Evaluation and Management of Unhealed Tibial Fractures | Exchange Nailing | Bone Grafting | Ilizarov
- Definition: Fracture that has not healed by 9 months, or shows no progression for 3 months.
- Workup: Verify INFECTION status (ESR, CRP, aspiration) and METABOLIC status (Vit D, Ca, PTH).
- Hypertrophic: Needs STABILITY (Exchange nailing usually successful).
- Atrophic: Needs BIOLOGY (Bone graft, RIA) and STABILITY.
- Infected: Needs DEBRIDEMENT first (Masquelet technique or Bone Transport).
- “The 'Diamond Concept' covers: Mechanical Stability, Osteogenesis, Osteoconduction, Osteoinduction.
- “Exchange nailing allows reaming (autograft) and larger nail (stability).
- “Fibulectomy may be needed to allow compression of the tibial nonunion site.
Any nonunion remains infected until proven otherwise. Even with normal skin. Check CRP/ESR. Consider tagged WBC scan or biopsy.
An intact or healed fibula can strut the tibia, preventing compression ("hold-open" effect). A small section of fibula may need excision (fibulectomy) to allow dynamization.
Don't forget the medical causes! Vitamin D deficiency, thyroid/parathyroid issues, diabetes, smoking (nicotine).
Mandatory for elective nonunion surgery. Nicotine is a potent vasoconstrictor and inhibitor of healing.
- Callus
- Abundant (Elephant Foot)
- Vascularity
- Excellent
- Treatment Principles
- **Stability** (Stiffen fixation)
- Callus
- None (Pencil Tip)
- Vascularity
- Poor
- Treatment Principles
- **Biology** (Graft) + Stability
- Callus
- Variable
- Vascularity
- Poor (Biofilm)
- Treatment Principles
- **Debridement** first to Reconstruction
NICE MDNonunion Risk Factors
Hook:NICE MDs prevent nonunions.
VS GODiamond Concept
Hook:VS GO (Giannoudis)
Overview and Pathophysiology
- FDA: Fracture not healed at 9 months.
- Clinical: Fracture showing no radiographic progression over 3 consecutive months.
- Tibial Shaft: The most common location for long bone nonunion due to poor blood supply (anteromedial surface subcutaneous) and high energy trauma.
- Diamond Concept: Considers the biological and mechanical environment.
- Biology: Cells (osteoblasts), Scaffold (matrix), Signals (BMPs), Vascularity.
- Mechanics: Strain environment. Micro-motion promotes callus; too much motion prevents it; absolute rigid stability promotes primary healing (no callus).
Anatomy and Pathophysiology
Vascular Anatomy (Critical)
The tibia is subcutaneous anteromedially, making its blood supply vulnerable:
Nutrient Artery:
- Enters via posterior cortex at the proximal third
- Supplied by Posterior Tibial Artery
- Often disrupted in the initial fracture
- Provides 30-40% of blood supply
Periosteal Supply:
- The sole supply after nutrient artery disruption
- Depends on the surrounding soft tissue envelope
- Anterior tibial artery/muscles (lateral)
- Posterior tibial artery/muscles (posterior)
- Provides 60-70% of blood supply
Watershed Zone:
- The distal third of the tibia has the poorest blood supply
- Highest nonunion rate (distal third)
- Limited collateral circulation
Biomechanics
Strain environment:
- Primary healing: Strain less than 2% (absolute stability, no callus)
- Secondary healing: Strain 2-10% (micro-motion, callus formation)
- Nonunion: Strain greater than 10% (excessive motion prevents healing)
Fibula role:
- Acts as a strut
- If healed, prevents compression of the tibia ("holding it open")
- May require fibulectomy to allow compression
Pathophysiology
Hypertrophic nonunion:
- Biology: Good (abundant callus formation)
- Stability: Poor (excessive motion)
- Mechanism: Strain greater than 10% prevents bridging
- Treatment: Increase stability (exchange nailing)
Atrophic nonunion:
- Biology: Poor (no callus, sclerotic bone)
- Stability: Variable
- Mechanism: Biological failure (poor vascularity, dead bone)
- Treatment: Improve biology (bone graft) + stability
Infected nonunion:
- Biology: Poor (biofilm prevents healing)
- Stability: Variable
- Mechanism: Infection prevents biological healing
- Treatment: Eradicate infection first (debridement, antibiotics)
Classification Systems
Based on Vascularity of the bone ends (Strontium scan originally, now radiographic appearance).
- Hypertrophic: High vascularity. "Elephant Foot". Problem = Instability.
- Atrophic: Low vascularity. "Pencil Point". Problem = Biology.
- Oligotrophic: Intermediate. "Horse Hoof".
Clinical Assessment
History
Pain:
- Pain upon weight bearing is the hallmark
- Pain at rest suggests infection
- Persistent pain despite adequate time for healing
Constitutional symptoms:
- Fevers/chills (infection)
- Night sweats (infection)
- Weight loss (infection, malignancy)
Risk factors:
- Smoking (most important modifiable factor - slower union, more secondary surgery)
- Diabetes (poor healing)
- NSAID use (inhibits bone healing)
- Steroids (inhibits bone healing)
- Previous open fracture (infection risk)
Physical Examination
Inspection:
- Condition of skin/flaps (previous surgery, open fracture)
- Sinus tracts (infection - pathognomonic)
- Deformity (malalignment, shortening)
- Swelling (infection, chronic inflammation)
Palpation:
- Tenderness at fracture site
- Motion at fracture site (gross instability)
- Warmth (infection)
- Crepitus (motion at nonunion)
Neurovascular:
- Distal pulses (posterior tibial, dorsalis pedis)
- Sensation (saphenous, sural, superficial peroneal)
- Motor function (dorsiflexion, plantarflexion)
Pain with weight bearing is the hallmark of nonunion - persistent pain despite adequate time for healing. Pain at rest suggests infection. Always assess for sinus tracts (pathognomonic for infection) and motion at fracture site (gross instability).
Associated Conditions
- Infection: Previous open fracture, sinus tracts
- Metabolic disease: Vitamin D deficiency, hyperparathyroidism
- Smoking: Most important modifiable risk factor
- Diabetes: Poor healing, infection risk
Investigations

- Infection: CBC, ESR, CRP. (If elevated, Aspiration/Biopsy).
- Metabolic: Calcium, Phosphate, ALP, Vitamin D (25-OH), PTH, TSH, HbA1c, Albumin.
- X-rays: AP/Lat/Oblique. Assess callus, implant failure, alignment.
- CT Scan: Gold standard for assessing bony bridging (often obscured by metal on X-ray). Look for less than 50% bridging on cuts.
- Nuclear Medicine:
- Bone Scan: High sensitivity, low specificity.
- WBC Scan (Indium/Sulfur colloid): Useful to differentiate infection from remodelling.
HOTInfection Workup
Hook:Is the nonunion HOT (Infected)?
Scoring Union Objectively: RUST and mRUST
The topic repeatedly asks you to "assess bony bridging", judge whether there has been "no radiographic progression over 3 months", and reach for CT when plain films are equivocal — yet the "is it united?" judgment on plain films is notoriously subjective and disagrees between observers. That matters here, because both the diagnosis of nonunion and the decision to reoperate hinge on that read. The Radiographic Union Score for Tibia (RUST) turns it into a reproducible number.
How RUST is scored
- Use orthogonal radiographs (AP and lateral); each view shows two cortices, so four cortices are scored in total.
- Each cortex scores: 1 = fracture line visible, no callus; 2 = callus present but fracture line still visible; 3 = bridging callus with the fracture line no longer visible.
- Sum the four cortices: RUST ranges from 4 (no healing at any cortex) to 12 (complete union at all four).
- mRUST (modified RUST) scores each cortex out of 4 — adding a top tier for a bridged cortex that has remodelled with no visible line — giving a range of 4 to 16 and finer discrimination, particularly around metaphyseal or plated fractures where callus is subtle.
Why it matters in nonunion
RUST is not just a fresh-fracture tool. In operatively treated tibial nonunions, a low preoperative RUST predicts failure of nonunion surgery and both pre- and post-operative RUST correlate with time to union — so scoring the cortices at presentation risk-stratifies the nonunion itself and calibrates how aggressive (biology plus stability, not stability alone) the reconstruction must be. Track RUST on serial films: a score that plateaus and fails to climb over 3 months supports the nonunion diagnosis and the case for intervention, while CT remains the arbiter when metal obscures cortices or the plain-film score is borderline.
RUST Predicts Success of Tibial Nonunion Surgery
- RUST applies to the nonunion itself, not only to fresh fractures
- A preoperative RUST below 7 flags a high risk of persistent nonunion
- Serial RUST helps time and judge the success of nonunion surgery
Q: How do you objectively quantify tibial union on radiographs, and why bother? A: RUST — score each of the four cortices on AP and lateral films (1 = fracture line, no callus; 2 = callus with a visible line; 3 = bridging callus, no line), summing to 4-12. mRUST scores each cortex out of 4 (range 4-16). It converts a subjective "united/not united" read into a reproducible number; a preoperative RUST below 7 predicts a high risk of persistent nonunion (Christiano/Egol 2018).
Differential Diagnosis
The clinical picture (persistent pain, failure to heal) overlaps with several entities. The single most important fork is infected vs aseptic, because it changes the whole reconstructive plan.
- Distinguishing Features
- Mechanical pain on loading, normal inflammatory markers, no sinus
- Key Discriminator
- Normal ESR/CRP, negative cultures
- Distinguishing Features
- Rest/night pain, sinus, warmth, raised ESR/CRP
- Key Discriminator
- Positive deep cultures / sinus tract
- Distinguishing Features
- Healing progressing but slow; callus advancing on serial films
- Key Discriminator
- Progression over 3 months (vs none in nonunion)
- Distinguishing Features
- Deformity/limb-length issue, pain may be adjacent joint
- Key Discriminator
- Bridging callus present on CT
- Distinguishing Features
- Implant breakage or backout, mechanical pain
- Key Discriminator
- Radiographic implant failure
- Distinguishing Features
- No clear preceding adequate fracture healing window; lytic lesion
- Key Discriminator
- MRI/biopsy if neoplasm suspected
Management Algorithm
Management Pathway
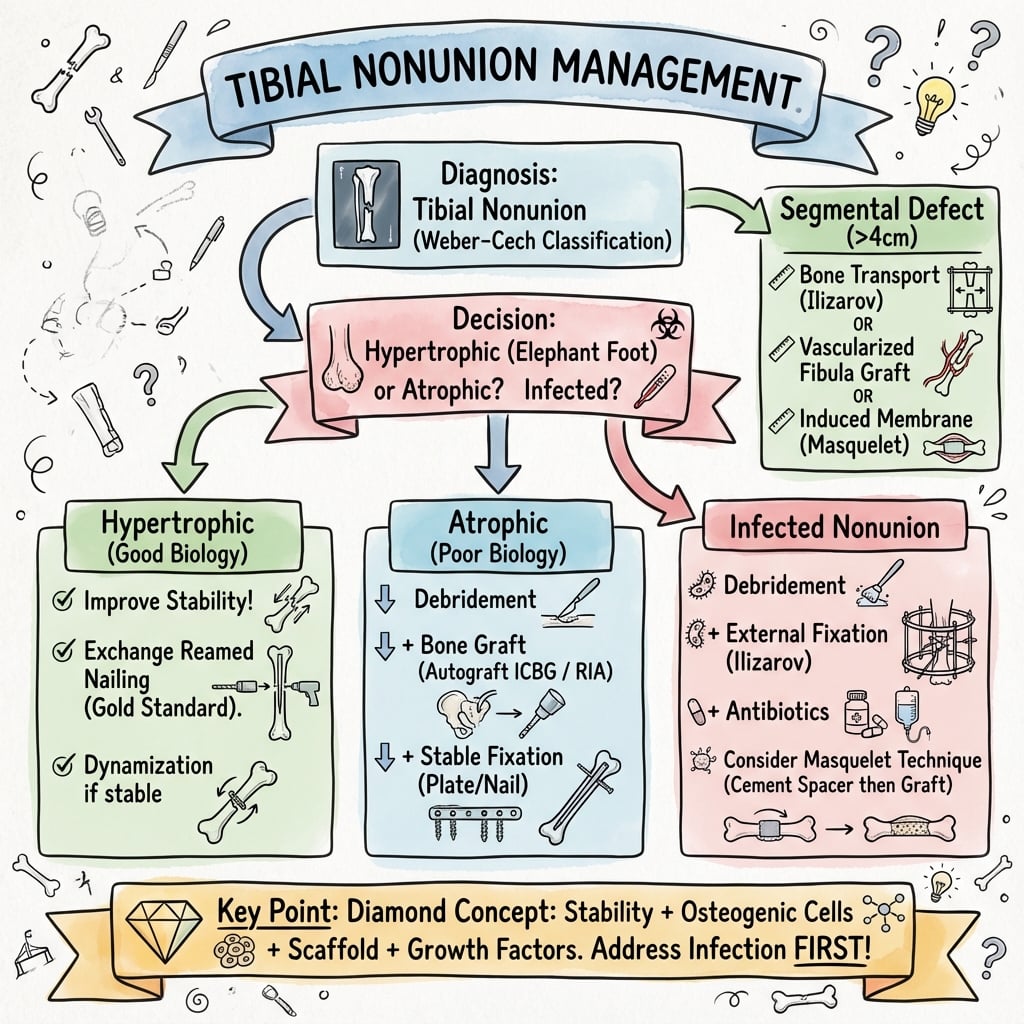
Tibial Nonunion Management
Classify nonunion (Weber & Cech: hypertrophic, atrophic, oligotrophic). Rule out infection (ESR, CRP, aspiration). Assess metabolic status (vitamin D, calcium, PTH). Obtain CT scan to assess bony bridging.
Smoking cessation mandatory (smokers have slower union and more secondary surgery - Adams 2001). Optimize metabolic status (vitamin D supplementation if deficient). Control diabetes. Discontinue NSAIDs if possible.
If hypertrophic (good biology, poor stability), exchange nailing with larger diameter nail. Success rate greater than 90%. Consider fibulectomy if fibula holding fracture apart.
If atrophic (poor biology), debride to bleeding bone, bone grafting (iliac crest or RIA), stable fixation (exchange nailing or compression plating). Success rate 85-90%.
If infected, staged approach: Stage 1 (debridement, hardware removal, antibiotic spacer), Stage 2 (6-8 weeks later, bone grafting or bone transport). Success rate 80-90%.
Surgical Technique
Exchange Nailing Technique
Indications:
- Hypertrophic nonunion (good biology, poor stability)
- Aseptic nonunion
- Previous IM nailing
Technique:
- Removal: Extract old nail. Send tip for sonication/culture (rule out infection).
- Reaming: Aggressive reaming of the canal. Often 1-2mm larger than previous. This produces "reamings" (autograft).
- Insertion: Insert a nail that is 1-2mm larger than the largest reamer.
- Locking: Static locking (or dynamic if axial stability is assured).
- Fibulectomy: Consider if fibula is holding the fracture apart.
Critical: Check distal pulses after reaming (vascular injury risk).
Success rate: Greater than 90% for hypertrophic nonunions.
Fibular Osteotomy: Releasing the 'Hold-Open' Strut
The intact fibula recurs throughout this topic — in the one-pager pearls, the "Intact Fibula" warning, the biomechanics, exchange nailing, the vivas and the cheat sheet — yet the technique and logic of dividing it are never developed. This is a uniquely tibial (two-bone-segment) problem worth owning here.
The mechanical problem
In the leg the tibia and fibula share length. When the fibula has healed (or was never broken) it behaves as a rigid lateral strut. As the tibia tries to compress across its nonunion — under weight-bearing, dynamization, or a compression device — the fibula "holds it open", distracting the tibial bone ends and defeating the very axial compression and callus-generating micromotion the treatment relies on. A persistent tibial gap alongside a united fibula on radiographs is the classic clue.
When to release it
- A hypertrophic (or oligotrophic) tibial nonunion with an intact/healed fibula where compression is the goal.
- Before dynamizing a nailed tibia (removing locking screws will not compress a fracture the fibula is strutting).
- When planning acute shortening of a segmental defect, where the fibula would otherwise resist limb-length adjustment.
Technique and pitfalls
- Perform a segmental fibular osteotomy/ostectomy — remove a short segment (about 1 cm, enough that the fibula cannot simply re-strut by bridging) through a small direct-lateral incision.
- Site the resection at a level offset from the tibial nonunion so the two do not consolidate into a single mass and so the exposure is safe.
- Stay away from the common peroneal nerve at the fibular neck proximally, and preserve the distal syndesmosis and lateral malleolus — a resection too distal destabilises the ankle mortise.
- It is an adjunct, not a stand-alone: fibular release enables the mechanical solution (compression plating/nailing, dynamization, or frame compression) but does not substitute for biology in an atrophic nonunion, and it is unnecessary when the fibula is itself un-united or already absent.
Q: Why and how do you divide the fibula in tibial nonunion surgery? A: A healed or intact fibula acts as a lateral strut that distracts the tibial nonunion and blocks compression and dynamization. Excise a short segment (about 1 cm) through a lateral incision, offset from the tibial nonunion, keeping clear of the common peroneal nerve proximally and preserving the distal syndesmosis. This lets the tibia compress under load, dynamization, or a compression frame — an adjunct to fixation, never a substitute for biology in atrophic nonunion.
Complications
- Incidence
- 10-20%
- Risk Factors
- Previous open fracture, infected nonunion
- Prevention/Management
- Thorough debridement, antibiotics, staged approach
- Incidence
- 5-10%
- Risk Factors
- Through graft site, screw holes
- Prevention/Management
- Protected weight bearing, gradual progression
- Incidence
- 10-20%
- Risk Factors
- Iliac crest harvest, RIA
- Prevention/Management
- Careful technique, consider RIA for large volumes
- Incidence
- Less than 5%
- Risk Factors
- Bleeding, tight compartments
- Prevention/Management
- Monitor, fasciotomy if needed
- Incidence
- 10-15%
- Risk Factors
- Smoking, infection, poor biology
- Prevention/Management
- Address all Diamond Concept components
Infection Recurrence
10-20% incidence:
- Cause: Especially in previously open fractures, biofilm presence
- Prevention: Thorough debridement, antibiotics, staged approach
- Management: Radical debridement, hardware removal, antibiotics, reconstruction
Re-fracture
5-10% incidence:
- Cause: Through graft site or screw holes, premature weight bearing
- Prevention: Protected weight bearing, gradual progression
- Management: Revision fixation if needed
Donor Site Morbidity
10-20% incidence:
- Cause: Iliac crest harvest (cluneal nerve injury), RIA (femur fracture)
- Prevention: Careful technique, consider RIA for large volumes
- Management: Pain management, nerve blocks if needed
Compartment Syndrome
Less than 5% incidence:
- Cause: Bleeding into tight compartments after surgery
- Prevention: Monitor, careful hemostasis
- Management: Fasciotomy if needed (four-compartment)
Postoperative Care
Immediate Postoperative
- Immobilization: None (early mobilization)
- Weight bearing: Partial weight bearing initially (depends on fixation stability)
- ROM: Early knee and ankle ROM (immediate)
- PT: Ambulation training, strengthening
Rehabilitation Protocol
Weeks 0-2:
- Partial weight bearing (20-50% body weight)
- Knee and ankle ROM exercises
- Quadriceps and calf strengthening
- Ice and elevation
Weeks 2-6:
- Progressive weight bearing (50-75% body weight)
- Continue ROM and strengthening
- Balance and proprioception
Weeks 6-12:
- Progressive to full weight bearing
- Full ROM
- Progressive activity
Weeks 12+:
- Full weight bearing
- Return to activity (when union confirmed)
- Continue monitoring with serial X-rays
Dynamization
If healing slow at 3-4 months:
- Remove static locking screws (proximal or distal)
- Allow localized compression at nonunion site
- Monitor with serial X-rays
Adjunctive Treatments
Low-intensity pulsed ultrasound (LIPUS):
- FDA approval for fresh fracture nonunions
- Evidence debated (TRUST trial showed no benefit)
- May be considered in selected cases
Outcomes and Prognosis
Overall Outcomes
Exchange nailing:
- Success rate: Greater than 90% for hypertrophic nonunions
- Time to union: 6-9 months after revision surgery
- Complications: 10-15% (infection recurrence, re-fracture)
Compression plating:
- Success rate: 85-90%
- Time to union: 6-9 months after revision surgery
- Complications: 10-15% (infection, hardware failure)
Ilizarov bone transport:
- Success rate: Greater than 90% for infected nonunions
- Time to union: 9-12 months (longer for large defects)
- Complications: 20-30% (pin site infection, joint stiffness)
Functional Outcomes
Return to activity:
- Timeline: 6-12 months postoperatively
- Rate: 80-85% return to pre-injury level
- Factors: Nonunion type, treatment method, smoking status, rehabilitation compliance
Functional testing:
- Strength: 90%+ of contralateral
- ROM: Full (if no complications)
- No pain or instability
Long-Term Prognosis
Union rates:
- Hypertrophic: Greater than 90% with exchange nailing
- Atrophic: 85-90% with bone graft + fixation
- Infected: 80-90% with staged reconstruction
Risk factors for failure:
- Smoking: Prolongs union and increases need for secondary surgery
- Infection: Higher failure rate
- Poor bone quality: Osteoporosis, metabolic disease
- Large defects: Greater than 5cm
Factors Affecting Outcomes
Positive factors:
- Hypertrophic nonunion (good biology)
- No infection
- Smoking cessation
- Good bone quality
- Complete rehabilitation
Negative factors:
- Atrophic nonunion (poor biology)
- Infection present
- Continued smoking
- Poor bone quality
- Large defects
Guidelines, Registries & Global Practice
Global Epidemiology
- Tibial shaft fracture is the most common long-bone fracture; nonunion complicates roughly 5-15% of shaft fractures and is higher (up to ~30-50%) after high-energy open (especially Gustilo IIIB/IIIC) injuries.
- The distal third is the highest-risk segment due to a precarious blood supply and thin soft-tissue envelope.
- Modifiable drivers (smoking, diabetes, malnutrition, NSAIDs) and injury factors (open wound, segmental loss, infection) dominate risk across all populations.
Guideline & Registry Landscape (Side by Side)
- Region
- USA
- Key Position on Nonunion
- Optimise mechanics + biology; reserve BMP for selected high-risk cases; routine adjuncts (LIPUS) not supported
- Region
- UK
- Key Position on Nonunion
- Early ortho-plastic combined care, definitive soft-tissue cover within 72h to reduce deep infection and nonunion
- Region
- Global
- Key Position on Nonunion
- Diamond Concept framework; absolute vs relative stability matched to nonunion type and strain
- Region
- Europe
- Key Position on Nonunion
- Non-union work-up must exclude low-grade infection; staged reconstruction for infected/segmental defects
- Registry evidence: trauma and limb-reconstruction registries (e.g. UK BOA open-fracture audits, national fracture databases) consistently link delayed soft-tissue cover, higher Gustilo grade and smoking to nonunion and deep infection.
High- vs Limited-Resource Practice Variation
- Ortho-plastic teams, free-flap cover, RIA grafting
- CT for union assessment, advanced imaging for infection
- Access to BMP, induced-membrane and circular-frame reconstruction
- Reliance on iliac-crest autograft and standard internal fixation
- Greater role for low-cost external fixation and bone transport
- Infection and delayed presentation more common; staged debridement central
Tibial nonunion is a common viva topic. Know that hypertrophic = needs stability (exchange nailing, high union rates), atrophic = needs biology + stability (debridement, bone graft + stable fixation), always rule out infection (ESR, CRP, aspiration/biopsy), smoking cessation is mandatory (slower union and more secondary surgery in smokers - Adams 2001), and the Diamond Concept (cells, scaffold, factors, stability). Be prepared to discuss exchange nailing technique and fibulectomy indications.
Controversies and Areas of Uncertainty
Both reliably heal aseptic, stable nonunions. Exchange nailing re-reams (autograft + larger nail) but exposes to canal contamination spread; augmentation plating retains the nail and controls rotation with lower morbidity. No definitive RCT favours one.
For infected segmental defects, acute shortening/lengthening had fewer complications than transport in comparative data (Tetsworth 2017), but transport avoids acute soft-tissue and neurovascular compromise. Choice remains case-specific.
rhBMP-2 reduces secondary interventions in open fractures (BESTT), but high cost, off-label nonunion use and heterotopic ossification temper routine use. BMAC and RIA graft are popular yet less rigorously proven.
The TRUST RCT found LIPUS did not accelerate union or improve function after tibial nailing, undermining routine use despite earlier enthusiasm and regulatory clearance.
The FDA 9-month definition is arbitrary; many advocate intervening earlier when no progression is seen for 3 months rather than waiting for an absolute time threshold.
Up to 20% of presumed aseptic nonunions yield positive cultures. The threshold for tissue sampling and the value of routine implant sonication are debated.
MCQ Practice Points
Q: What is the primary cause of a hypertrophic nonunion (Elephant Foot)? A: Inadequate Stability - The biology is sufficient (callus formation), but motion prevents bridging. Treatment is exchange nailing with larger diameter nail (greater than 90% success).
Q: What is the primary cause of an atrophic nonunion (Pencil Point)? A: Poor Biology - No callus formation, sclerotic bone ends, indicating biological failure. Treatment requires bone grafting (biology) + stable fixation (stability). Success rate 85-90%.
Q: What is the primary biological function of the induced membrane in the Masquelet technique? A: Secretes growth factors (VEGF, BMP-2) and provides vascularity - The membrane prevents soft tissue interposition and vascularizes the graft. Wait 6-8 weeks for membrane formation before Stage 2.
Q: When performing exchange nailing for a tibial nonunion, by how much should you over-ream? A: 1.5mm to 2mm larger than the existing canal/nail - This ensures fresh bleeding bone surfaces (autograft from reamings) and allows insertion of larger diameter nail for increased stability.
Q: When is a fibulectomy indicated in tibial nonunion surgery? A: When the fibula has healed and is strutting the tibia - The intact fibula prevents compression at the fracture site ('hold-open' effect). Excision of a small section allows compression and dynamization.
Q: What are the four pillars of the Diamond Concept for fracture healing? A: Osteogenic cells, Osteoconductive scaffolds, Growth factors, Mechanical environment - Systematic framework for analyzing why a nonunion occurred and how to treat it. Address all four pillars for success.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old smoker presents with a distal third tibial fracture treated with an IM nail 6 months ago. He has pain with weight bearing. X-rays show a transverse fracture line with sclerosis and no callus. He continues to smoke.”
“A 40-year-old man presents 8 months after tibial shaft fracture treated with IM nail. He has persistent pain with weight bearing. X-rays show abundant callus formation ('Elephant Foot') but the nail is broken at the nonunion site. The fracture line is still visible.”
“A 52-year-old man had a Gustilo IIIB open distal tibial fracture nailed 9 months ago. He now has a discharging sinus, pain at rest, and X-rays showing a lucent fracture line with a sequestrum. CRP is elevated. There is an estimated 4cm of devitalised bone.”
Classification
- Hypertrophic = Lack of stability
- Atrophic = Lack of biology
- Infected = Biofilm presence
- Oligotrophic = Mixed picture
Workup
- ESR / CRP (Infection screen)
- Vitamin D / Calcium / PTH (Metabolic)
- CT Scan (Assess bony bridging)
- WBC Scan (If infection ambiguous)
Treatment Choice
- Hypertrophic to Exchange Nail
- Atrophic to Bone Graft + Plate/Nail
- Infected to Debridement + Abx + Staged reconstruction
- Defect to Bone Transport or Masquelet
Key Concepts
- Dynamization (remove locking screws)
- Fibulectomy (remove 'hold-open' strut)
- Reamer Irrigator Aspirator (RIA) harvest
- Diamond Concept (Cells, Scaffold, Factors, Stability)
Evidence Base
Exchange Nailing for Aseptic Tibial Nonunion
- Reliable union in closed and lower-grade open aseptic nonunions
- Fails in type IIIb fractures with significant bone loss
- Wound infection is the commonest complication
Augmentation Plating Over a Retained Nail
- Plate added over a retained nail controls rotational instability nails resist poorly
- Tibial union 84.6% (11/13); femoral union 100% (25/25)
- Avoids the morbidity of nail removal and re-reaming
The Diamond Concept Applied to Long-Bone Nonunion
- Four pillars: cells, scaffold, growth factors, mechanical stability
- 98.4% union when all deficient pillars are addressed
- Provides a systematic diagnostic and treatment framework
Masquelet Induced-Membrane Technique
- Two-stage technique for critical-sized diaphyseal defects (4-25cm)
- Induced membrane is vascular and prevents graft resorption
- Preserve the membrane at stage 2 - it is the active biological element
Bone Transport vs Acute Shortening for Infected Defects
- Both techniques reliably achieve union and limb salvage
- Acute shortening/lengthening had fewer complications than transport
- Plan for docking-site grafting in most cases
rhBMP-2 in Open Tibial Fractures (BESTT Trial)
- rhBMP-2 1.50 mg/mL reduced secondary interventions by 44%
- Faster fracture and wound healing, fewer hardware failures
- Evidence base for osteoinductive augmentation in high-risk open fractures
LIPUS Does Not Accelerate Tibial Healing (TRUST Trial)
- No effect on radiographic union or functional recovery
- No reduction in nonunion rate vs sham
- Challenges routine LIPUS use after tibial nailing
Smoking and Open Tibial Fracture Healing
- Smoking prolongs union and increases need for secondary surgery
- Higher rates of flap failure, delayed union and nonunion
- Cessation advised to minimise complications