Tibial Nerve Anatomy
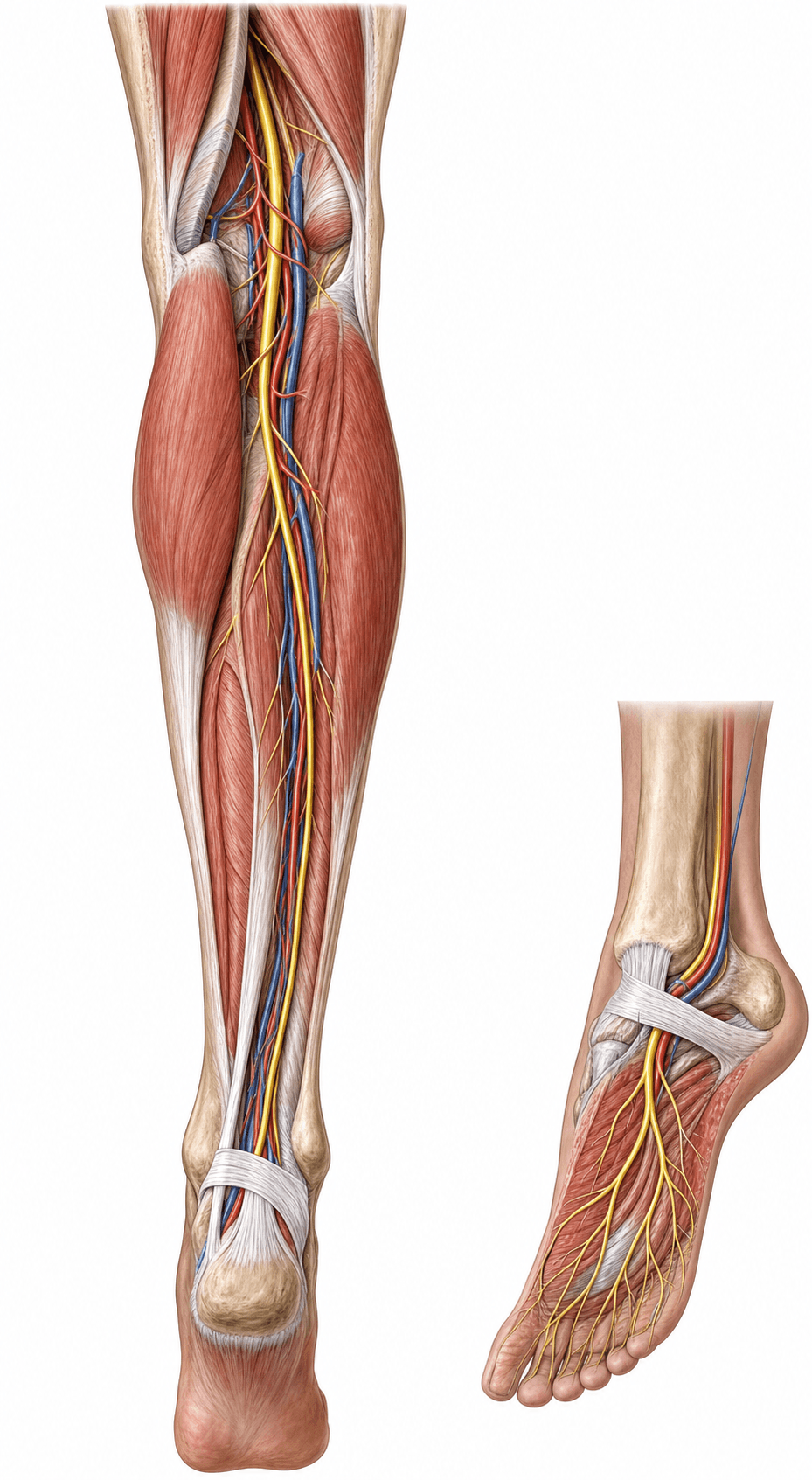
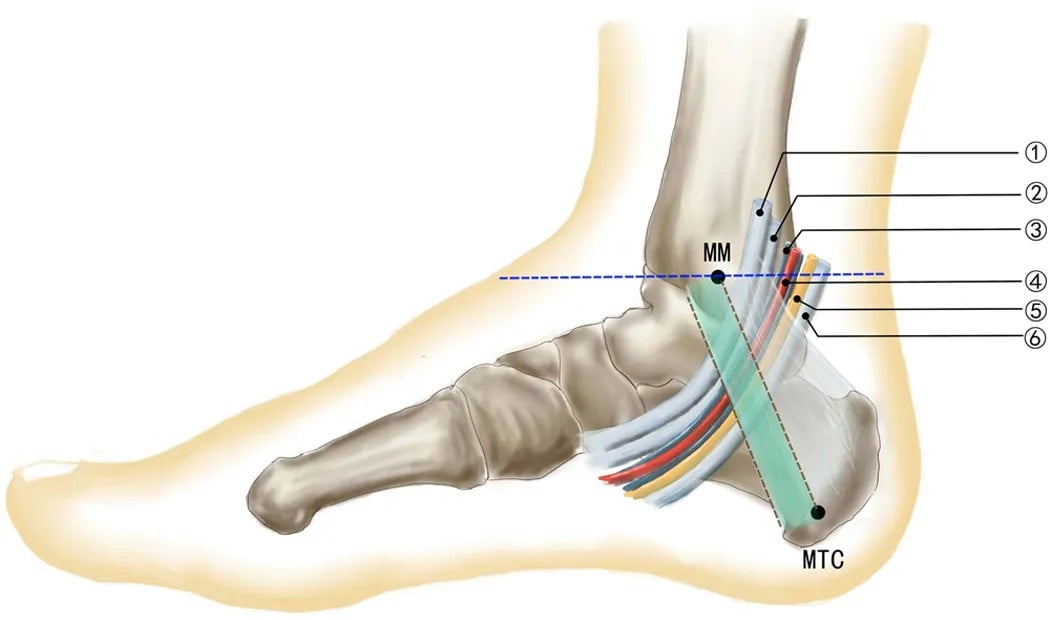
Deep to the flexor retinaculum behind the medial malleolus, anterior to posterior: Tibialis posterior, flexor Digitorum longus, posterior tibial Artery and Vein, tibial Nerve, flexor Hallucis longus. The nerve divides here into medial and lateral plantar nerves.
Compression of the tibial nerve (or its plantar branches) in the tunnel causes burning sole pain, paraesthesia and a positive Tinel sign behind the medial malleolus. Causes include space-occupying lesions (ganglion, varicosities), deformity (hindfoot valgus) and trauma.
Tom, Dick, And Very Nervous HarryTarsal Tunnel Contents (Ant → Post)
Hook:Tom, Dick, And Very Nervous Harry — Tibialis posterior, flexor Digitorum longus, Artery (+Vein), Nerve, flexor Hallucis longus, anterior to posterior through the tarsal tunnel.
Overview
The tibial nerve is the workhorse of the posterior leg and foot: it plantarflexes the ankle, flexes the toes, inverts the foot and gives the sole its sensation — so it is the nerve you assess in a knee dislocation, a posterior-leg or popliteal injury, and any patient with sole symptoms. Its exam value clusters at two sites: the popliteal fossa (where it is the most superficial of the bundle and at risk with the popliteal artery in knee dislocation) and the tarsal tunnel behind the medial malleolus (where it and its plantar branches are compressed or entrapped). Hold three ideas together — the course (sciatic → popliteal fossa → deep posterior compartment → tarsal tunnel → plantar nerves), the deficit (loss of plantarflexion/toe flexion and an insensate sole), and the entrapments (tarsal tunnel syndrome, Baxter's nerve, jogger's foot).
Origin & Course
Origin
- The tibial nerve is the larger terminal branch of the sciatic nerve, carrying fibres from the anterior (ventral) divisions of L4-S3.
- The sciatic nerve typically divides into the tibial and common peroneal nerves at the apex of the popliteal fossa (though a higher division is a common variant).
Innervation: Motor & Sensory Supply
The tibial nerve supplies both posterior leg compartments: superficial (gastrocnemius, soleus, plantaris) and deep (tibialis posterior, flexor digitorum longus, flexor hallucis longus, popliteus), plus all the intrinsic plantar muscles via the plantar nerves.
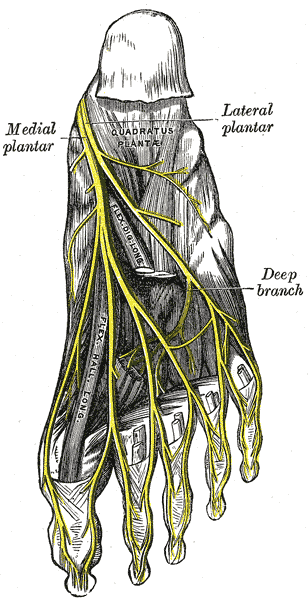
Medial 3.5 / Lateral 1.5 (the hand's median-ulnar pattern, in the foot)Plantar nerve territories
Hook:The sole mirrors the hand: medial plantar = median (medial 3.5 toes), lateral plantar = ulnar (lateral 1.5 toes).
- Plantarflexion (gastrocnemius-soleus - "tiptoe"), inversion (tibialis posterior) and toe flexion (FDL/FHL) all depend on the tibial nerve.
- Sensory: the sole of the foot (medial plantar - medial sole and medial 3.5 toes; lateral plantar - lateral sole and lateral 1.5 toes), the heel (medial calcaneal), and a contribution to the sural nerve (posterolateral leg/lateral foot).
Regional Anatomy: Nerve Block and Plantar Entrapments
Beyond tarsal tunnel syndrome, three practical points round out the foot-and-ankle examiner's expectations.
- Posterior tibial nerve block. The tibial nerve is blocked behind the medial malleolus, just posterior to the posterior tibial artery, as part of an ankle block for forefoot and sole surgery — it is the component that anaesthetises the sole. Knowing its position relative to the artery (nerve posterior to the pulse) is the practical landmark.
- Jogger's foot (medial plantar nerve entrapment). The medial plantar nerve can be entrapped at the knot of Henry (where FDL and FHL tendons cross) or under the abductor hallucis, classically in runners with a valgus/pronated foot — producing medial arch/sole burning and altered sensation of the medial sole and medial toes.
- Baxter's nerve revisited. The first branch of the lateral plantar nerve (Baxter's / inferior calcaneal nerve) is entrapped between abductor hallucis and quadratus plantae and is a frequently-missed cause of chronic plantar heel pain that mimics plantar fasciitis — suspect it when heel pain is refractory or associated with abductor digiti minimi wasting.
- Proximal entrapment at the soleal sling. The tarsal tunnel is the distal entrapment, but the tibial nerve can also be compressed proximally where it passes deep to the tendinous arch of soleus (the "soleal sling") as it enters the deep posterior compartment — proximal/high tibial neuropathy. This produces calf pain with plantar paraesthesia and a Tinel sign high in the popliteal/proximal-calf region rather than behind the medial malleolus, and is a recognised (often exertional) cause of posterior-leg and sole symptoms that a medial-ankle examination will miss — so localise the level of the Tinel sign and consider the soleal sling when tarsal-tunnel signs are absent.
A patient with refractory "plantar fasciitis" who fails standard treatment may have Baxter's nerve entrapment; a runner with a pronated foot and medial arch burning may have jogger's foot (medial plantar entrapment). Both are tibial-nerve-branch entrapments that plain plantar-fasciitis management will not fix — the anatomy is the diagnosis.
Clinical Correlations
Proximal (High) Tibial Nerve Injury
- Occurs with knee dislocation, proximal tibial trauma, or popliteal injury.
- Deficit: loss of plantarflexion, inversion and toe flexion (a calcaneovalgus foot), loss of intrinsic foot muscles, and crucially an insensate sole.
- The insensate plantar surface historically influenced limb-salvage-versus-amputation decisions, though this is now applied cautiously as outcomes data have evolved.
The tibial nerve's motor branches to the triceps surae (gastrocnemius/soleus) and tibialis posterior are the targets for managing the spastic equinovarus foot (stroke, traumatic brain injury, cerebral palsy) — a high-yield neuro-orthopaedic point separate from trauma and entrapment:
- A diagnostic tibial nerve / motor-branch block (local anaesthetic) is performed first to distinguish dynamic spasticity (which relaxes after the block) from a fixed contracture (which does not), predicting the response to definitive treatment.
- Botulinum toxin or phenol chemodenervation of the gastrocsoleus and tibialis posterior motor branches gives reversible tone reduction and is often the first definitive step.
- Selective (fascicular) tibial neurotomy — partial section of the motor branches to the spastic muscles — gives a durable reduction in equinovarus tone and is an alternative/adjunct to the orthopaedic options (tendo-Achilles lengthening, split tibialis anterior/posterior transfer).
The same anatomy that explains an insensate sole after a high injury explains where the surgeon or injector targets tone in the spastic foot.
Guidelines, Registries & Global Practice
Global Practice Picture
Tibial nerve anatomy underpins management of tarsal tunnel syndrome, plantar heel pain (Baxter's nerve), posterior leg compartment and popliteal injuries, and the assessment of the insensate foot. The internationally consistent principles are: know the tarsal tunnel contents and plantar division, diagnose tarsal tunnel syndrome clinically with electrodiagnostic/imaging support, and treat the underlying cause.
Side-by-Side Synthesis
- Detail
- Larger terminal branch of sciatic (L4-S3)
- Detail
- Superficial + deep posterior compartments
- Detail
- Tarsal tunnel (behind medial malleolus)
- Detail
- Medial + lateral plantar (+ medial calcaneal)
- Detail
- Sole of foot, heel, (sural contribution)
- Detail
- Tarsal tunnel syndrome; high injury → insensate sole
Evidence Base
Both references (checked against PubMed) are descriptive/anatomical rather than outcome studies. Develi documents a tarsal-tunnel branching variant — useful only as a reminder that the plantar division is variable (high division/trifurcation), which matters at tarsal-tunnel release and in Baxter's-nerve pathology. Bowley & Doughty is a review situating tarsal tunnel syndrome among lower-limb entrapment neuropathies, reinforcing that the diagnosis is clinical with electrodiagnostic/imaging support. For an anatomy viva the reproducible course, the tarsal-tunnel contents and the named entrapments matter more than either single paper.
Trifurcation of the tibial nerve within the tarsal tunnel
- The tibial nerve is the larger terminal branch of the sciatic nerve and terminates in the tarsal tunnel as the medial and lateral plantar nerves
- Reports a trifurcation variant of the tibial nerve within the tarsal tunnel
- The variant branch curved laterally and ran deep to quadratus plantae
- The posterior tibial artery showed a corresponding three-branch termination
Entrapment Neuropathies of the Lower Extremity
- Reviews cause, signs, diagnosis and treatment of lower-limb entrapment neuropathies including the posterior tibial nerve (tarsal tunnel syndrome)
- Accurate identification and management prevents pain, sensory loss and weakness affecting mobility
- Diagnosis relies on clinical examination supported by electrodiagnosis and imaging (ultrasound/MRI)
- Considers the tibial nerve alongside common peroneal, femoral and lateral femoral cutaneous neuropathies