Age greater than 50 years
- Previous trauma or fracture
- Repetitive pinch activities (occupational)
- Joint laxity or hypermobility
- Genetic predisposition
The CMC joint is a saddle joint with unique biomechanics. High contact stresses during pinch (up to 120 kg/cm²) combined with the small articular surface area predispose to cartilage degeneration. The anterior oblique ligament (beak ligament) acts as the primary restraint, and its attenuation initiates the degenerative cascade.
Natural history:
- Initial ligamentous laxity leads to joint instability
- Abnormal kinematics increase contact stresses
- Progressive cartilage loss and osteophyte formation
- Dorsoradial subluxation of metacarpal base
- Adduction contracture (first web space narrowing)
- Secondary STT arthritis in advanced cases (Stage IV)
Anatomy and Pathophysiology
Osseous anatomy:
- Trapezium: distal carpal row bone with saddle-shaped articular surface
- First metacarpal base: reciprocally curved saddle surface
- Saddle joint (sellar joint): biaxial motion - flexion/extension and abduction/adduction
- Opposition is a combination of abduction, flexion, and pronation
Ligamentous anatomy (16 ligaments described):
The CMC joint has complex ligamentous support with 16 described ligaments. The key structures:
- Location
- Volar-ulnar, beak-shaped
- Function
- Primary restraint to dorsoradial subluxation
- Clinical Significance
- Failure is initiating event in arthritis
- Location
- Dorsal-radial
- Function
- Secondary restraint
- Clinical Significance
- Contributes to stability in extension
- Location
- Between MC1 and MC2
- Function
- Prevents dorsal subluxation
- Clinical Significance
- May be used for reconstruction
- Location
- Dorsal aspect
- Function
- Restraint in flexion
- Clinical Significance
- Less critical than AOL
The anterior oblique ligament (AOL) is also called the beak ligament due to its shape. It originates from the volar-ulnar tubercle of the trapezium and inserts on the volar-ulnar aspect of the metacarpal base. It is the primary restraint and its attenuation is the initial pathologic event. Think of it as the ACL of the thumb CMC joint.
Biomechanics:
- Saddle joint allows two degrees of freedom: flexion/extension and abduction/adduction
- Combination movements create opposition (pronation component from muscle action)
- Contact stresses during pinch are extremely high: 120 kg/cm² (12 MPa)
- Small articular surface area (1-2 cm²) concentrates forces
- Ligamentous restraints prevent subluxation under these high loads
Pathophysiology:
The degenerative cascade:
Anterior oblique ligament stretches or partially tears, often from repetitive microtrauma or hormonal-related laxity. Joint kinematics become abnormal with subluxation during pinch.
Dorsoradial subluxation of the metacarpal base occurs with pinch. Altered contact areas and increased peak stresses damage articular cartilage.
Progressive cartilage loss with fibrillation, fissuring, and full-thickness defects. Subchondral bone exposure and sclerosis. Osteophyte formation at joint margins.
Severe joint space loss, large osteophytes, cyst formation. Adduction contracture develops. In Stage IV, pantrapezial arthritis with STT joint involvement.
Secondary deformities:
- Adduction contracture: first web space narrowing
- Metacarpal base dorsoradial subluxation: prominent "shoulder" at base
- MCP hyperextension: compensatory for adduction (swan neck of thumb)
- Z-deformity: adduction at CMC, hyperextension at MCP, flexion at IP
SADDLESADDLE - Anatomy and Biomechanics
Hook:SADDLE describes the joint anatomy - remember the beak ligament is anterior oblique
Classification Systems
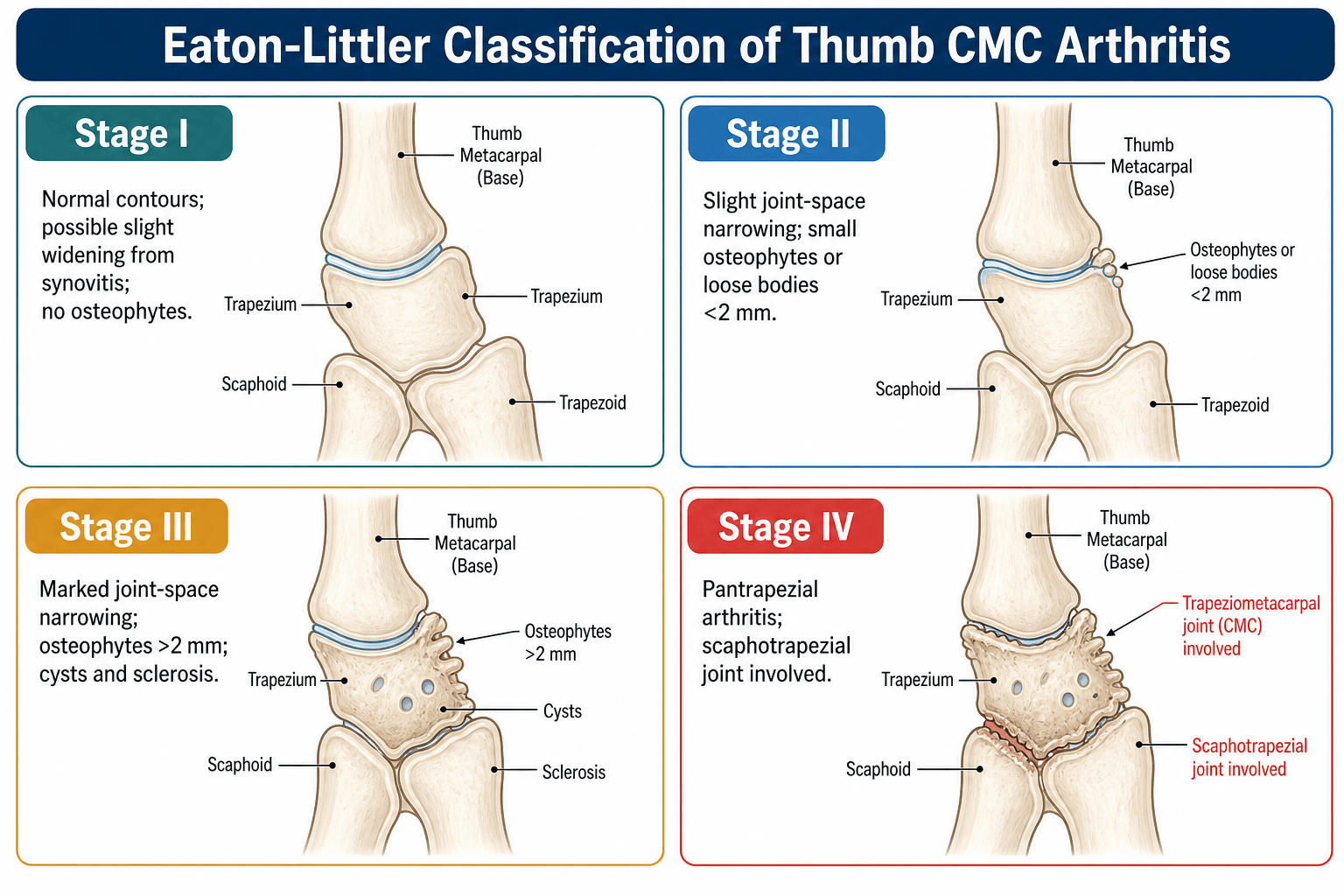
The Eaton-Littler classification (modified Eaton classification) is the standard staging system for thumb CMC arthritis. It is based on radiographic findings and guides treatment decisions.
Stage I: Pre-Arthritic
- Normal joint space or slight widening
- No osteophytes
- Possible joint effusion (synovitis)
- Subluxation may be present on stress views
- Pain with activities
- Tenderness over CMC joint
- Grind test positive
- Maintained pinch strength
- Conservative management primary
- Splinting (thumb spica)
- NSAIDs
- Activity modification
- Corticosteroid injection (diagnostic and therapeutic)
- Arthroscopic synovectomy (rarely indicated)
Stage I is relatively uncommon as patients often present later.
The defining feature of Stage IV is involvement of the STT joint (scaphotrapezial-trapezoid articulation). This is pantrapezial arthritis. Treatment requires addressing the STT joint, either with trapeziectomy (which removes the trapezium articulating with scaphoid) or with combined procedures like STT fusion.
Clinical Presentation and Examination
- Chief complaint: pain at base of thumb, difficulty with pinch activities
- Pain characteristics: worse with pinch, opening jars, turning keys, writing
- Functional impact: reduced grip strength, difficulty with ADLs
- Duration: often gradual onset over months to years
- Previous treatments: splinting, NSAIDs, injections
- Hand dominance: affects functional expectations
- Occupation: heavy manual labor vs. sedentary
Physical examination
- Squaring of thumb base: prominence from dorsoradial subluxation and osteophytes
- Thenar atrophy: in advanced cases
- Adduction contracture: reduced first web space
- MCP hyperextension: compensatory Z-deformity
- Skin changes: overlying the joint
- Tenderness: directly over CMC joint (volar and dorsal)
- Osteophyte palpation: bony prominences at base
- Crepitus: with joint motion
- Synovitis: soft tissue fullness
- Opposition: thumb tip to small finger base (Kapandji score)
- Abduction: measure first web space
- Radial abduction and palmar abduction: often reduced
- Extension: may have compensatory MCP hyperextension
- Technique
- Axial compression of thumb metacarpal with rotation
- Positive Finding
- Pain and/or crepitus reproduced
- Sensitivity
- Very high (pathognomonic)
- Technique
- Stabilize trapezium, translate metacarpal dorsally and volarly
- Positive Finding
- Pain, crepitus, or excessive translation
- Sensitivity
- High for instability
- Technique
- Radial deviation of wrist with compression
- Positive Finding
- Pain over STT joint (Stage IV)
- Sensitivity
- Moderate for STT involvement
- Technique
- Key pinch (lateral) and tip pinch measured
- Positive Finding
- Reduced compared to contralateral (greater than 30%)
- Sensitivity
- Functional assessment
The grind test is the most specific examination finding for CMC arthritis. Hold the thumb metacarpal, apply axial compression (pushing the base toward the trapezium), and rotate the metacarpal. Pain and crepitus are pathognomonic. The test reproduces the high contact stresses that occur during pinch.
Differential diagnosis:
- Pain Location
- Volar/dorsal base of thumb
- Key Test / Sign
- Grind test positive; squaring of base
- Discriminating Feature
- Pain reproduced by axial load + rotation; narrowing on Robert view
- Pain Location
- Radial styloid (1st extensor compartment)
- Key Test / Sign
- Finkelstein / Eichhoff positive
- Discriminating Feature
- Tenderness 1-2cm proximal to CMC joint; grind test negative
- Pain Location
- Distal scaphoid / radial wrist
- Key Test / Sign
- STT tenderness; STT narrowing on imaging
- Discriminating Feature
- Defines Eaton-Littler stage IV when combined with CMC disease
- Pain Location
- Anatomical snuffbox
- Key Test / Sign
- Snuffbox tenderness; scaphoid views
- Discriminating Feature
- Trauma history; proximal to CMC joint
- Pain Location
- Volar wrist over FCR tendon
- Key Test / Sign
- Pain on resisted wrist flexion
- Discriminating Feature
- Linear tenderness along tendon, not over joint
- Pain Location
- Volar wrist / radial 3.5 digits
- Key Test / Sign
- Tinel/Phalen, nerve conduction studies
- Discriminating Feature
- Paraesthesia and night symptoms; may coexist with CMC OA
- First dorsal compartment arthritis: rare; consider if de Quervain symptoms persist
- Trigger thumb: locking and catching at IP or MCP joint, not joint-line pain
Investigations and Imaging
Radiographic assessment:
Standard radiographic series for CMC arthritis:
- Shows joint space narrowing
- Osteophytes
- Subluxation pattern
- Dorsal subluxation visible
- Osteophyte size assessment
- True AP of CMC joint
- Positioning: forearm pronated, thumb extended and opposed
- Best view for joint space narrowing and subluxation
- Most useful for staging
- Resisted tip pinch during radiograph
- Demonstrates dynamic subluxation
- Useful in early disease (Stage I-II)
- Stage I: Normal joint space or widening, stress view shows subluxation
- Stage II: Narrowing, osteophytes less than 2mm
- Stage III: Severe narrowing, osteophytes greater than 2mm, sclerosis
- Stage IV: Above findings plus STT joint involvement
The Robert view (also called Bett view) is the most important radiograph for CMC arthritis. It provides a true AP view of the CMC joint by pronating the forearm and placing the thumb flat on the cassette. This view best demonstrates joint space narrowing and subluxation for Eaton-Littler staging.
- Not routinely required for diagnosis
- May be useful to assess:
- Ligament integrity (AOL)
- Synovitis severity
- Articular cartilage status
- Occult fractures
- STT joint involvement when X-ray equivocal
- Rarely indicated
- May be useful for:
- Preoperative planning for arthrodesis
- Complex deformity assessment
- Failed prior surgery
- Can assess synovitis
- Guide injection procedures
- Limited role compared to radiographs
- Diagnostic injection: local anesthetic into CMC joint
- Pain relief confirms CMC as source
- Distinguishes from de Quervain or STT arthritis
- Therapeutic injection: corticosteroid
- May provide temporary relief (weeks to months)
- Up to 3 injections can be attempted
- Helps select appropriate surgical candidates
GRINDGRIND - Clinical Diagnosis
Hook:GRIND is the pathognomonic test - axial compression and rotation of thumb metacarpal
Management Approach
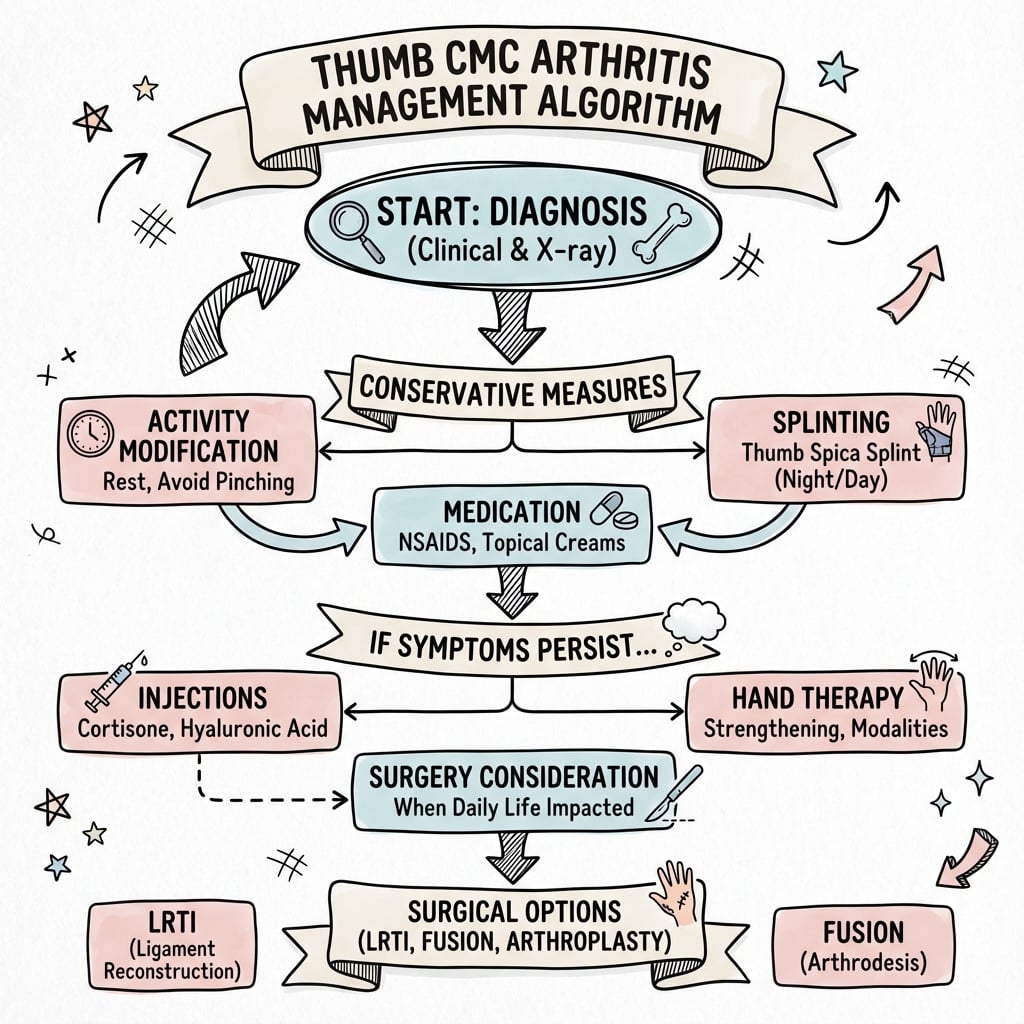
Conservative Management (Stage I-II)
Non-operative treatment trial (3-6 months):
- Thumb spica splinting (removable, worn during activities and night)
- Activity modification (avoid repetitive pinch)
- NSAIDs (oral or topical)
- Hand therapy (strengthening, ROM, adaptive equipment)
- Corticosteroid injection (up to 3 attempts)
Success rate: 40-60% of patients achieve adequate symptom control. Better outcomes in Stage I-II disease.
Surgical Indications
Consider surgery when:
- Failure of conservative management for 3-6 months
- Persistent pain affecting function
- Significant functional limitation (ADLs, occupation)
- Pinch strength loss greater than 30-50%
- Patient motivation for surgical intervention
- Stage III-IV disease (earlier surgical consideration)
These indications apply to properly selected patients with realistic expectations.
Complications of Surgical Treatment
Early complications (less than 6 weeks):
- Incidence
- 5-10%
- Management
- Observation (most resolve), neuroma excision if persistent
- Prevention
- Careful dissection, protect nerve branches
- Incidence
- 1-2%
- Management
- Antibiotics, wound care, possible debridement
- Prevention
- Perioperative antibiotics, sterile technique
- Incidence
- 2-3%
- Management
- Compression, drainage if large
- Prevention
- Hemostasis, drain consideration
- Incidence
- 1-5%
- Management
- Early mobilization, therapy, medications
- Prevention
- Early ROM, avoid prolonged immobilization
Late complications (greater than 6 weeks):
- Incidence
- 20-30% simple, less than 10% LRTI
- Management
- Usually asymptomatic, revision LRTI if symptomatic
- Prevention
- LRTI technique, adequate suspensionplasty
- Incidence
- 5-10%
- Management
- Therapy, revision reconstruction if severe
- Prevention
- Proper LRTI tension, adequate rehabilitation
- Incidence
- 5-10%
- Management
- Investigate cause (incomplete trapeziectomy, STT, de Quervain), treat accordingly
- Prevention
- Complete trapezium removal, assess STT joint
- Incidence
- 2-3%
- Management
- Tenolysis if adhesions, reconstruction if rupture
- Prevention
- Gentle technique, early ROM
- Incidence
- 5-10%
- Management
- Desensitization therapy, scar massage
- Prevention
- Meticulous skin closure, therapy
- Implant loosening (10-15%)
- Dislocation (5-10%)
- Subsidence (5-10%)
- Periprosthetic fracture (2-5%)
- Metallosis (rare)
- Nonunion (5-10%)
- Malunion (improper positioning)
- Hardware failure or irritation
- Adjacent joint arthritis (MCP, STT)
Subsidence (proximal migration of the thumb metacarpal into the trapezial space) occurs in 20-30% of simple trapeziectomy cases but is less common with LRTI (less than 10%). Importantly, radiographic subsidence does not always correlate with poor clinical outcomes. Many patients with subsidence have excellent pain relief and function. Symptomatic subsidence requires revision LRTI.
Surgical Techniques
Trapeziectomy with Ligament Reconstruction and Tendon Interposition
- Stage II-IV disease with failed conservative treatment
- Primary surgical option for most patients
- Standard procedure with best long-term evidence
- Dorsal or volar approach (volar more common)
- Wagner incision: longitudinal over thenar eminence
- Identify and protect radial sensory nerve branches
- Protect palmar cutaneous branch of median nerve
- Identify CMC joint and trapezium
- Dissect circumferentially around trapezium
- Protect FCR tendon (volar approach) or ECRB (dorsal)
- Remove trapezium completely
- Ensure no fragments remain
- Inspect STT joint (Stage IV)
- Harvest half-width of FCR (most common) or entire APL
- FCR: make distal window, retrieve with tendon stripper
- Leave proximal attachment intact
- Length: 10-12 cm typically adequate
- Drill hole in metacarpal base (dorsal-radial to volar-ulnar)
- Second drill hole in index metacarpal base or through FCR tunnel
- Thread tendon through metacarpal hole
- Create sling or anchor to suspend first metacarpal
- Prevents proximal migration and subsidence
- Remaining tendon rolled into ball or figure-of-eight
- Placed in trapezial space as spacer
- Suture to capsule to prevent migration
- Maintains space and prevents subsidence
- Repair capsule
- Close skin
- Apply thumb spica splint with IP joint free
- Complete trapezium removal is essential (prevents pain)
- FCR harvest: take only half width to preserve wrist flexion
- Ensure adequate tension on suspension (not too tight)
- Interposition prevents bone-on-bone contact
- Thumb spica splint for 3-4 weeks
- Remove sutures at 2 weeks
- ROM exercises begin at 4 weeks
- Strengthening at 8-12 weeks
- Avoid heavy lifting for 3 months
This concludes the LRTI technique description.
LRTILRTI - Surgical Technique
Hook:LRTI stands for Ligament Reconstruction and Tendon Interposition - the gold standard
Managing the Hyperextended MCP Joint
The Z (collapse) deformity described earlier - CMC adduction with compensatory MCP hyperextension (the thumb "swan-neck") - has a surgical corollary that is repeatedly examined: a significantly hyperextending thumb MCP must be addressed at the same sitting as the CMC procedure. If it is left uncorrected, the deforming force persists and the trapeziectomy or reconstruction is more likely to fail with recurrent adduction and weak pinch. Assess the MCP passively at surgery and choose by the magnitude and correctability of the hyperextension.
- Problem
- Minor; does not drive recurrence
- Option at the Same Sitting
- Usually no specific MCP procedure needed
- Problem
- Contributes to collapse and weak pinch
- Option at the Same Sitting
- Temporary MCP pinning in about 20-30 degrees of flexion for around 4 weeks, with or without volar capsulodesis
- Problem
- Perpetuates the Z-deformity and threatens the reconstruction
- Option at the Same Sitting
- Volar plate capsulodesis, sesamoid arthrodesis, or EPB-to-metacarpal transfer
- Problem
- Cannot be corrected by soft tissue alone
- Option at the Same Sitting
- MCP arthrodesis in slight (about 15-20 degrees) flexion
A hyperextended thumb MCP is the compensatory half of the Z (collapse) deformity. If you perform a trapeziectomy or LRTI and leave a significantly hyperextending MCP, the deforming force continues and the reconstruction is more likely to fail. Assess the MCP passively at surgery and correct it concurrently - pinning or capsulodesis for moderate flexible hyperextension, and MCP arthrodesis (in slight flexion) for a fixed or arthritic joint.
The Adducted Thumb and First Web Space Contracture
The adduction contracture and first-web narrowing listed among the secondary deformities are also a surgical decision point. Advanced disease pulls the first metacarpal into adduction, narrowing the first web and limiting grasp and opposition. Removing the trapezium does not open a contracted web on its own, so a fixed contracture that is not released will blunt the functional benefit of surgery. Grade the release by severity.
- Finding
- Web narrowed but passively correctable
- Release at the Time of Surgery
- Therapy and stretching; trapeziectomy alone usually restores the web as the metacarpal falls back
- Finding
- Tight adductor pollicis and deep fascia
- Release at the Time of Surgery
- Adductor pollicis recession/release from its third-metacarpal origin, with or without first dorsal interosseous release
- Finding
- Contracted web skin limiting abduction
- Release at the Time of Surgery
- Web deepening with a four-flap (or Z-) plasty, or a local rotation flap
A fixed first-web adduction contracture limits the abduction and opposition you can restore - removing the trapezium does not open a contracted web by itself. Assess the web pre-operatively: for a supple web, trapeziectomy alone is usually enough, but a tight adductor needs a release (adductor recession with or without first dorsal interosseous release) and a skin-deficient web needs a four-flap or Z-plasty at the same sitting.
Postoperative Care and Rehabilitation
- Thumb spica splint or cast
- Includes wrist and thumb CMC/MCP joints
- IP joint free for motion
- Elevate hand to reduce swelling
- Suture removal at 2 weeks
- Continue splinting until week 4
- Remove splint at 4 weeks
- Begin gentle ROM exercises
- Thumb opposition
- Radial and palmar abduction
- CMC and MCP flexion/extension
- Progress to active ROM without resistance
- Custom splint for protection during activities
- Scar massage and desensitization
- Begin progressive resistance exercises
- Pinch strengthening (putty, grippers)
- Grip strengthening
- Functional activities training
- Gradual return to work (light duty)
- Full ROM usually achieved by 3 months
- Strengthening continues for 6 months
- Maximal improvement at 6-12 months
- Return to unrestricted activities at 3-6 months
- Heavy manual labor may require 6 months
- Pain relief: 90-95% of patients
- Pinch strength: 80-90% of contralateral side
- ROM: Slightly reduced but functional
- Satisfaction: 85-95%
- Return to activities: 90%+
Starting ROM at 4 weeks is critical to prevent stiffness and adhesions. Prolonged immobilization beyond 4 weeks increases risk of CRPS and poor functional outcomes. Balance protection of reconstruction with need for early mobilization.
Outcomes and Prognosis
Cochrane Review: No Surgical Technique Proven Superior
- No technique superior for pain or physical function (low-quality evidence)
- Mean pain ~26mm/100 VAS after trapeziectomy alone; LRTI changed pain by only -2.8mm (95% CI -9.8 to 4.2)
- Trapeziectomy with LRTI associated with MORE adverse events (19 vs 10 per 100; RR 1.89)
- No RCT compared surgery with sham or with non-operative care
- Most outcomes evidence remains low quality
Systematic Review: LRTI Not Superior to Simpler Procedures
- No procedure proven superior for pain or function
- Trapeziectomy with LRTI carries a higher complication rate
- Autologous interposition preferable to synthetic spacers (e.g. Artelon)
- Higher-level RCTs comparing arthrodesis and total joint replacement still needed
- Follow-up in higher-evidence trials was short (~12 months), limiting long-term conclusions
Total Joint Replacement: Faster Recovery, Costlier, Higher Complications
- Outcomes very implant-dependent; some implants withdrawn from market
- No clear superiority over trapeziectomy variants
- Higher complication rate and additional implant cost
- Best implants achieve survivorship beyond 10 years
- Worst implants show unacceptably high early failure
RCT: Touch Dual-Mobility Prosthesis vs Tendon Interposition
- Prosthesis group recovered faster, with better strength and ROM throughout follow-up
- Both techniques improved significantly versus preoperative values
- Authors suggest joint replacement be preferred, reserving interposition for prosthetic complications or STT osteoarthritis
- Follow-up limited to 24 months — long-term survivorship not yet established
RCT: Arthrodesis vs LRTI — Trial Stopped for Excess Complications
- Arthrodesis complications 71% vs 29% for LRTI (p=0.016) — trial halted early
- PRWHE and DASH similar between groups at 12 months
- More LRTI patients would repeat their surgery (86% vs 53%, p=0.025)
- Authors do NOT recommend routine plate-and-screw arthrodesis in this group
- Nonunion reported in the literature averages 8-21% after CMC arthrodesis
Intra-Articular Injection: Steroid Fast, Hyaluronate Durable
- Corticosteroid: maximal relief at 2-3 weeks (faster onset)
- Hyaluronate: better pain and pinch power at 26 weeks (more durable)
- Pain improvement reported by 79-88% of patients at 6 months
- Both agents well tolerated with no causally-linked adverse events
- Injection is symptomatic, not disease-modifying
Ligament Anatomy: 16 Ligaments, Beak (Deep AOL) and Dorsoradial Key
- 16 distinct ligaments identified around the trapezium/TMC joint
- Deep anterior oblique (beak) ligament functions as a pivot enabling thumb pronation
- Dorsoradial ligament is a substantial dynamic stabiliser
- Trapezio-second and trapezio-third metacarpal ligaments resist cantilever bending
- Modern biomechanical data implicate the dorsoradial ligament as well as the beak ligament in instability
Guidelines, Registries & Global Practice
Global epidemiology:
In the population-based Rotterdam study (n=3906, age greater than or equal to 55y), radiographic thumb-base osteoarthritis was present in 35.8% of participants, with hand osteoarthritis in at least one joint affecting 67% of women and 54.8% of men — confirming the thumb base as one of the most commonly affected sites (Dahaghin et al, Ann Rheum Dis 2004). The same cohort showed only a modest-to-weak correlation between radiographic change and pain or disability, underscoring that radiographic stage alone should not drive surgical decisions. The Eaton-Littler radiographic classification itself shows only moderate interobserver agreement and fair agreement on treatment choice (Spaans et al, J Hand Surg Am 2011), which is why management is anchored to symptoms and function rather than imaging stage alone.
Side-by-side guidance and evidence base:
- Position
- No surgical technique superior; LRTI adds complications without functional benefit
- Evidence Level
- Level I (low-quality RCT pooling)
- Position
- First-line conservative: education, exercise/hand therapy, topical/oral NSAIDs; intra-articular steroid for short-term relief; surgery only after non-operative failure
- Evidence Level
- Guideline (GRADE-based)
- Position
- Stepwise care: splint + therapy + injection, then trapeziectomy-based surgery; no single 'gold-standard' operation mandated
- Evidence Level
- Consensus / Level II
- Position
- Trapeziectomy +/- interposition mainstay; modern total joint replacement an accepted option in selected patients
- Evidence Level
- Consensus / Level II
- Position
- Dual-mobility total joint replacement gives faster recovery and better early strength/ROM vs interposition
- Evidence Level
- Level I (single-centre RCT)
Registry and implant-surveillance evidence:
Unlike hip and knee replacement, thumb CMC implants are not comprehensively captured by most national joint registries, so survivorship data rely on cohort series and systematic reviews. Huang et al (J Hand Surg Eur Vol 2015) found total-joint survivorship highly implant-dependent, with some designs surviving beyond 10 years and others withdrawn for early failure. This registry gap is a key reason guideline bodies remain cautious about routine arthroplasty and why post-market surveillance is emphasised.
Practice variation:
There is wide international variation in operative choice driven by surgeon training rather than evidence: practice in many high-income settings is dominated by trapeziectomy with or without LRTI, whereas some continental European centres (notably France) have higher uptake of total joint replacement. The Cochrane and Vermeulen reviews show this variation is not justified by superiority data.
MCQ and Exam Practice Points
-
Epidemiology:
- Most common site of osteoarthritis in the hand
- Female to male ratio 15:1
- Affects 33% of postmenopausal women
-
Anatomy:
- Saddle joint (sellar joint) with biaxial motion
- Anterior oblique ligament (beak ligament) is primary stabilizer
- 16 ligaments described around CMC joint
- Contact stress during pinch: 120 kg/cm²
-
Pathophysiology:
- Initial event is AOL attenuation or failure
- Leads to dorsoradial subluxation
- Abnormal kinematics cause cartilage degeneration
-
Clinical examination:
- Grind test is pathognomonic: axial compression with rotation
- Squaring of thumb base from subluxation and osteophytes
- Adduction contracture reduces first web space
-
Eaton-Littler classification:
- Stage I: widening, no narrowing
- Stage II: narrowing, osteophytes less than 2mm
- Stage III: severe narrowing, osteophytes greater than 2mm
- Stage IV: pantrapezial arthritis (STT joint involved)
-
Imaging:
- Robert view (Bett view) is best radiograph for staging
- True AP of CMC joint with forearm pronated
-
Treatment:
- Stage I-II: conservative first (splinting, NSAIDs, injection)
- Stage III-IV: surgery if conservative fails
- Trapeziectomy with LRTI is gold standard
- Success rate 90-95% for pain relief
-
Surgical techniques:
- LRTI: FCR most common donor tendon (half width harvested)
- Simple trapeziectomy has equivalent outcomes but higher subsidence
- Arthrodesis: best for young male manual laborers (maximal strength)
- CMC arthroplasty: higher revision rate (10-15%)
-
Complications:
- Radial sensory nerve injury: 5-10%
- Subsidence: 20-30% simple trapeziectomy, less than 10% LRTI
- Nonunion after arthrodesis: 5-10%
-
Outcomes:
- Pain relief in 90-95% with LRTI
- Pinch strength recovers to 80-90% of contralateral
- Maximal improvement at 6-12 months
- Stage III disease with failed conservative treatment → LRTI
- Young male laborer → arthrodesis
- Persistent post-operative pain → assess for STT arthritis (Stage IV)
- Stage II disease → conservative vs. surgical (shared decision)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old right-hand-dominant female presents with 2 years of progressive right thumb base pain. She reports difficulty opening jars, turning keys, and writing. Conservative treatment with splinting and NSAIDs for 6 months has failed. X-rays show Eaton-Littler Stage III changes. She asks about surgical options.”
“A 35-year-old male carpenter presents with left thumb base pain. He does heavy manual work requiring strong grip and pinch. Examination reveals positive grind test, reduced pinch strength 40% compared to right side. X-rays show Stage III CMC arthritis. He has tried conservative treatment for 4 months without benefit. He asks what operation will give him the strongest grip to return to his carpentry work.”
“A 58-year-old female underwent trapeziectomy with LRTI 6 months ago for Stage III CMC arthritis. She initially improved but now has persistent radial-sided wrist pain, especially with gripping. Examination shows tenderness over the scaphoid and STT joint area. Post-operative X-rays show complete trapezium removal with some subsidence but good alignment. How would you manage this?”
“A 55-year-old female office worker has Stage II CMC arthritis. She has had splinting and two corticosteroid injections over 8 months with temporary relief but pain returns. She asks if she should have surgery now or continue with injections.”
Key Anatomy
- Saddle joint (sellar) - biaxial motion: flexion/extension + abduction/adduction
- Anterior oblique ligament (AOL/beak ligament) - PRIMARY stabilizer, prevents dorsoradial subluxation
- 16 ligaments total described, AOL most important
- High contact stress: 120 kg/cm² during pinch
- Small articular surface (1-2 cm²) predisposes to arthritis
Eaton-Littler Classification
- Stage I: Normal/widened space, synovitis, stress view shows subluxation → Conservative
- Stage II: Narrowing, osteophytes less than 2mm → Conservative trial, surgery if fails
- Stage III: Severe narrowing, osteophytes greater than 2mm, CMC only → Surgery (LRTI gold standard)
- Stage IV: Stage III + STT joint arthritis (pantrapezial) → Surgery addressing all joints
Clinical Examination
- GRIND TEST: axial compression + rotation of MC = pain/crepitus (PATHOGNOMONIC)
- Squaring of thumb base (subluxation + osteophytes)
- Adduction contracture (reduced first web space)
- Thenar atrophy in advanced cases
- Pinch strength reduced (compare to contralateral)
Imaging
- Robert view (Bett view): TRUE AP of CMC joint - BEST for staging
- Eaton stress view: resisted pinch shows dynamic subluxation
- PA and lateral hand views
- Assess STT joint for Stage IV disease
Conservative Treatment
- Thumb spica splinting (activities + night)
- NSAIDs (oral or topical)
- Activity modification
- Corticosteroid injection (up to 3 attempts)
- Hand therapy (strengthening, adaptive equipment)
- Success in 40-60% of Stage I-II patients
Surgical Options
- Trapeziectomy + LRTI: GOLD STANDARD, 90-95% success, FCR tendon most common donor
- Simple trapeziectomy: equivalent outcomes, higher subsidence (20-30% vs less than 10%)
- Arthrodesis: young male laborers, MAX strength (100%+), loses motion, nonunion 5-10%
- CMC arthroplasty: emerging, higher revision (10-15%), not yet standard
- Recovery: 4 weeks splint, ROM at 4 weeks, strengthen 8-12 weeks, full recovery 6-12 months
LRTI Technique
- Complete trapeziectomy (no fragments)
- Harvest HALF of FCR tendon (or entire APL)
- Suspensionplasty: drill MC base, weave tendon, anchor to MC2 or through FCR tunnel
- Interposition: remaining tendon rolled into space as spacer
- Prevents subsidence and bone-on-bone contact
Complications
- Radial sensory nerve injury: 5-10% (paresthesia, neuroma)
- Subsidence: 20-30% simple, less than 10% LRTI (often asymptomatic)
- CRPS: 1-5% (early ROM prevents)
- Persistent pain: incomplete trapezium, STT arthritis, de Quervain
- Arthrodesis: nonunion 5-10%, MCP hyperextension/arthritis long-term
Exam Viva Answers
- Stage III failed conservative → Recommend LRTI, discuss simple trapeziectomy equivalent evidence
- Young male laborer → Arthrodesis for MAX strength, accept loss of motion
- Persistent pain post-op → DDx: STT arthritis (Stage IV), de Quervain, nerve, incomplete removal
- Stage II → Shared decision: surgery justified if failed conservative, or continue if managing
- Difference LRTI vs simple → Subsidence lower with LRTI but outcomes equivalent at 1 year
High-Yield Numbers
- 33% of postmenopausal women affected
- 15:1 female to male ratio
- 90-95% surgical success rate
- 80-90% pinch strength recovery
- 120 kg/cm² contact stress during pinch
- 4 weeks immobilization, 6-12 months full recovery
References
-
Becker SJE, Makarawung DJS, Spit SA, et al. Disability in patients with trapeziometacarpal joint arthrosis: incidental versus presenting diagnosis. J Hand Surg Am. 2014;39(10):2009-2015. doi:10.1016/j.jhsa.2014.07.009
-
Wajon A, Vinycomb T, Carr E, et al. Surgery for thumb (trapeziometacarpal joint) osteoarthritis. Cochrane Database Syst Rev. 2015;2015(2):CD004631. doi:10.1002/14651858.CD004631.pub4
-
Eaton RG, Littler JW. Ligament reconstruction for the painful thumb carpometacarpal joint. J Bone Joint Surg Am. 1973;55(8):1655-1666.
-
Bettinger PC, Linscheid RL, Berger RA, et al. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg Am. 1999;24(4):786-798. doi:10.1053/jhsu.1999.0786
-
Pellegrini VD Jr. Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration. I. Anatomy and pathology of the aging joint. J Hand Surg Am. 1991;16(6):967-974.
-
Vermeulen GM, Slijper H, Feitz R, et al. Surgical management of primary thumb carpometacarpal osteoarthritis: a systematic review. J Hand Surg Am. 2011;36(1):157-169. doi:10.1016/j.jhsa.2010.10.028
-
Salem H, Davis TR. Six year outcome excision of the trapezium for trapeziometacarpal joint osteoarthritis: is it improved by ligament reconstruction and temporary Kirschner wire insertion? J Hand Surg Eur Vol. 2012;37(3):211-219. doi:10.1177/1753193411414518
-
Huang K, Hollevoet N, Giddins G. Thumb carpometacarpal joint total arthroplasty: a systematic review. J Hand Surg Eur Vol. 2015;40(4):338-350. doi:10.1177/1753193414563243
-
Vitale MA, Hettinger RM, O'Connor JP, et al. Trapeziometacarpal arthroplasty. J Am Acad Orthop Surg. 2016;24(8):555-562. doi:10.5435/JAAOS-D-15-00266
-
Gottschalk MB, Carpenter E, Oakes D, et al. Thumb carpometacarpal arthrodesis for arthritis: patient-reported outcomes and satisfaction at greater than 5-year follow-up. J Hand Surg Am. 2018;43(9):815-821. doi:10.1016/j.jhsa.2018.05.012
-
Burton RI, Pellegrini VD Jr. Surgical management of basal joint arthritis of the thumb. Part II. Ligament reconstruction with tendon interposition arthroplasty. J Hand Surg Am. 1986;11(3):324-332.
-
Forestier E, Vidoni E, Corain M, et al. Radiographic progression in thumb base osteoarthritis: a follow-up study. Clin Exp Rheumatol. 2018;36(6):1059-1064.
-
Marks M, Hensler S, Wehrli M, et al. Trapeziectomy with suspension-interposition arthroplasty for thumb carpometacarpal osteoarthritis: a randomized controlled trial comparing the use of allograft versus flexor carpi radialis tendon. J Hand Surg Am. 2017;42(12):978-986. doi:10.1016/j.jhsa.2017.07.004
-
Spekreijse KR, Vermeulen GM, Kedilioglu MA, et al. The effect of a bone tunnel during ligament reconstruction for trapeziometacarpal osteoarthritis: a 5-year follow-up. J Hand Surg Am. 2013;38(4):690-696. doi:10.1016/j.jhsa.2013.01.023
-
Marks M, Audigé L, Herren DB, et al. Trapeziometacarpal joint implant arthroplasty outcomes and approach-related complications: a systematic review. J Hand Surg Eur Vol. 2014;39(9):927-938. doi:10.1177/1753193413511936
-
Gangopadhyay S, McKenna H, Burke FD, et al. Five- to 18-year follow-up for treatment of trapeziometacarpal osteoarthritis: a prospective comparison of excision, tendon interposition, and ligament reconstruction and tendon interposition. J Hand Surg Am. 2012;37(3):411-417. doi:10.1016/j.jhsa.2011.11.027
-
Davis TR, Brady O, Dias JJ. Excision of the trapezium for osteoarthritis of the trapeziometacarpal joint: a study of the benefit of ligament reconstruction or tendon interposition. J Hand Surg Am. 2004;29(6):1069-1077. doi:10.1016/j.jhsa.2004.06.017
-
Hartigan BJ, Stern PJ, Kiefhaber TR. Thumb carpometacarpal osteoarthritis: arthrodesis compared with ligament reconstruction and tendon interposition. J Bone Joint Surg Am. 2001;83(10):1470-1478.
-
Spaans AJ, van Laarhoven CM, Schuurman AH, et al. Interobserver agreement of the Eaton-Littler classification system and treatment strategy of thumb carpometacarpal joint osteoarthritis. J Hand Surg Am. 2011;36(9):1467-1470. doi:10.1016/j.jhsa.2011.06.017
-
Raven EE, Haverkamp D, Sierevelt IN, et al. Long-term results of surgical intervention for osteoarthritis of the trapeziometacarpal joint: comparison of resection arthroplasty, trapeziectomy with tendon interposition and trapezio-metacarpal arthrodesis. Int Orthop. 2007;31(4):547-554. doi:10.1007/s00264-006-0224-5