Deformity Correction | CORA Concept | Osteotomy Techniques
- CORA (Center of Rotation of Angulation) = intersection of proximal and distal anatomic axes - osteotomy at CORA corrects angulation without translation
- Indications for correction: Angular deformity over 10-15°, rotational over 15-20°, shortening over 2cm, symptomatic, or predisposing to arthritis
- Closing wedge: Inherently stable, shortens limb (~2mm per degree per 10cm), best when shortening acceptable
- Opening wedge: Lengthens limb, preserves bone stock, requires bone graft if gap over 1cm, higher nonunion risk
- Dome osteotomy: Allows multiplanar correction, no length change, technically demanding
- “CORA = intersection of proximal and distal anatomic axes - osteotomy at CORA corrects angulation without translation
- “Closing wedge: 1° correction = 1.75mm wedge base per 10cm length, inherently stable, shortens limb
- “Opening wedge: Lengthens limb, requires graft if gap over 1cm, higher nonunion risk (10-15%)
- “Mechanical axis deviation (MAD) over 10mm is significant - normal passes through knee center
CORA (Center of Rotation of Angulation) = intersection of proximal and distal anatomic axes. Osteotomy AT the CORA corrects angulation without translation. Osteotomy AWAY from CORA creates translation deformity. Critical for planning.
Angular deformity over 10-15°, rotational over 15-20°, shortening over 2cm, symptomatic, or predisposing to arthritis - Mechanical axis deviation (MAD) over 10mm is significant. Normal mechanical axis passes through knee center.
Closing wedge: Inherently stable, shortens limb (~2mm per degree per 10cm). Opening wedge: Lengthens limb, requires graft if gap over 1cm. Dome: Multiplanar correction, no length change. Choose based on deformity and goals.
Full-length standing radiographs (mechanical axis), CT scan with 3D reconstruction (multiplanar deformity), rotation protocol (compare to contralateral). Calculate CORA, measure all deformity components (angulation, rotation, length, translation).
- Threshold
- Over 10-15°
- Treatment
- Osteotomy at CORA
- Outcome
- 85-90% good results
- Threshold
- Over 15-20°
- Treatment
- Derotational osteotomy
- Outcome
- 85-90% good results
- Threshold
- Over 2cm
- Treatment
- Lengthening osteotomy
- Outcome
- 80-85% good results
- Threshold
- Step-off over 2mm
- Treatment
- Intra-articular osteotomy
- Outcome
- 70-80% good results
Overview and Epidemiology
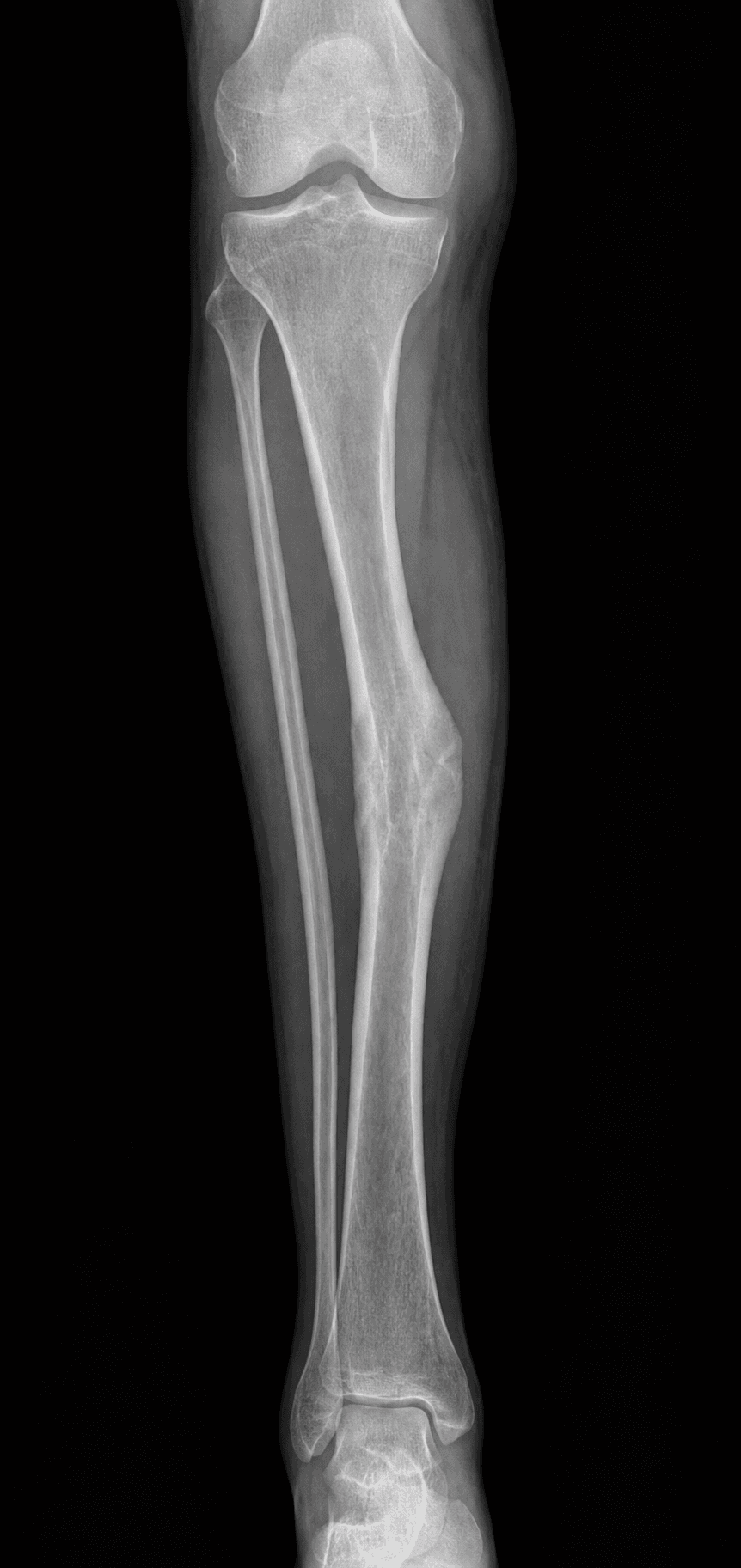
Tibial malunion occurs when a tibial fracture heals in a non-anatomic position, causing deformity, functional impairment, or predisposition to arthritis. Correction requires systematic evaluation, preoperative planning (including CORA calculation), and appropriate osteotomy technique.
Definition
Malunion: Fracture that has healed in a non-anatomic position, causing:
- Deformity: Angular, rotational, or shortening
- Functional impairment: Gait disturbance, joint dysfunction
- Predisposition to arthritis: Abnormal joint loading
Acceptable alignment (tibial shaft fractures):
- Varus/valgus: Under 5 degrees
- AP angulation: Under 10 degrees
- Rotation: Under 10 degrees
- Shortening: Under 10mm
Malunion thresholds (indications for correction):
- Angular: Over 10-15 degrees (causes mechanical axis deviation)
- Rotational: Over 15-20 degrees (causes functional impairment)
- Shortening: Over 2cm (causes gait asymmetry)
Q: What happens if you perform an osteotomy away from the CORA? A: Translation deformity occurs. Osteotomy AT the CORA corrects angulation without translation. Osteotomy AWAY from CORA creates translation deformity. Critical for preoperative planning.
Epidemiology
- Incidence: 5-10% of tibial shaft fractures develop malunion
- Location: Distal third most common (poor blood supply, difficult fixation)
- Age: Peak 20-40 years (high-energy trauma)
- Gender: Male predominance (2:1 ratio)
- Risk factors: High energy, open fracture, poor initial reduction, inadequate fixation
Anatomy and Pathophysiology
Mechanical Axis
Normal mechanical axis:
- Passes from center of femoral head through center of knee to center of ankle
- Should pass through knee center (medial to tibial spine)
- Deviation causes abnormal joint loading
Mechanical axis deviation (MAD):
- Normal: 0-10mm medial to knee center
- Significant: Over 10mm deviation
- Causes: Angular deformity, predisposes to arthritis
CORA Concept
Center of Rotation of Angulation (CORA):
- Definition: Intersection of proximal and distal anatomic axes
- Location: At apex of deformity
- Significance: Osteotomy at CORA corrects angulation without translation
- Calculation: Draw proximal and distal anatomic axes, identify intersection point
Osteotomy location:
- At CORA: Pure angular correction (no translation)
- Away from CORA: Creates translation deformity (undesirable)
- Planning: Use full-length standing radiographs to identify CORA
Pathophysiology
Angular malunion:
- Varus: Medial compartment overload, predisposes to arthritis
- Valgus: Lateral compartment overload, predisposes to arthritis
- Apex anterior: Knee hyperextension, gait disturbance
- Apex posterior: Knee flexion contracture, gait disturbance
Rotational malunion:
- Internal rotation: Foot progression angle abnormal, gait disturbance
- External rotation: Foot progression angle abnormal, gait disturbance
- Functional impact: Difficulty with activities requiring rotation
Shortening:
- Gait asymmetry: Compensatory mechanisms (pelvic tilt, equinus)
- Functional impact: Fatigue, back pain, joint overload
Classification Systems
Deformity-Based Classification
Angular malunion:
- Varus/valgus (frontal plane)
- Apex anterior/posterior (sagittal plane)
- Combined (multiplanar)
- Treatment: Osteotomy at CORA
Rotational malunion:
- Internal rotation
- External rotation
- Treatment: Derotational osteotomy
Shortening:
- Less than 2cm (usually acceptable)
- Over 2cm (may need correction)
- Treatment: Lengthening osteotomy or accept with shoe lift
Intra-articular malunion:
- Joint surface step-off
- Treatment: Intra-articular osteotomy (if early) or arthroplasty/arthrodesis (if established arthritis)
Deformity type determines treatment approach.
Clinical Assessment
History
Symptoms:
- Pain: Joint pain (knee or ankle), activity-related
- Functional impairment: Gait disturbance, difficulty with activities
- Deformity: Visible deformity, leg length discrepancy
- Previous fracture: History of tibial fracture, treatment method
Risk factors:
- High-energy trauma
- Open fracture
- Poor initial reduction
- Inadequate fixation
- Non-compliance with treatment
Physical Examination
Inspection:
- Deformity: Visible angulation, rotation, shortening
- Gait: Antalgic, Trendelenburg, equinus (if shortening)
- Alignment: Standing alignment, leg length discrepancy
Palpation:
- Tenderness at malunion site
- Deformity palpable
- Previous surgical scars
Range of Motion:
- Knee ROM (may be limited if proximal)
- Ankle ROM (may be limited if distal)
- Foot progression angle (rotational assessment)
Special tests:
- Mechanical axis: Standing alignment assessment
- Rotation: Compare to contralateral (knee flexed 90 degrees)
- Length: Block test, tape measure
Q: What deformity components must be assessed in tibial malunion? A: Angulation (frontal and sagittal planes), rotation (compare to contralateral with knee flexed 90°), shortening (block test), and translation. Use full-length standing radiographs and CT scan with rotation protocol for complete assessment.
Associated Conditions
- Post-traumatic arthritis: Joint degeneration from abnormal loading
- Limb length discrepancy: Functional impact
- Gait abnormalities: Compensatory mechanisms
Differential Diagnosis
The painful, deformed or symptomatic post-fracture lower leg is not always a malunion needing osteotomy. Distinguish the entities below before planning correction.
- Key feature
- Healed fracture in non-anatomic position; deformity stable
- Discriminating test
- Full-length standing films + CT (bone bridged, MAD measured)
- Implication
- Corrective osteotomy if symptomatic / mechanical
- Key feature
- Persistent pain, motion or lucency at fracture line
- Discriminating test
- No bridging callus on CT; tenderness on stressing site
- Implication
- Treat the nonunion (revision fixation, graft) first
- Key feature
- Joint-line pain, stiffness, joint-space loss
- Discriminating test
- Weight-bearing joint views show arthritis, not shaft deformity
- Implication
- Osteotomy alone insufficient - may need fusion / arthroplasty
- Key feature
- Pain, warmth, prior open injury or wound issue
- Discriminating test
- Raised CRP/ESR, sinus, MRI; consider biopsy
- Implication
- Eradicate infection before any reconstruction
- Key feature
- Pain over plate / prominent nail, no deformity
- Discriminating test
- Local tenderness over implant; alignment normal
- Implication
- Hardware removal, not osteotomy
- Key feature
- Radiographic malalignment but no symptoms
- Discriminating test
- Functional scores normal; MAD within knee
- Implication
- Observe - do not operate on the radiograph
Investigations
Standard X-ray Protocol
Full-length standing radiographs (essential):
- AP and lateral full-length (hip to ankle)
- Assess mechanical axis
- Measure angular deformity
- Assess limb length
Local views:
- AP and lateral tibia
- Assess malunion site
- Previous hardware
Key measurements:
- Mechanical axis deviation (MAD)
- Anatomic axis angles
- Limb length discrepancy
Full-length standing radiographs are essential for CORA calculation.
Management Algorithm
Management Pathway
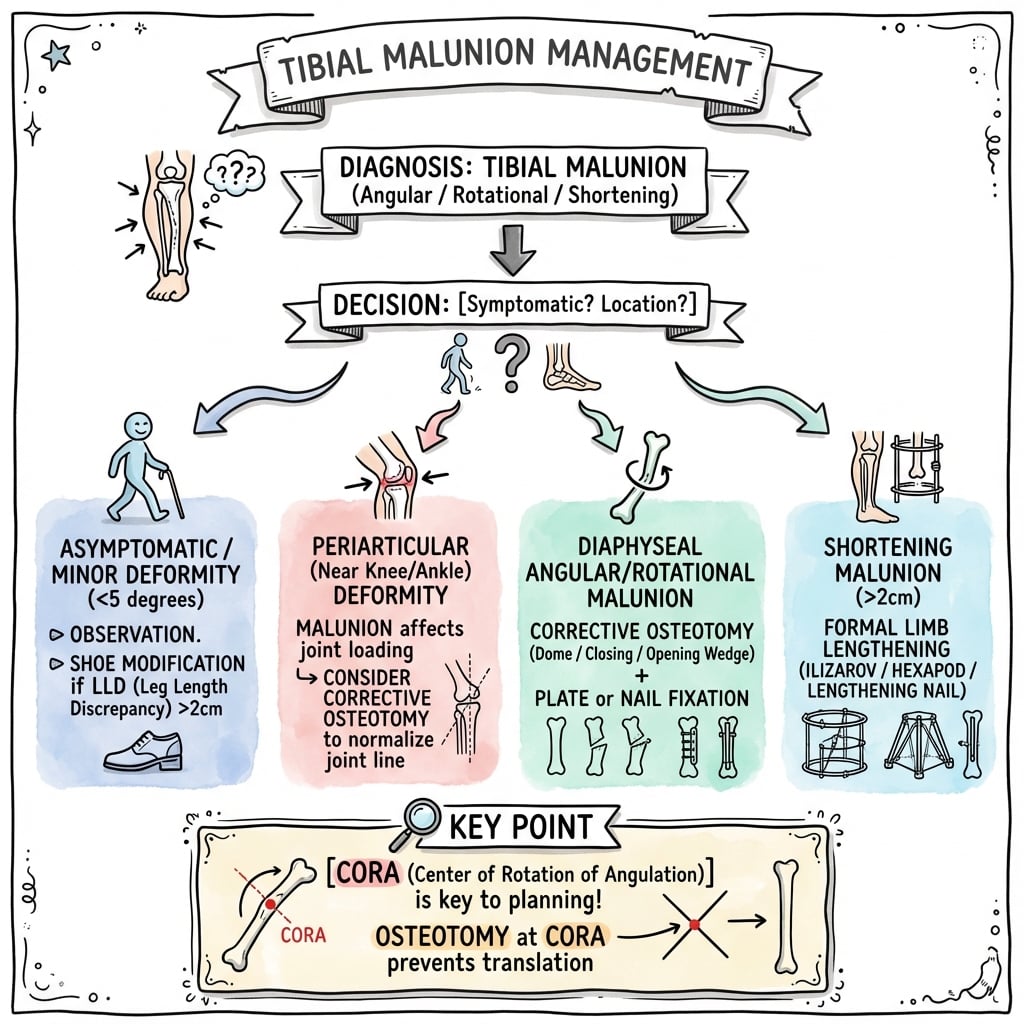
Tibial Malunion Management
Assess all deformity components (angulation, rotation, length, translation). Obtain full-length standing radiographs and CT scan. Calculate CORA. Measure mechanical axis deviation (MAD).
If angular deformity over 10-15°, rotational over 15-20°, shortening over 2cm, symptomatic, or predisposing to arthritis, proceed with correction. If asymptomatic and minimal deformity, consider observation.
Calculate CORA (intersection of proximal and distal axes). Plan osteotomy type (closing wedge, opening wedge, dome). Plan fixation (plate, nail, external fixator). Consider bone graft if opening wedge over 1cm.
Perform osteotomy at CORA (or planned location). Correct all deformity components. Verify correction intraoperatively (fluoroscopy, clinical assessment). Fix with rigid construct. Success rate 85-90%.
Surgical Technique
Closing Wedge Osteotomy
Indications:
- Angular deformity correction
- Shortening acceptable or desired
- Good bone quality
Technique:
- Exposure: Direct approach to malunion site
- Mark CORA: Identify CORA with K-wires under fluoroscopy
- Osteotomy: Make two cuts converging at CORA
- Wedge calculation: 1° correction = 1.75mm wedge base per 10cm length
- Remove wedge: Excise calculated wedge
- Close gap: Compress osteotomy site
- Fixation: Compression plate with at least 6 cortices each side
Advantages:
- Inherently stable (bone-bone contact)
- Faster healing
- Easier to hold reduction
Disadvantages:
- Shortens limb (~2mm per degree per 10cm)
- May not be suitable if lengthening needed
Closing wedge is preferred when shortening is acceptable.
CORA (Center of Rotation of Angulation) is critical for planning - Osteotomy AT the CORA corrects angulation without translation. Osteotomy AWAY from CORA creates translation deformity. Always calculate CORA preoperatively using full-length standing radiographs.
The Fibula in Tibial Malunion Correction
The leg is a two-bone segment, and any plan to realign the tibia must account for the fibula. An intact - or separately malunited - fibula behaves as a lateral strut that tethers the tibia and blocks correction. This is why the operative series in this topic's own evidence base routinely add a fibular procedure: Sanders performed a fibular osteotomy "as needed" during oblique tibial correction, and Hintermann corrected "malunion of the fibula" alongside the distal tibia in every case of his supramalleolar series.
When the fibula tethers correction
- Angular correction (varus/valgus, especially at the middle and distal thirds) - the fibula resists closing or opening the tibial wedge to the planned angle.
- Lengthening - a united fibula prevents distraction of the tibial segments.
- Derotation - a solidly healed fibula resists rotating the distal tibial fragment.
- Distal-third / ankle malunion - a short, externally rotated malunited fibula holds the talus in a malaligned position, so it must be osteotomised and realigned first to let the talus re-centre under the tibia (the same principle as correcting a malunited ankle fracture).
Technique and cautions
- Perform the fibular osteotomy through a separate lateral incision, ideally at a different level from the tibial cut (staggered), to reduce the risk of tibiofibular cross-union / synostosis.
- An oblique fibular cut allows some sliding for length and easier fixation.
- Protect the nerves: a proximal fibular osteotomy risks the common peroneal nerve; a distal osteotomy risks the superficial peroneal nerve.
- Do not osteotomise a fibula that is not tethering - for a short-segment sagittal (procurvatum/recurvatum) correction with a compliant fibula, an unnecessary cut simply adds a second bone to heal.
Q: A tibial osteotomy for malunion will not reach the planned alignment intraoperatively - what is the most likely mechanical cause? A: A tethering intact or malunited fibula. Because the leg is a two-bone segment, the fibula acts as a lateral strut resisting tibial realignment, length and derotation. Plan a concomitant, staggered-level fibular osteotomy for angular, rotational and lengthening corrections - especially distal-third and ankle-level deformity - while protecting the peroneal nerves.
CORAMalunion Correction Principles
Hook:CORA: Center of Rotation of Angulation - osteotomy at CORA corrects without translation!
ARSIndications for Correction
Hook:ARS: Angular over 10-15°, Rotational over 15-20°, Shortening over 2cm!
The Oblique (Single-Cut) Osteotomy for Combined Deformity
The surgical-technique menu above (closing wedge, opening wedge, dome, derotational) omits the oblique single-cut osteotomy, even though this topic's own evidence base (Sanders) and its management algorithm ("dome/oblique for multiplanar deformity") both invoke it. It deserves separate description because it uniquely corrects multiplanar angulation and length through one cut.
Concept
A single oblique (angled) cut is planned so that rotating the distal fragment about the plane of the osteotomy simultaneously corrects coronal and sagittal angulation; sliding the fragments along the oblique surface then adds or removes length. The obliquity and axis of the cut are chosen from full-length templating, because the achieved correction is exquisitely sensitive to the plane selected. The broad oblique bone contact provides a large healing surface and accepts a lag screw plus a neutralisation plate.
Evidence and outcomes
- Sanders and colleagues (PMID 7844130) treated 15 multiplanar tibial malunions with a single oblique osteotomy, lag screw and neutralisation plate.
- Mean preoperative deformity was 14 degrees coronal and 13 degrees sagittal, corrected to within about 1 degree in the coronal plane, with a mean of 1.3 cm of lengthening and union at 4.5 months.
- 10 of 12 followed patients had an excellent result.
When to choose it
- Combined coronal and sagittal angulation with a length component, in good-quality diaphyseal bone - an alternative to a dome osteotomy or to stacking two single-plane wedges.
- Monitor for lengthening (Sanders used somatosensory evoked potentials during axial lengthening), and usually add a fibular osteotomy.
Q: A diaphyseal tibial malunion has combined varus, procurvatum and 1.5 cm of shortening. What single osteotomy can address all three components? A: A planned oblique (single-cut) osteotomy. Rotating the distal fragment about one carefully chosen oblique plane corrects multiplanar angulation, and sliding along the cut adds length. Sanders fixed these with a lag screw and neutralisation plate, reporting correction to within about 1 degree coronally, roughly 1.3 cm of lengthening, union near 4.5 months and 10 of 12 excellent results.
CODOsteotomy Types
Hook:COD: Closing wedge (stable, shortens), Opening wedge (lengthens, graft), Dome (multiplanar)!
Complications
- Incidence
- 10-15%
- Risk Factors
- Opening wedge, smoking, poor fixation
- Prevention/Management
- Bone graft, rigid fixation, smoking cessation
- Incidence
- 5-10%
- Risk Factors
- Inadequate fixation, premature weight bearing
- Prevention/Management
- Rigid fixation, protected weight bearing
- Incidence
- 10-15%
- Risk Factors
- Inadequate planning, poor intraoperative assessment
- Prevention/Management
- Meticulous planning, intraoperative verification
- Incidence
- 5-10%
- Risk Factors
- Previous surgery, compromised soft tissue
- Prevention/Management
- Careful technique, prophylactic antibiotics
- Incidence
- 5-10%
- Risk Factors
- Proximal tibia (peroneal nerve)
- Prevention/Management
- Identify and protect nerves
Nonunion
10-15% incidence (opening wedge):
- Cause: Gap must heal, inadequate graft, poor fixation, smoking
- Prevention: Bone graft if gap over 1cm, rigid fixation, smoking cessation
- Management: Revision fixation with bone graft
Loss of Correction
5-10% incidence:
- Cause: Inadequate fixation, premature weight bearing, poor bone quality
- Prevention: Rigid fixation (minimum 6 cortices each side), protected weight bearing
- Management: Revision fixation if significant
Overcorrection/Undercorrection
10-15% incidence:
- Cause: Inadequate preoperative planning, poor intraoperative assessment
- Prevention: Meticulous planning, intraoperative verification (fluoroscopy, clinical)
- Management: Revision osteotomy if symptomatic
Postoperative Care
Immediate Postoperative
- Immobilization: Splint initially (2 weeks)
- Weight bearing: Depends on fixation
- Closing wedge with rigid plate: May allow early weight bearing
- Opening wedge: Protected weight bearing 6-12 weeks
- Dome: Protected weight bearing 6-12 weeks
- ROM: Early knee and ankle ROM (immediate)
- PT: ROM exercises, strengthening
Rehabilitation Protocol
Weeks 0-2:
- Splint or cast
- Non-weight bearing or touch-down weight bearing
- Knee and ankle ROM exercises
- Ice and elevation
Weeks 2-6:
- Transition to walking boot (if distal)
- Progressive weight bearing (if fixation stable)
- Continue ROM and strengthening
- Balance and proprioception
Weeks 6-12:
- Progressive to full weight bearing
- Full ROM
- Progressive activity
Weeks 12+:
- Full weight bearing
- Return to activity (when union confirmed)
- Continue monitoring with serial X-rays
Union and Hardware Removal
Union timeline: Typically 3-4 months postoperatively.
Hardware removal: Consider if prominent or symptomatic, usually after union confirmed (6-12 months).
Outcomes and Prognosis
Overall Outcomes
Corrective osteotomy outcomes:
- Success rate: 85-90% (good correction, union)
- Functional outcomes: 80-85% return to pre-injury level
- Complications: 15-20% (nonunion, loss of correction, overcorrection)
Union rates:
- Closing wedge: 90-95% (inherently stable)
- Opening wedge: 85-90% (requires graft, higher nonunion risk)
- Dome: 85-90% (technically demanding)
Functional Outcomes
Return to activity:
- Timeline: 6-12 months postoperatively
- Rate: 80-85% return to pre-injury level
- Factors: Deformity severity, treatment method, rehabilitation compliance
Pain relief:
- Immediate: 70-80% pain relief with correction
- Long-term: Maintained if correction maintained
- Factors: Correction quality, arthritis presence
Long-Term Prognosis
Arthritis prevention:
- With correction: 80-85% prevent or delay arthritis
- Without correction: 50-60% develop arthritis at 10 years
- Risk factors: Deformity severity, joint involvement
Correction maintenance:
- Closing wedge: 90-95% maintain correction
- Opening wedge: 85-90% maintain correction
- Loss of correction: 5-10% (usually minor)
Factors Affecting Outcomes
Positive factors:
- Good preoperative planning (CORA calculation)
- Rigid fixation
- Adequate bone graft (if opening wedge)
- Complete rehabilitation
Negative factors:
- Inadequate planning
- Poor fixation
- Inadequate bone graft
- Smoking
- Premature weight bearing
Prevention and Return to Sport
Prevention
Primary prevention:
- Proper initial fracture reduction
- Adequate fixation
- Close follow-up during healing
- Early intervention if malunion developing
Secondary prevention (after malunion):
- Corrective osteotomy if indicated
- Prevent progression to arthritis
- Maintain function
Return to Sport
Criteria:
- Full union confirmed
- Full ROM (equal to contralateral)
- Strength greater than 90% of contralateral
- No pain or instability
Timeline: Usually 6-12 months postoperatively, depending on union and rehabilitation.
Guidelines, Registries & Global Practice
Global Epidemiology
- Tibial shaft fractures are among the most common long-bone fractures, with population incidence commonly quoted around 16-22 per 100,000 per year; high-energy diaphyseal injuries predominate in young men and fragility-type injuries in older women.
- Symptomatic malunion is a minority outcome but a recognised one: long-term cohorts (van der Schoot, PMID 8836057) found roughly half of healed lower-leg fractures retained at least 5 degrees of malalignment, and 3D analysis after nailing (Boucher/Bhandari, PMID 12172277) found about 77% malaligned by convention - though most remain asymptomatic.
- Distal-third deformity is the least forgiving because malalignment is referred to the ankle (Puno, PMID 1941305).
Side-by-Side Guidance
- Emphasis
- Deformity analysis, CORA / osteotomy rules
- Practical position
- Plan from full-length standing films; osteotomy and correction axis through the CORA
- Emphasis
- Get initial fixation right to prevent malunion
- Practical position
- Open-fracture and shaft standards stress acceptable alignment at index surgery
- Emphasis
- Symptom- and function-led correction
- Practical position
- Reconstruct for symptomatic deformity / mechanical-axis malalignment, not radiographs alone
- Emphasis
- Joint-preserving realignment before salvage
- Practical position
- Supramalleolar / periarticular osteotomy preferred while cartilage is intact
Registry and Outcome Notes
- No arthroplasty-style registry tracks corrective osteotomy itself, but national hip-and-knee registries (NJR UK, AJRR US, AOANJRR Australia, SHAR Sweden) capture the downstream end-points - arthroplasty for post-traumatic arthritis - that uncorrected malalignment can drive.
- High tibial osteotomy registry and series data inform the malunion debate on hinge fractures and loss of correction (e.g. lateral hinge fracture incidence around 24% in opening-wedge HTO, PMID 31273455), reinforcing the value of protecting the far cortex/hinge.
High- vs Limited-Resource Practice
- Well-resourced settings: CT with 3D reconstruction, computer-assisted / patient-specific guides, and hexapod circular frames for gradual multiplanar correction are routine options.
- Limited-resource settings: Correction relies on careful clinical and plain-radiograph planning, acute single-cut osteotomy with plate or nail fixation, and judicious use of simpler external fixators; the deformity-analysis principles are unchanged even where advanced imaging is unavailable.
Q: What are the key points examiners look for in tibial malunion vivas? A: CORA concept (osteotomy at CORA corrects without translation), a symptom/mechanical-axis-led indication qualified by deformity level and joint status, and the osteotomy menu (closing vs opening wedge, oblique, dome, derotational, supramalleolar). Be ready to calculate the CORA and to say when realignment must be combined with fusion / arthroplasty.
Controversies and Areas of Uncertainty
The "safe" thresholds quoted in textbooks are pragmatic conventions, not hard biomechanical limits, and several long-running debates affect everyday decisions.
Classic cadaveric and clinical work argues angulation predisposes to arthritis, yet 3D outcome data (Boucher/Bhandari) found 77% of nailed tibiae malaligned by convention with no functional penalty at 5.5 years. The honest position: treat symptomatic mechanical-axis deviation, not an isolated degree measurement.
A given angle produces more joint malalignment the closer the apex is to a joint (Puno). A distal deformity is far less forgiving than the same angle mid-shaft, so the threshold to correct should fall as the deformity approaches the ankle.
No high-level randomised data favour one over the other for diaphyseal malunion. Closing wedge gives immediate bone contact and stability but shortens; opening wedge preserves length but adds a gap to heal. Acute correction vs gradual correction (hexapod / circular frame) is a parallel debate, with frames favoured for large, multiplanar or length deformities and where soft tissues are poor.
When malunion coexists with established adjacent arthritis, realignment alone underperforms (Kane and Raikin). Whether to stage osteotomy then later fusion / replacement, or to combine in one procedure, remains surgeon- and patient-specific.
Examiners reward candidates who say the indication for correction is symptomatic deformity or demonstrable mechanical-axis malalignment, qualified by deformity level (distal less tolerant) and joint status (correct the joint too if already arthritic) - rather than reciting a single degree cut-off as if it were absolute.
MCQ Practice Points
Q: What is CORA and why is it important? A: CORA (Center of Rotation of Angulation) = intersection of proximal and distal anatomic axes - Osteotomy AT the CORA corrects angulation without translation. Osteotomy AWAY from CORA creates translation deformity. Critical for preoperative planning.
Q: What are the indications for tibial malunion correction? A: Angular deformity over 10-15°, rotational over 15-20°, shortening over 2cm, symptomatic, or predisposing to arthritis - Mechanical axis deviation (MAD) over 10mm is significant. Normal mechanical axis passes through knee center.
Q: How do you calculate the wedge size for a closing wedge osteotomy? A: 1° correction = 1.75mm wedge base per 10cm bone length - Example: 15° varus correction at 10cm level = 26mm wedge base width. Closing wedge shortens limb (~2mm per degree per 10cm).
Q: When is opening wedge osteotomy preferred over closing wedge? A: When lengthening is desired or bone preservation is critical - Opening wedge lengthens limb and preserves bone stock. Requires bone graft if gap over 1cm. Higher nonunion risk (10-15%) than closing wedge.
Q: How do you assess rotational malunion? A: CT rotation protocol comparing to contralateral limb - Radiographs cannot reliably show rotation. Clinical assessment: For tibia, assess foot progression angle with knee flexed 90°. Intraoperatively, use K-wire markers in proximal and distal segments.
Q: What is normal mechanical axis and when is deviation significant? A: Normal mechanical axis passes from femoral head center through knee center to ankle center - Should pass through knee center (medial to tibial spine). Mechanical axis deviation (MAD) over 10mm is significant and predisposes to arthritis.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents 8 months after tibial shaft fracture treated with IM nail. He has medial knee pain with activity. Standing radiographs show 18 degrees varus deformity with mechanical axis deviation of 15mm medial to knee center. The malunion is in the middle third of the tibia.”
“A 30-year-old athlete presents 10 months after tibial shaft fracture. He has difficulty with cutting and pivoting activities. Clinical examination shows 25 degrees internal rotation compared to the contralateral side. CT rotation protocol confirms 25 degrees internal rotation malunion. The malunion is in the middle third.”
“A 48-year-old labourer presents 14 months after a distal-third tibial fracture treated non-operatively in a cast. He has activity-related anteromedial ankle pain. Standing films show a 12 degrees valgus, apex-medial deformity in the distal metaphysis with a mildly tilted talus; the ankle joint space is largely preserved. There is no shaft tenderness and inflammatory markers are normal.”
Key Concepts
- CORA = Center of Rotation of Angulation (intersection of proximal and distal axes)
- Osteotomy at CORA corrects angulation without translation
- Osteotomy away from CORA creates translation deformity
- Mechanical axis: Femoral head center → knee center → ankle center
Indications
- Angular deformity: Over 10-15° (MAD over 10mm)
- Rotational deformity: Over 15-20° (functional impairment)
- Shortening: Over 2cm (gait asymmetry)
- Symptomatic: Pain, functional impairment
- Predisposing to arthritis: Abnormal joint loading
Osteotomy Techniques
- Closing wedge: Stable, shortens (~2mm per degree per 10cm), 90-95% union
- Opening wedge: Lengthens, needs graft if gap over 1cm, 85-90% union
- Dome: Multiplanar, no length change, technically demanding
- Derotational: For rotational malunion, clinical verification critical
Preoperative Planning
- Full-length standing radiographs (mechanical axis, CORA calculation)
- CT scan with 3D reconstruction (multiplanar deformity)
- Rotation protocol (compare to contralateral)
- Calculate CORA, measure all components (angulation, rotation, length, translation)
Complications
- Nonunion: 10-15% (opening wedge, prevent with graft and rigid fixation)
- Loss of correction: 5-10% (prevent with rigid fixation)
- Overcorrection/undercorrection: 10-15% (prevent with meticulous planning)
- Infection: 5-10% (careful technique)
Evidence Base
Angular malunion drives adjacent-joint arthritis (15-year follow-up)
- 49% healed with at least 5° malalignment at long-term review
- Malaligned fractures had significantly more knee and ankle arthritis
- Supports anatomic reduction to minimise late degenerative change
Ankle (not knee) malalignment predicts poor outcome
- Ankle malalignment correlated strongly with poor outcome (p=0.001)
- Knee outcome did not correlate with knee malalignment (p=0.82)
- Distal-third deformity is less well tolerated than proximal
Oblique osteotomy for multiplanar tibial malunion
- Single oblique osteotomy corrects combined coronal and sagittal deformity
- Coronal correction to within 1° of normal; union at 4.5 months
- 10 of 12 excellent results with lag screw plus neutralisation plate
Supramalleolar osteotomy for distal-tibial / ankle malunion
- 87.5% good or excellent at 7-year follow-up
- Realignment restored a congruent ankle in the majority
- Joint-preserving alternative to fusion / replacement for distal malunion
Combined osteotomy plus TTC nail for malunion with hindfoot arthritis
- Single-stage osteotomy plus TTC nail for malunion with established arthritis
- VAS pain 8.3 to 2.8; AOFAS hindfoot 43 to 76
- Realignment alone is insufficient once the joint is destroyed
Conventional alignment thresholds are exceeded but not always symptomatic
- 77% met conventional malunion criteria after IM nailing
- Radiographic malalignment did not correlate with function at 5.5 years
- Plain films underestimate coronal deformity vs 3D / CT
CORA and the osteotomy rules of deformity correction
- CORA = intersection of proximal and distal axes, at the apex of deformity
- Osteotomy and ACA through CORA = pure angular correction, no translation
- Osteotomy away from CORA mandates translation to restore the axis