Congenital Underdevelopment of the Thumb
- Blauth Classification: Types I-V based on thumb development (I mild to V absent).
- Type IIIB or Higher: Absolute indication for pollicization (unstable CMC joint).
- TAR Syndrome: Thrombocytopenia-Absent Radius - thumbs are PRESENT (vs radial club hand).
- Fanconi Anemia: Must screen with chromosome breakage test - bone marrow failure risk.
- Pollicization: Transfer index finger to thumb position - Buck-Gramcko technique gold standard.
- “Blauth IIIB = pollicization (unstable CMC)
- “TAR = thumbs present, radii absent
- “Screen for Fanconi with chromosome breakage
- “Pollicization at 12-18 months optimal
- “Four-flap Z-plasty for web space deepening
Absolute: Blauth IIIB, IV, V (unstable or absent CMC joint). IIIA is controversial - depends on stability, thenar function, patient/family preference. If CMC unstable or thenar absent with poor grip, pollicize.
TAR Syndrome: Thrombocytopenia + Absent Radius, but thumbs are PRESENT. Check platelets before surgery. Radial Club Hand: Radius absent AND thumb hypoplastic/absent.
Must perform chromosome breakage test (DEB or MMC) for all radial dysplasia cases. Fanconi patients develop bone marrow failure, leukemia, and solid tumors - requires hematology follow-up.
Optimal: 12-18 months (before pinch development). Acceptable: 6 months to 3 years. Earlier surgery preserves cortical reorganization. Late pollicization (older than 5 years) has poorer outcomes.
Overview and Epidemiology
Thumb hypoplasia is congenital underdevelopment of the thumb, ranging from mild hypoplasia to complete absence (aplasia). It represents a spectrum of deficiency affecting bones, joints, muscles, tendons, nerves, and vessels.
Epidemiology
- Incidence: Approximately 1 per 100,000 live births
- Bilateral: 60% of cases are bilateral
- Associated Syndromes: 60-70% have associated anomalies
- Gender: Equal male-to-female ratio
- Inheritance: Usually sporadic, occasionally autosomal dominant
Associated Conditions
Radial Longitudinal Deficiency
- Often part of radial dysplasia spectrum
- Can range from hypoplastic radius to complete radial aplasia
- Radial club hand deformity common
Thrombocytopenia-Absent Radius (TAR) Syndrome
- Thrombocytopenia with bilateral absent radii
- KEY FEATURE: Thumbs are PRESENT (differentiates from radial club hand)
- Must check platelet count before any surgery
- Autosomal recessive inheritance
Fanconi Anemia
- Progressive bone marrow failure
- Increased cancer risk (leukemia, solid tumors)
- MUST screen with chromosome breakage test (DEB or MMC test)
- Radial dysplasia with thumb hypoplasia
- Short stature, café-au-lait spots, renal anomalies
VACTERL Association
- Vertebral anomalies
- Anal atresia
- Cardiac defects
- Tracheo-Esophageal fistula
- Renal anomalies
- Limb defects (radial ray including thumb)
Holt-Oram Syndrome
- Cardiac septal defects (ASD, VSD)
- Upper limb radial ray deficiency
- Autosomal dominant (TBX5 gene mutation)
Other Associations
- Diamond-Blackfan anemia
- Aase syndrome
- Nager syndrome
- Maternal diabetes
Embryology
- Develops during limb bud formation at 4-8 weeks gestation
- Radial ray formation controlled by AER (Apical Ectodermal Ridge) and ZPA (Zone of Polarizing Activity)
- Disruption of FGF and Sonic Hedgehog (SHH) signaling pathways
- Results in spectrum from mild hypoplasia to complete absence
Anatomy
- First metacarpal (shorter, wider than digital metacarpals)
- Trapezium-MC1 joint (CMC - saddle joint for opposition)
- MP joint (condylar with sesamoids)
- IP joint (hinge joint)
- Proximal and distal phalanges
CMC saddle joint allows opposition movement
Thenar Eminence:
- APB (Abductor pollicis brevis): Abduction, median nerve
- FPB (Flexor pollicis brevis): Flexion at MP, median/ulnar
- OP (Opponens pollicis): Opposition, median nerve
- AdP (Adductor pollicis): Adduction, ulnar nerve
Type II hypoplasia: Thenar muscles absent
Extrinsic Function:
- FPL: Flexion of IP joint (AIN branch of median)
- EPL: Extension of IP joint (PIN branch of radial)
- EPB: Extension of MP joint (PIN)
- APL: Abduction at CMC (PIN)
Type III hypoplasia: Extrinsics absent/hypoplastic
Vascular Anatomy:
- Princeps pollicis artery (from radial artery)
- Digital arteries to both sides
- Dorsal network from first dorsal metacarpal artery
Pollicization: Radial digital artery of index becomes dominant
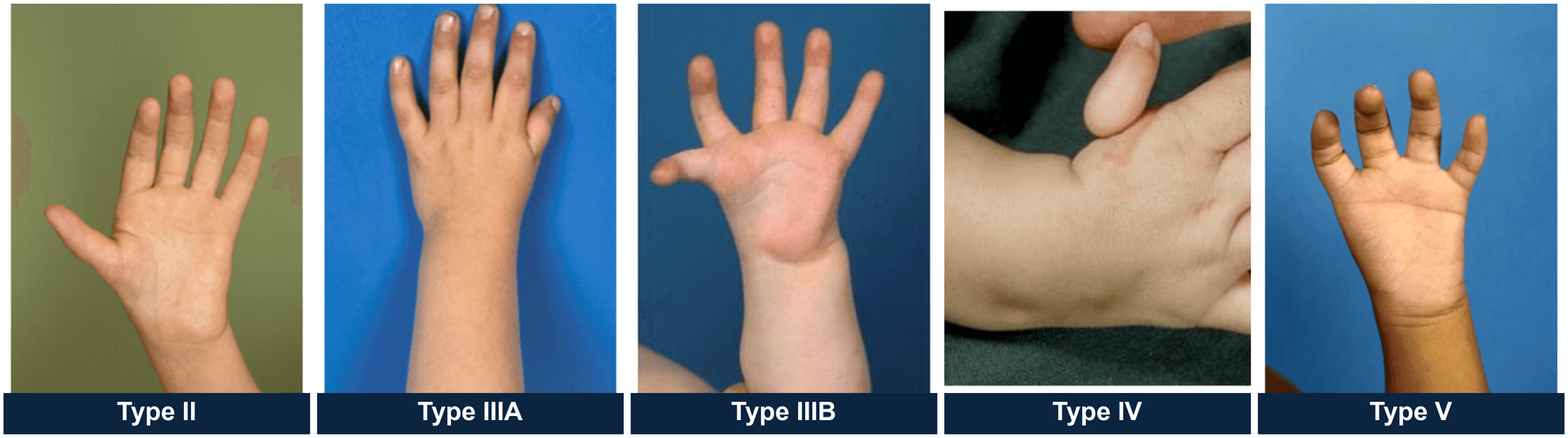
Blauth Classification System
The Blauth classification (Types I-V) is the gold standard for categorizing thumb hypoplasia severity and guiding treatment. It is based on degree of skeletal and soft tissue development.
Type I: Minor Generalized Hypoplasia
- All structures present but smaller than normal
- Stable CMC and MP joints
- Thenar muscles present but hypoplastic
- First web space adequate
- Opponensplasty (if thenar weak)
- Thumb augmentation procedures
- Conservative management often acceptable
Type II: Absence of Intrinsic Thenar Muscles
- Thenar muscles absent (APB, FPB, OP)
- First web space narrowed (adduction contracture)
- Ulnar collateral ligament of MP joint lax/absent
- CMC joint stable
- Extrinsic muscles (FPL, EPL) present
- Opponensplasty (FDS, ADM, or ECRL transfer)
- First web space deepening (four-flap Z-plasty)
- UCL reconstruction at MP joint (if unstable)
- Consider skeletal augmentation if severely hypoplastic
Type III: Extrinsic Muscle and Thenar Muscle Deficiency
DIVIDED INTO IIIA AND IIIB - critical distinction for treatment:
Type IIIA: Stable CMC Joint
- Extrinsic tendons (FPL, EPL) absent or hypoplastic
- Thenar muscles absent
- Metacarpal present and CMC joint stable
- First web space severely narrowed
Treatment: CONTROVERSIAL
- Reconstruction option: Opponensplasty, web deepening, tendon transfers, possible metacarpal lengthening
- Pollicization option: More predictable functional outcome
- Decision based on: CMC stability, metacarpal quality, family preference, surgeon experience
Type IIIB: Unstable CMC Joint
- Partial/hypoplastic metacarpal
- CMC joint unstable or subluxated
- Extrinsic and intrinsic muscles absent/severely deficient
Treatment: POLLICIZATION (absolute indication)
Type IV: Pouce Flottant (Floating Thumb)
- Only rudimentary proximal phalanx present (floating on soft tissue)
- No metacarpal or minimal nubbin
- No functional muscles
- Attached by narrow skin bridge
- Pollicization (absolute indication)
- May ablate rudimentary thumb before pollicization
Type V: Absence (Aplasia)
- Complete absence of thumb
- No skeletal or muscular structures
- Pollicization (absolute indication)
Classification
Blauth Classification Summary
- Key Feature
- Minor generalized hypoplasia
- CMC Joint
- Stable
- Treatment
- Opponensplasty if weak
- Key Feature
- Absent thenar, narrow web
- CMC Joint
- Stable
- Treatment
- Opponensplasty + web deepening
- Key Feature
- Absent extrinsics, stable CMC
- CMC Joint
- STABLE
- Treatment
- Controversial - reconstruct vs pollicize
- Key Feature
- Absent extrinsics, unstable CMC
- CMC Joint
- UNSTABLE
- Treatment
- Pollicization (absolute)
- Key Feature
- Pouce flottant (floating)
- CMC Joint
- Absent
- Treatment
- Pollicization (absolute)
- Key Feature
- Complete aplasia
- CMC Joint
- Absent
- Treatment
- Pollicization (absolute)
Key Decision: CMC stability determines IIIA vs IIIB and treatment approach
Clinical Assessment
History
Birth and Developmental History
- Maternal diabetes, teratogen exposure
- Developmental milestones
- Hand dominance (if old enough)
Family History
- Similar anomalies in family members
- Autosomal dominant inheritance patterns
Functional Assessment
- Current hand use and grip patterns
- Activities of daily living affected
- Pinch function
Systemic Review
- Cardiac symptoms (Holt-Oram)
- GI issues (VACTERL)
- Hematologic symptoms - bruising, petechiae (TAR, Fanconi)
- Renal issues
Physical Examination
General Inspection
- Bilateral assessment (60% bilateral)
- Overall hand size and proportions
- Forearm - assess for radial club hand deformity
- Elbow - assess for radial head dislocation
Thumb Examination
- Size: Length and width compared to contralateral
- First web space: Depth and width (adduction contracture)
- CMC joint: Stability testing - critical for Blauth classification
- MP joint: Stability, UCL integrity
- IP joint: Presence, stability
Muscle Assessment
- Thenar bulk: APB, FPB, opponens pollicis (Type II has absent thenar)
- Opposition: Ability to oppose thumb to small finger
- FPL function: Active IP flexion
- EPL function: Active IP/MP extension
Vascular Examination
- Capillary refill in thumb
- Allen test (assess radial/ulnar artery dominance)
- Digital artery presence (critical for pollicization planning)
Neurologic Examination
- Median nerve sensation
- Two-point discrimination
Associated Findings
- Radial dysplasia/club hand
- Syndactyly
- Polydactyly
- Other limb anomalies
Special Tests
CMC Joint Stability (Critical for IIIA vs IIIB)
- Stress testing of CMC joint
- Assess for subluxation/dislocation
- Fluoroscopy if uncertain
Pinch Force Measurement
- Compared to contralateral side
- Functional assessment
Investigations
Imaging
Radiographs (AP and Lateral)
- Thumb bones: Assess metacarpal, phalanges
- CMC joint: Evaluate stability, articular surfaces
- Carpal bones: Scaphoid, trapezium development
- Radius: Assess for radial dysplasia
- Forearm: Radial length, radial head dislocation
MRI (Selected Cases)
- Assessment of thenar and extrinsic muscles
- CMC joint cartilage and stability
- Vascular anatomy for pollicization planning
Ultrasound
- Vascular mapping (radial digital artery of index)
- Thenar muscle bulk assessment
Laboratory Investigations (Rule Out Syndromes)
Complete Blood Count
- Platelets: Rule out TAR syndrome (thrombocytopenia)
- Hemoglobin: Assess for Fanconi, Diamond-Blackfan anemia
Chromosome Breakage Test
- DEB (diepoxybutane) or MMC (mitomycin C) test
- MANDATORY for all radial dysplasia cases to rule out Fanconi anemia
- Fanconi cells show increased chromosomal breaks with exposure
Genetic Testing
- TBX5 gene (Holt-Oram syndrome)
- RBM8A/FAAP gene (TAR syndrome)
- Fanconi gene panel (FANC genes)
Other Investigations
Echocardiography
- Rule out cardiac defects (Holt-Oram, VACTERL)
- Especially if murmur present
Renal Ultrasound
- Assess for renal anomalies (VACTERL, Fanconi)
Spine Radiographs
- Vertebral anomalies (VACTERL)
Differential Diagnosis
- Key Distinguishing Feature
- Underdeveloped or absent thumb; assess CMC stability
- Classification
- Blauth I-V
- Treatment Direction
- Reconstruct (I-IIIA) vs pollicise (IIIB-V)
- Key Distinguishing Feature
- Extra rather than deficient thumb
- Classification
- Wassel-Flatt
- Treatment Direction
- Excise/combine less dominant component
- Key Distinguishing Feature
- Extra (third) phalanx, longer in-line thumb
- Classification
- Wood / opposability-based
- Treatment Direction
- Phalanx excision or delta correction
- Key Distinguishing Feature
- Fixed IP flexion with Notta node; thumb normally formed
- Classification
- Sling/Dinham
- Treatment Direction
- A1 pulley release if persistent
- Key Distinguishing Feature
- Thumb-in-palm from absent/weak EPL-EPB
- Classification
- Tsuyuguchi/McCarroll
- Treatment Direction
- Splinting then tendon transfer
- Key Distinguishing Feature
- Multiple joint contractures, other limbs involved
- Classification
- Part of amyoplasia spectrum
- Treatment Direction
- Release, transfers, web reconstruction
- Key Distinguishing Feature
- Short/webbed digits, often nubbins; usually sporadic
- Classification
- Blauth-Gekeler
- Treatment Direction
- Distraction, transfers, web release
Conditions to Differentiate from Thumb Hypoplasia
Thumb Duplication (Polydactyly)
- Extra thumb rather than underdeveloped thumb
- Wassel classification
- Treatment: Excision of less functional duplicate
Trigger Thumb (Congenital)
- Flexion contracture of IP joint
- Notta's node palpable
- Usually not associated with hypoplasia
- Treatment: Release of A1 pulley
Thumb Clasped Thumb Deformity
- Thumb held in palm (adduction and flexion)
- EPL and EPB deficiency or absence
- Treatment: Splinting, tendon transfers if persistent
Radial Polydactyly with Hypoplastic Components
- Combination of duplication and hypoplasia
- Both thumbs may be hypoplastic
- May require Bilhaut-Cloquet procedure (combine two hypoplastic thumbs)
Arthrogryposis with Thumb Involvement
- Multiple joint contractures
- Thumb-in-palm deformity
- Other limb involvement
Symbrachydactyly
- Short, webbed digits
- Can involve thumb
- Usually sporadic
Management Algorithm

Treatment decision based on Blauth classification, CMC stability, and functional requirements.
Conservative Management
Observation Only
- Mild Type I with good function
- Bilateral cases where pollicization timing differs
Adaptive Strategies
- Occupational therapy
- Adaptive equipment for ADLs
- Side-to-side pinch patterns
Surgical Management Overview
Reconstruction Indications (Types I, II, IIIA)
- CMC joint stable
- Metacarpal present with reasonable quality
- Family preference for maintaining thumb appearance
Pollicization Indications (Types IIIB, IV, V)
- ABSOLUTE: Blauth IIIB (unstable CMC), IV (pouce flottant), V (aplasia)
- RELATIVE: Blauth IIIA with poor metacarpal quality, absent extrinsics, family preference
Surgical Timing
Optimal Window: 12-18 months
- Rationale: Before development of cortical representation for pinch (occurs around 18-24 months)
- Brain plasticity allows cortical reorganization - index finger cortical area becomes thumb area
- Early enough to not delay hand function development
Acceptable Range: 6 months to 3 years
- Earlier (6-12 months): Smaller structures, technically demanding
- Later (greater than 3 years): Poorer outcomes, less cortical plasticity
Late Pollicization (older than 5 years)
- Less optimal outcomes
- Poor cortical reorganization
- Consider if diagnosis delayed or family previously declined
Surgical Techniques
Opponensplasty for Types I-II
Indications:
- Absent or weak thenar muscles
- Stable CMC joint
- Adequate thumb skeletal structure
Opponensplasty Options:
1. FDS Ring Finger Transfer (Most Common)
- FDS ring finger harvested at A1 pulley
- Passed around ulnar border of hand
- Attached to APB insertion (radial base of proximal phalanx)
- Provides opposition vector
2. ADM Transfer (Huber Transfer)
- Abductor digiti minimi transferred to thumb
- Neurovascular pedicle preserved
- Good for opposition and first web abduction
3. ECRL Transfer
- Used when FDS or ADM not suitable
- Routed through interosseous membrane or around FCU
- Attached to APB insertion
Technique (FDS Opponensplasty):
- Harvest FDS ring finger at A1 pulley (preserve A2)
- Pass through window at ulnar wrist (volar to FCU)
- Subcutaneous tunnel to thumb
- Attach to radial base of proximal phalanx at APB insertion
- Tension: Thumb in full opposition with wrist neutral
First Web Deepening
- Narrow first web space (adduction contracture)
- Types II and III
- Design two opposing Z-plasties on dorsal and volar surfaces
- 60-degree angles for maximum lengthening
- Raise full-thickness skin flaps
- Transpose flaps to deepen web
- May need skin graft for closure if severe contracture
Alternative: Dorsal Rotation Flap
- Large dorsal flap rotated into web space
- Skin graft to donor site
UCL Reconstruction (Type II)
Lax or absent UCL at MP joint
- Harvest palmaris longus or plantaris tendon
- Bone tunnels in proximal phalanx and metacarpal
- Weave graft in figure-of-8 pattern
- Tension with thumb in slight radial deviation
Thumb Augmentation
- Hypoplastic metacarpal or proximal phalanx (Types I-II)
- Bone grafting to metacarpal
- Distraction lengthening (rarely used)
- On-top plasty (transfer of great toe to thumb) - for older patients with late presentation
Pollicization needs a satisfactory index; when there is no usable index (it is absent, destroyed, or has already been used) or in the older child/adult who presents late or declines pollicization, a free microvascular toe-to-hand transfer reconstructs the thumb. The second toe is the usual donor (it sacrifices less of the foot and leaves a more acceptable donor site, although the great or "trimmed great toe" gives a bulkier, more thumb-like digit); the transferred toe brings its own nail, joints, tendons, neurovascular bundles and — in a child — an open physis so it continues to grow. It is technically demanding free tissue transfer (microvascular anastomosis to the radial artery and a dorsal vein, with nerve coaptation for sensation) carrying flap-failure and donor-foot-morbidity risks, and the reconstructed digit is weaker and less mobile than a pollicized index. For that reason pollicization remains first choice in the young child with a usable index, and toe transfer is reserved for the no-index situation. This is distinct from an on-top plasty, which transposes local tissue rather than a free vascularized toe.
This completes the reconstruction techniques section.
Associated Syndromes - Detailed
TAR Syndrome (Thrombocytopenia-Absent Radius)
KEY FEATURE: Radii absent but thumbs PRESENT - differentiates from typical radial club hand.
- Bilateral radial aplasia
- Thrombocytopenia (low platelets, usually less than 50,000)
- Thumbs present (may be hypoplastic but always present)
- Often associated with cow's milk allergy
- Cardiac anomalies in 30%
- Compound inheritance: RBM8A gene deletion PLUS modifier allele
- Autosomal recessive pattern
- Check platelet count BEFORE any surgery
- Transfuse platelets if less than 50,000 for surgery
- Thrombocytopenia usually improves after age 1 year
- Radial club hand requires centralization
- Thumbs usually do NOT require pollicization (present and functional)
Fanconi Anemia
CRITICAL: Must screen all radial dysplasia patients with chromosome breakage test.
- Progressive bone marrow failure (aplastic anemia)
- Radial ray abnormalities (radial dysplasia, thumb hypoplasia/aplasia)
- Short stature
- Café-au-lait spots, hyperpigmentation
- Renal anomalies (horseshoe kidney, renal agenesis)
- Microcephaly, developmental delay
- Increased cancer risk (AML, head/neck SCC)
- Autosomal recessive (most common)
- Over 20 FANC genes identified
- DNA repair defect
- Chromosome breakage test: DEB (diepoxybutane) or MMC (mitomycin C)
- Fanconi cells show increased chromosomal breaks and rearrangements when exposed to DNA crosslinking agents
- Genetic testing for FANC gene mutations
- Hematology follow-up for bone marrow function
- Monitor for malignancy
- Orthopedic surgery timing coordinated with hematologist
- Bone marrow transplant may be needed
- Genetic counseling
- Can proceed with pollicization/reconstruction if blood counts adequate
- Increased bleeding risk if thrombocytopenic
- Long-term cancer surveillance
VACTERL Association
- Vertebral anomalies (hemivertebrae, scoliosis)
- Anal atresia/imperforate anus
- Cardiac defects (VSD, ASD, TOF)
- Tracheo-Esophageal fistula/esophageal atresia
- Renal anomalies (agenesis, dysplasia, hydronephrosis)
- Limb abnormalities (radial dysplasia, thumb hypoplasia)
- At least 3 components required
- Non-random association (not a syndrome, no single genetic cause)
- Spine X-rays
- Echocardiography
- Renal ultrasound
- GI evaluation if feeding difficulties
- Thumb reconstruction/pollicization as per Blauth classification
- Scoliosis monitoring and treatment if needed
Holt-Oram Syndrome
- Upper limb radial ray deficiency (thumb hypoplasia/aplasia to phocomelia)
- Cardiac septal defects (ASD, VSD) - present in 75%
- Conduction abnormalities (first-degree AV block)
- Autosomal dominant
- TBX5 gene mutation (transcription factor important for heart and limb development)
- Variable expressivity
- Echocardiography mandatory
- ECG (may show AV block)
- Cardiology clearance before surgery
- Pollicization as indicated
- Cardiac status may affect surgical timing
Other Associations
Diamond-Blackfan Anemia
- Congenital red cell aplasia
- Thumb hypoplasia, radial dysplasia
- Short stature, craniofacial anomalies
Aase Syndrome
- Hypoplastic anemia
- Triphalangeal thumbs
- Cleft palate, narrow shoulders
Nager Syndrome (Acrofacial Dysostosis)
- Mandibular hypoplasia
- Radial ray deficiency
- Thumb hypoplasia/aplasia
Complications
Complication Summary
- Vascular compromise (less than 1%): MOST SERIOUS - immediate re-exploration
- Web space contracture (10-15%): Revision Z-plasty
- Malposition (5-10%): Revision osteotomy if severe
- Tendon imbalance: Revision tendon work
- Under/over-tensioned opponensplasty
- Web contracture recurrence
- Persistent UCL instability
Postoperative Care
Postoperative Protocol
- Long arm thumb spica cast: 4-6 weeks
- K-wire removal: 4-6 weeks
- Vascular monitoring: First 48 hours critical
- Passive ROM: 6 weeks post-op
- Active ROM: 8 weeks post-op
- Short arm splint: 4 weeks
- Opponensplasty protection: 6 weeks
- Therapy: Active ROM at 4-6 weeks
Outcomes
Outcome Summary
- Opposition achieved: greater than 90%
- Pinch strength: 50-75% of normal
- Grasp function: Excellent
- Cosmetic acceptance: High (especially if early)
- Opponensplasty success: 80-90%
- Web space maintained: 80-90%
- May require revision procedures
Guidelines, Registries & Global Practice
Global Epidemiology
Thumb hypoplasia and aplasia sit within radial longitudinal deficiency, the commonest congenital longitudinal deficiency of the upper limb. Severity of the thumb deficiency rises in lockstep with the severity of the radial deficiency, a relationship confirmed both in historical cohorts and in contemporary multicentre registry data (James 2004, PMID 15466728; Forman/CoULD 2020, PMID 33086350). Roughly one-third of patients carry a recognised syndrome, and registry data show syndromic children are twice as likely to be bilateral and 2.5 times more likely to have combined radial and thumb involvement.
- Region / Body
- Global
- Role
- Grades thumb severity I-V and drives reconstruct-vs-pollicise decision
- Status
- Universal standard
- Region / Body
- IFSSH-endorsed
- Role
- Dysmorphology-based classification of all congenital hand anomalies
- Status
- Current IFSSH system
- Region / Body
- Global
- Role
- Grades associated radial longitudinal deficiency
- Status
- Standard for radius
- Region / Body
- USA, multicentre
- Role
- Prospective outcome / complication benchmarking
- Status
- Largest active registry
Guidance & Practice Consensus
There is no randomised-trial-level guideline for this rare condition; international practice is built on case series, registry data and society consensus rather than graded recommendations. Bodies such as the IFSSH (classification), ASSH and BSSH (paediatric hand standards) and AAOS instructional material converge on the same operative principles.
- Consensus Position
- Reconstruct stable Blauth I-IIIA; pollicise unstable IIIB-V
- Evidence / Variation
- Consensus on CMC stability as the threshold (Manske/McCarroll, PMID 1572922)
- Consensus Position
- Buck-Gramcko index pollicisation is the global standard
- Evidence / Variation
- Original series PMID 5121802; minor regional technical modifications
- Consensus Position
- Most centres operate at 12-18 months
- Evidence / Variation
- Range 6 months-3 years; expert opinion, not trial-based
- Consensus Position
- Chromosome breakage (DEB/MMC) for all radial-ray cases
- Evidence / Variation
- Strongly supported (Esmer, PMID 14679584); variably applied in practice
- Consensus Position
- Increasingly favours pollicisation when extrinsics/FPL absent
- Evidence / Variation
- Genuine practice variation; shared decision-making essential
Registry Evidence & Complication Benchmarks
The CoULD registry provides the most robust contemporary outcome data. Across 2,430 congenital upper-limb procedures the overall complication rate was 5.3% (4.1% excluding trivial events), with thumb deficiency surgery among the higher-complication groups and post-pollicisation vascular compromise among the most severe events (Bae/CoULD 2026, PMID 41500756). No reliable patient-level risk factors were identified, underscoring that complications are multifactorial.
Multidisciplinary tertiary care integrating hand surgery, clinical genetics and haematology enables comprehensive syndrome screening including mandatory chromosome-breakage testing; early referral by 3-6 months allows assessment and planning within the optimal 12-18 month surgical window.
MCQ Practice Points
Q: What is the Blauth classification for thumb hypoplasia and which types require pollicization?
A: Blauth classification (modified by Manske/McCarroll): Type I: Minor hypoplasia, all structures present; Type II: Intrinsic muscle hypoplasia, first web space narrowing, UCL instability; Type IIIA: Type II + extrinsic tendon abnormalities, stable CMC joint; Type IIIB: Type III + unstable CMC joint (global proximal deficiency); Type IV: Floating thumb (pouce flottant); Type V: Absent thumb. Pollicization indicated for Types IIIB, IV, and V - reconstructing an unstable or floating thumb yields inferior results to pollicization.
Q: What is the critical distinction between Blauth Type IIIA and Type IIIB thumb hypoplasia?
A: The critical distinction is CMC joint stability. Type IIIA: CMC joint is stable (basal joint elements intact) - amenable to reconstruction (opponensplasty, tendon transfers, first web release). Type IIIB: CMC joint is unstable (deficient trapezium, metacarpal base) - reconstruction gives poor results, pollicization preferred. Clinical assessment: passively stress the CMC joint; radiographs may show hypoplastic trapezium. This distinction is crucial for surgical planning - Type IIIB represents a threshold below which pollicization gives superior functional outcomes.
Q: What is pollicization and what are the key technical principles?
A: Pollicization converts the index finger into a thumb. Key principles: 1) Shorten and rotate index metacarpal approximately 160 degrees into pronation; 2) Position in palmar abduction and opposition; 3) Transfer intrinsics to recreate thenar function (first dorsal interosseous becomes APB, first palmar interosseous becomes adductor); 4) Preserve neurovascular bundles; 5) Close first web space primarily. Optimal timing is 12-18 months of age. The index finger never achieves normal thumb strength but provides excellent pinch and grasp function.
Q: What conditions are associated with thumb hypoplasia?
A: Thumb hypoplasia is commonly associated with: Radial longitudinal deficiency (radial club hand) - most common association; Holt-Oram syndrome (heart-hand syndrome - cardiac septal defects + radial ray deficiency); VACTERL association; Fanconi anemia (bone marrow failure, short stature); TAR syndrome (thrombocytopenia-absent radius - thumbs present); Trisomy 18. Isolated thumb hypoplasia also occurs. All patients require cardiac echocardiography, renal ultrasound, and hematology workup (CBC, chromosomal breakage studies for Fanconi).
Q: What are the surgical options for Blauth Type II thumb hypoplasia?
A: Type II hypoplasia has all skeletal elements but deficient thenar muscles, first web narrowing, and UCL laxity. Surgical options: 1) First web space release/Z-plasty - address contracture; 2) Opponensplasty - restore opposition (Huber transfer using ADM, FDS ring finger transfer, EIP transfer); 3) UCL reconstruction - stabilize MCP joint; 4) FPL augmentation if weak. Surgery is typically staged: web release first, then tendon transfers after 6-12 months. Combination of procedures can achieve functional thumb with stable pinch.
At a Glance
Thumb hypoplasia is congenital underdevelopment ranging from mild hypoplasia to complete aplasia. The Blauth classification (I-V) guides treatment: Types I-II are reconstructable (opponensplasty, web deepening); Type IIIA is controversial; Types IIIB-V require pollicization (index-to-thumb transfer). The key decision point is CMC joint stability - if unstable or absent, pollicization is indicated. Often associated with syndromes: TAR syndrome (thrombocytopenia + absent radius, but thumbs PRESENT), Fanconi anemia (screen with chromosome breakage test), VACTERL, and Holt-Oram. Surgery at 12-18 months optimizes cortical reorganization and functional outcomes.
- Key Features
- Minor generalized hypoplasia
- CMC Joint
- Stable
- Thenar Muscles
- Present but weak
- Treatment
- Opponensplasty +/- augmentation
- Key Features
- Absent thenar, narrow web
- CMC Joint
- Stable
- Thenar Muscles
- Absent
- Treatment
- Opponensplasty + web deepening + UCL reconstruction
- Key Features
- Extrinsic deficiency, stable CMC
- CMC Joint
- Stable
- Thenar Muscles
- Absent
- Treatment
- CONTROVERSIAL - reconstruction vs pollicization
- Key Features
- Unstable CMC, partial MC
- CMC Joint
- UNSTABLE
- Thenar Muscles
- Absent
- Treatment
- POLLICIZATION
- Key Features
- Pouce flottant - proximal phalanx only
- CMC Joint
- Absent
- Thenar Muscles
- Absent
- Treatment
- POLLICIZATION
- Key Features
- Complete absence (aplasia)
- CMC Joint
- Absent
- Thenar Muscles
- Absent
- Treatment
- POLLICIZATION
BLAUTHBLAUTH Classification Memory
Hook:BLAUTH: Build up I-II, Ligaments stable in IIIA, Absent stability IIIB-V needs Hand swap (pollicization)
POLLICIZATIONPOLLICIZATION Surgical Steps
Hook:POLLICIZATION steps: Position, Osteotomy, preserve Ligaments, Lengthen extensors, Intrinsics reposition, Collaterals preserve, Index artery preserve, Z-plasty web, Alignment correct, Tenodesis balance
TARTAR Syndrome Recognition
Hook:TAR = Thrombocytopenia + Absent Radius + Retained thumbs (this distinguishes from radial club hand)
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 9-month-old child presents with bilateral thumb hypoplasia. On the right, there is a small thumb with absent thenar muscles, narrow web space, but stable CMC and MP joints. On the left, the thumb appears as a small nubbin attached by a skin bridge with no functional structures. How would you assess and manage this child?”
“You are performing a pollicization for a Blauth Type V thumb aplasia in an 18-month-old child. Walk me through your surgical technique, focusing on the key steps and critical structures to preserve.”
“A 14-month-old presents with Blauth Type IIIA thumb hypoplasia. The CMC joint is stable on stress testing, but the thumb is very small with absent thenar muscles and no FPL function. The family is concerned about their child having a four-fingered hand. How do you counsel them and what factors influence your decision between reconstruction and pollicization?”
Blauth Classification (CRITICAL)
- Type I: Minor hypoplasia, all structures present - OPPONENSPLASTY
- Type II: Absent thenar, narrow web, stable CMC/MP - RECONSTRUCTION
- Type IIIA: Stable CMC, absent extrinsics/intrinsics - CONTROVERSIAL
- Type IIIB: UNSTABLE CMC, partial MC - POLLICIZATION
- Type IV: Pouce flottant (floating, PP only) - POLLICIZATION
- Type V: Complete absence (aplasia) - POLLICIZATION
Key Decision Point: IIIA vs IIIB
- IIIA: Stable CMC - Reconstruct OR pollicize (controversial)
- IIIB: UNSTABLE CMC - Pollicize (absolute)
- Test CMC stability with stress testing, fluoroscopy if uncertain
- Absent FPL/EPL favors pollicization even if CMC stable
Associated Syndromes (Screen ALL cases)
- TAR: Thrombocytopenia + Absent Radius + thumbs PRESENT
- Fanconi: Radial dysplasia + Chromosome breakage test (DEB/MMC)
- VACTERL: Vertebral, Anal, Cardiac, TE fistula, Renal, Limb
- Holt-Oram: Cardiac septal defects + radial dysplasia (TBX5 gene)
- ALWAYS: CBC, chromosome breakage, echo, renal US
Pollicization Technique (Buck-Gramcko)
- Four-flap skin incision for web space Z-plasty
- Preserve radial digital artery of index (CRITICAL)
- Metacarpal neck wedge osteotomy: 20-30 deg for pronation
- Position: 140-160 deg abduction, 120-140 deg pronation
- First DI repositioned as thenar muscle (radial base PP)
- FDP becomes FPL, EDC/EIP become EPL/EPB
- Immobilize 4-6 weeks in thumb spica
Reconstruction Components (Type I-II)
- Opponensplasty: FDS ring (most common), ADM (Huber), or ECRL
- Web deepening: Four-flap Z-plasty (60-deg angles)
- UCL reconstruction: PL graft, figure-8 through bone tunnels
- Skeletal augmentation: Bone graft to MC if severely hypoplastic
Surgical Timing and Outcomes
- OPTIMAL: 12-18 months (before cortical pinch representation)
- Pollicization outcomes: Pinch 50-75% normal, opposition over 90%
- Satisfaction over 90%, cosmetic acceptance high if early
- Late pollicization (older than 5 years): poorer outcomes, less plasticity
Complications
- MOST SERIOUS: Vascular compromise - immediate re-exploration
- Web contracture 10-15% - revision Z-plasty
- Malposition 5-10% - may need revision osteotomy
- Opponensplasty: under-tensioning (weak) or over-tensioning (swan-neck)
Exam Traps
- TAR: Thumbs PRESENT (vs radial club hand: thumbs absent/hypoplastic)
- MUST screen Fanconi with chromosome breakage test (bone marrow failure)
- Type IIIB requires pollicization (UNSTABLE CMC is absolute indication)
- Pollicization timing: 12-18mo optimal (brain plasticity critical)
Evidence Base
Reconstruction of the Congenitally Deficient Thumb
- Operation is dictated by the type of hypoplasia present
- Type III thumbs are the most difficult decision-making group
- Pollicisation as a salvage after failed reconstruction is nearly impossible
- Parents must be counselled that secondary procedures are often required
Pollicization of the Index Finger: Method and Results in Aplasia and Hypoplasia of the Thumb
- Index metacarpal shortened and rotated into pronation with the head fixed to the base
- First dorsal interosseous repositioned to act as abductor pollicis brevis
- First palmar interosseous repositioned to act as adductor pollicis
- Digital neurovascular bundles preserved to maintain perfusion of the new thumb
The Association of Radial Deficiency with Thumb Hypoplasia
- Thumb deficiency severity directly proportional to radial deficiency severity (p value below 0.0001)
- Two-thirds (63/95) of limbs with a normal radius had a reconstructible thumb
- 48 of 51 limbs (94%) with complete radial absence had a non-reconstructible thumb
- Every limb with a radial and/or carpal deficiency also had a thumb deficiency
DEB Test for Fanconi Anaemia Detection in Patients with Atypical Phenotypes
- DEB hypersensitivity diagnoses Fanconi anaemia before pancytopenia develops
- Fanconi anaemia was detected among children presenting with radial-ray abnormalities alone
- Clinical phenotype alone is unreliable, so screening must be triggered by the limb anomaly
- Early diagnosis has major implications for the patient and at-risk family members
Association of Radial Longitudinal Deficiency and Thumb Hypoplasia: An Update Using the CoULD Registry
- Radial severity correlated with thumb severity (Kendall tau = 0.49)
- Patients with a syndrome were twice as likely to have bilateral deficiency
- Syndromic patients were 2.5 times more likely to have combined radial and thumb deficiency
- Holt-Oram, TAR and Fanconi anaemia showed distinct deficiency patterns versus VACTERL
Complications Following Congenital Hand and Upper Limb Surgery: Lessons from the CoULD Registry
- Overall complication rate 5.3% (4.1% excluding minor Clavien-Dindo I events)
- Vascular compromise after pollicisation was among the most severe complications recorded
- Thumb deficiency, syndactyly and polydactyly surgery carried the most complications
- No reliable patient-specific risk factors (syndrome, bilaterality, comorbidity) were identified
References
-
Blauth W. Der hypoplastische Daumen. Arch Orthop Unfall-Chir. 1967;62(3):225-246.
-
Buck-Gramcko D. Pollicization of the index finger: Method and results in aplasia and hypoplasia of the thumb. J Bone Joint Surg Am. 1971;53(8):1605-1617.
-
Manske PR, McCarroll HR Jr. Reconstruction of the congenitally deficient thumb. Hand Clin. 1992;8(1):177-196.
-
Goldfarb CA, Murtha YM, Gordon JE, et al. Developmental outcomes of the digits pollicized for congenital thumb hypoplasia. J Bone Joint Surg Am. 2006;88(2):279-287.
-
Cheng JC, Ng BK, Ying SY, Fung BK. A 10-year study of 300 cases of thumb hypoplasia. J Hand Surg Br. 1999;24(4):472-476.
-
Kozin SH. Pollicization: the concept, technical details, and outcome. Clin Orthop Surg. 2012;4(1):18-35.
-
Alter BP. Diagnosis, genetics, and management of inherited bone marrow failure syndromes. Hematology Am Soc Hematol Educ Program. 2007:29-39.
-
Greenhalgh DG, Warden GD, Moncrief JA, et al. The pollicization procedure: a review of 139 cases. J Hand Surg Am. 1993;18(1):4-12.
-
Light TR, Ogden JA. Congenital constriction band syndrome: pathophysiology and treatment. Yale J Biol Med. 1993;66(3):143-155.
-
James MA, Green HD, McCarroll HR Jr, Manske PR. The association of radial deficiency with thumb hypoplasia. J Bone Joint Surg Am. 2004;86(10):2196-2205.
-
Tonkin MA, Tolerton SK, Quick TJ, et al. Classification of congenital anomalies of the hand and upper limb: development and assessment of a new system. J Hand Surg Am. 2013;38(9):1845-1853.
-
Bayne LG, Klug MS. Long-term review of the surgical treatment of radial deficiencies. J Hand Surg Am. 1987;12(2):169-179.
-
McCarroll HR Jr. Congenital anomalies: a 25-year overview. J Hand Surg Am. 2000;25(6):1007-1037.
-
Netscher DT, Baumholtz MA. Treatment of congenital hypoplasia and absence of the thumb. Hand Clin. 2009;25(2):151-171.
-
Mih AD, Villareal-Rios A, Abrams RA, Hanel DP. Hypoplastic thumb. J Am Acad Orthop Surg. 2014;22(4):246-255.
-
Bae DS, Canizares MF, Miller PE, et al. Predictors of functional outcomes following index finger pollicization for congenital thumb hypoplasia. J Hand Surg Am. 2015;40(11):2227-2233.
-
Sammer DM, Chung KC. Congenital hand differences: embryology and classification. Hand Clin. 2009;25(2):151-171.
-
Staines KG, Majzoub R, Thornby J, Netscher DT. Functional outcomes following pollicization for treatment of thumb hypoplasia/aplasia. J Hand Surg Am. 2005;30(6):1201-1213.
-
Wang AA, Tan J, Leit ME. Thrombocytopenia-absent radius syndrome: a clinical review. J Pediatr Orthop. 2013;33(3):e27-e30.
-
Hosalkar HS, Shah MA, Yoon M, et al. Pollicization of the index finger for congenitally absent or hypoplastic thumb. Orthopedics. 2009;32(8):571-577.