Pediatric ACL Equivalent | Meyers-McKeever Classification | Arthroscopic Fixation
- Pediatric ACL equivalent - tibial spine fracture in children = ACL injury in adults
- Meyers-McKeever classification guides treatment: Type I-II non-operative, Type III-IV surgical
- Intermeniscal ligament may block reduction in Type II and III - requires arthroscopic debridement
- Arthroscopic suture fixation is gold standard for Type III-IV (avoids hardware removal)
- Excellent outcomes with proper treatment: 85-95% good results, low complication rate
- “Tibial spine fracture = pediatric ACL injury - mechanism is hyperextension with valgus
- “Type II may be reducible with extension - if blocked by intermeniscal ligament, needs surgery
- “Arthroscopic suture fixation avoids hardware removal and allows early ROM
- “Complications: arthrofibrosis (5-10%), residual laxity (10-15%), growth disturbance (rare)
Tibial spine fracture in children = ACL injury in adults. Same mechanism (hyperextension with valgus), same instability pattern (anterior translation, pivot shift). Peak age 8-14 years. Meyers-McKeever classification guides treatment based on displacement.
Type I-II: Non-operative (extension cast). Type III-IV: Surgical (arthroscopic or open fixation). Type II may be reducible with extension - if blocked by intermeniscal ligament, needs arthroscopic debridement and fixation.
Gold standard for Type III-IV: Arthroscopic reduction and suture fixation through transosseous tunnels. Avoids hardware removal, allows early ROM, excellent outcomes (85-95% good results). Screw fixation alternative but requires removal.
Arthrofibrosis (5-10%): Most common - prevent with early ROM. Residual laxity (10-15%): May require revision. Growth disturbance (rare): Avoid crossing physis with fixation. Nonunion (rare): Usually with inadequate fixation.
- Displacement
- Less than 3mm
- Reducible?
- N/A - minimal
- Treatment
- Extension cast 4-6 weeks
- Displacement
- Anterior elevation
- Reducible?
- May be reducible
- Treatment
- Attempt closed reduction, cast if reducible
- Displacement
- Complete displacement
- Reducible?
- No - blocked
- Treatment
- Surgical fixation (arthroscopic preferred)
- Displacement
- Comminuted
- Reducible?
- No
- Treatment
- Surgical fixation (arthroscopic preferred)
Overview and Epidemiology
Tibial spine fractures (also called tibial eminence fractures) are avulsion fractures of the anterior tibial spine where the ACL inserts. These fractures represent the pediatric equivalent of ACL injuries in adults, occurring in skeletally immature patients before the ACL is strong enough to tear midsubstance.
Mechanism of Injury
Hyperextension with valgus force is the classic mechanism:
- Non-contact: Jumping/landing with knee hyperextension
- Contact: Direct blow to flexed knee causing hyperextension
- Bicycle accidents: Common in children (knee strikes handlebar)
- Sports: Soccer, basketball, gymnastics (landing with hyperextension)
The ACL inserts on the anterior tibial spine. In children, the bone is weaker than the ligament, so the ACL avulses the tibial spine rather than tearing midsubstance (as in adults).
In children, bone is weaker than ligament. The ACL insertion site (tibial spine) is cartilaginous and weak. Hyperextension force causes the ACL to avulse the tibial spine rather than tear midsubstance. This is why ACL injuries in children under 14 are almost always tibial spine fractures, not ligament tears.
Epidemiology
- Age: Peak 8-14 years (skeletally immature)
- Gender: Male predominance (2:1 ratio)
- Incidence: 3-5% of pediatric knee injuries
- Laterality: Usually unilateral, bilateral rare
- Associated injuries: Meniscal tears (10-20%), MCL injuries (5-10%)
Anatomy and Pathophysiology
Tibial Spine Anatomy
The anterior tibial spine (tibial eminence) is the bony prominence in the intercondylar notch where the ACL inserts:
- Location: Anterior intercondylar area of tibia
- Structure: Cartilaginous in children, ossifies with age
- ACL insertion: Anteromedial and posterolateral bundles attach here
- Blood supply: Middle genicular artery (same as ACL)
- Growth plate: Proximal tibial physis is 2-3cm distal - avoid crossing with fixation
Pathophysiology
- ACL is relatively strong (mature collagen)
- Tibial spine is cartilaginous and weak (immature bone)
- Hyperextension force → ACL avulses tibial spine (not ligament tear)
- Displacement depends on force magnitude and direction
- Tibial spine ossifies and strengthens
- ACL becomes relatively weaker
- Mechanism shifts from avulsion fracture to ligament tear
- Transition age: 14-16 years (skeletal maturity)
The proximal tibial physis is 2-3cm distal to the tibial spine. Fixation must avoid crossing the physis to prevent growth disturbance. Use transosseous tunnels that stay proximal to the physis, or use suture anchors in the tibial spine itself.
Classification System
Meyers-McKeever Classification (1959, modified by Zaricznyj 1977):
- Description
- Minimal displacement
- Displacement
- Less than 3mm elevation
- Radiographic Finding
- Minimal anterior elevation on lateral X-ray
- Description
- Anterior hinge intact
- Displacement
- Anterior 1/3-1/2 elevated
- Radiographic Finding
- Anterior elevation with posterior hinge visible
- Description
- Complete displacement
- Displacement
- No contact with bed
- Radiographic Finding
- Fragment completely separated, rotated
- Description
- Comminuted
- Displacement
- Multiple fragments
- Radiographic Finding
- Comminuted fragment, may be rotated
Key point: Type II may be reducible with knee extension (anterior hinge intact). If blocked by intermeniscal ligament, requires arthroscopic debridement and fixation.
Classification Systems
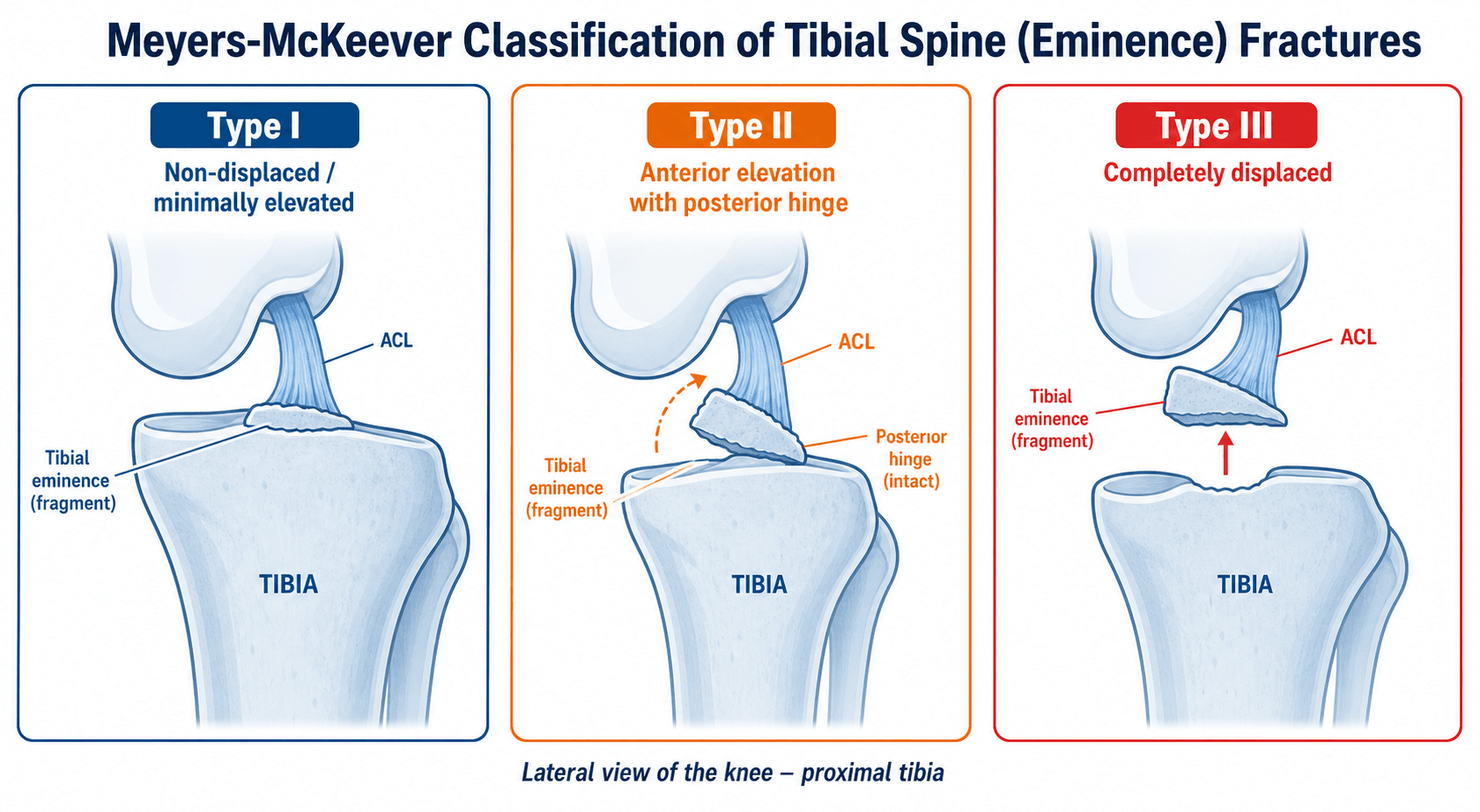
Meyers-McKeever Classification (Standard)
Type I: Minimal displacement (less than 3mm)
- Anterior edge slightly elevated
- Posterior hinge intact
- Treatment: Extension cast 4-6 weeks
Type II: Anterior hinge intact
- Anterior 1/3 to 1/2 elevated
- Posterior hinge maintains contact
- Treatment: Attempt closed reduction with extension, cast if reducible
Type III: Complete displacement
- Fragment completely separated
- No contact with tibial bed
- May be rotated
- Treatment: Surgical fixation (arthroscopic or open)
Type IV: Comminuted
- Multiple fragments
- May be rotated or displaced
- Treatment: Surgical fixation (arthroscopic or open)
This classification guides treatment decisions based on displacement and reducibility.
MACSTibial Spine Fracture Classification
Hook:Meyers-McKeever classification for ACL equivalent - Cast or Surgery based on displacement, Suture fixation is gold standard!
Clinical Assessment
History
Mechanism: Hyperextension with valgus force
- Jumping/landing with knee hyperextension
- Direct blow to flexed knee
- Bicycle accident (knee strikes handlebar)
- Sports: Soccer, basketball, gymnastics
Symptoms:
- Immediate pain and swelling
- Inability to bear weight
- Knee "giving way" (instability)
- Locking (if fragment blocks extension)
Physical Examination
Inspection:
- Knee effusion (hemarthrosis)
- Antalgic gait
- Knee held in slight flexion
Palpation:
- Tenderness over anterior tibial spine
- Joint line tenderness (if meniscal injury)
- MCL tenderness (if associated MCL injury)
Range of Motion:
- Limited flexion (pain, effusion)
- Limited extension (if fragment blocks)
- Extensor lag (if extensor mechanism affected)
Ligament Testing:
- Lachman test: Positive (anterior translation)
- Anterior drawer: Positive (anterior translation)
- Pivot shift: May be positive (rotational instability)
- Valgus stress: May be positive (if MCL injured)
Lachman test is positive in tibial spine fractures (same as ACL injury). The avulsed tibial spine allows anterior tibial translation. This is why tibial spine fractures are the pediatric ACL equivalent - same instability pattern, different injury mechanism.
Associated Injuries
- Meniscal tears: 10-20% (lateral meniscus more common)
- MCL injuries: 5-10%
- Bone bruises: Posterolateral tibia, lateral femoral condyle (kissing contusion)
- Extensor mechanism: Rare (patellar tendon avulsion)
Investigations
Standard X-ray Protocol
Views: AP and lateral knee. Oblique views if needed.
Key findings:
- Lateral view: Best for diagnosis and classification
- Anterior elevation: Fragment elevated from tibial bed
- Fragment size: Assess size and comminution
- Displacement: Measure displacement (Type I less than 3mm, Type III complete)
- Rotation: Assess fragment rotation
Lateral view is critical - shows displacement and classification.
AP view: May show fragment in intercondylar notch, but lateral is diagnostic.


Differential Diagnosis
The acutely swollen, haemarthrosis knee in a child has a focused differential. The tibial spine fracture is distinguished by the avulsed eminence on the lateral radiograph.
- Mechanism / clue
- Hyperextension/valgus; bicycle, sport
- Imaging
- Lateral X-ray: avulsed eminence
- Distinguishing feature
- Bony fragment at ACL footprint; Lachman positive
- Mechanism / clue
- Pivot/deceleration in older adolescent
- Imaging
- MRI: discontinuous ACL, no bony fragment
- Distinguishing feature
- No avulsion fragment; usually skeletally mature
- Mechanism / clue
- Twisting with quadriceps contraction
- Imaging
- Skyline / MRI: MPFL injury, medial patella bruise
- Distinguishing feature
- Lateral patellar apprehension; medial tenderness
- Mechanism / clue
- Shear during dislocation/twist
- Imaging
- X-ray/MRI: loose body, donor defect
- Distinguishing feature
- Mechanical locking, intra-articular fragment
- Mechanism / clue
- Direct/indirect force across physis
- Imaging
- X-ray: physeal widening, metaphyseal/epiphyseal line
- Distinguishing feature
- Tenderness over physis, not joint line
- Mechanism / clue
- Twist on planted foot
- Imaging
- MRI: meniscal signal
- Distinguishing feature
- Joint-line tenderness, no avulsion fragment
Loss of Reduction During Non-Operative Treatment
Non-operative care of a Type I or a reduced Type II fracture is an active, monitored process, not "cast and forget" — this answers the viva follow-up "What if it displaces to Type II in the cast?"
- Interval radiographs are mandatory. Films at roughly one to two weeks confirm the fragment has held its position; a marginally reduced Type II can re-elevate within the cast as swelling settles.
- Immobilisation angle is debated and matters. Near-full extension helps seat the anterior hinge of a Type II (the femoral notch presses the fragment down), but frank hyperextension can tension the ACL and lift the fragment, so a position of near-extension (commonly about 10 to 20 degrees of flexion) is often chosen to balance these effects.
- Loss of reduction changes the plan. If interval imaging shows progression to a displaced Type II or III, or a fragment now blocked by the interposed intermeniscal (transverse) ligament, abandon closed treatment and convert to arthroscopic reduction and fixation. Accepting a malunited, elevated fragment risks a mechanical extension block (the prominent fragment impinges in the intercondylar notch), residual laxity, and secondary arthrofibrosis.
Q: A Type I or reduced Type II tibial spine fracture is found to have displaced further on the two-week radiograph — what do you do? A: Do not accept malunion. A fragment that has lost reduction (progressed to a displaced Type II/III or become blocked by the intermeniscal ligament) is an indication to convert to arthroscopic reduction and fixation. This is precisely why interval radiographs during cast treatment are essential rather than optional.
Management Algorithm
Management Pathway
Tibial Spine Fracture Management
Determine Meyers-McKeever type. Assess reducibility for Type II. Check for associated injuries (meniscus, MCL).
Extension cast for 4-6 weeks. Non-weight bearing initially. Progressive weight bearing and ROM after cast removal.
Try closed reduction with knee extension. If reducible and stable, cast. If blocked by intermeniscal ligament, surgical.
Arthroscopic reduction and fixation (suture or screw). Open reduction if arthroscopic fails. Early ROM postoperatively.
Surgical Technique
Gold Standard Technique
Advantages:
- No hardware removal needed
- Allows early ROM
- Excellent visualization
- Low complication rate
Patient Positioning:
- Supine on standard table
- Tourniquet on thigh
- Leg holder or lateral post
- Standard arthroscopy setup
Portals:
- Anterolateral: Viewing portal
- Anteromedial: Working portal
- Superomedial: Optional outflow
Steps:
- Diagnostic arthroscopy (assess fragment, meniscus, cartilage)
- Debride intermeniscal ligament if blocking reduction
- Reduce fragment with probe or shaver
- Prepare fragment bed (debride to bleeding bone)
- Pass sutures through fragment (2-3 sutures)
- Create transosseous tunnels (2-3 tunnels, avoid physis)
- Pass sutures through tunnels
- Tie sutures over bone bridge (knee in extension)
- Confirm reduction and stability
Suture technique: Use No. 2 non-absorbable suture (Ethibond or Fiberwire). Pass through ACL insertion on fragment, then through transosseous tunnels.
Tunnel placement: Stay proximal to physis (2-3cm distal to joint line). Use 2-3 tunnels for stability.
Avoid crossing the proximal tibial physis with fixation. The physis is 2-3cm distal to the joint line. Use transosseous tunnels that stay proximal to the physis, or use suture anchors in the tibial spine itself. Crossing the physis can cause growth disturbance (rare but devastating).
SURGSurgical Indications
Hook:Surgery for Severe displacement, Unreducible fractures, Residual laxity, with Growth concern avoidance!
Complications
- Incidence
- 5-10%
- Risk Factors
- Delayed ROM, prolonged immobilization
- Prevention/Management
- Early ROM (2-4 weeks), aggressive PT
- Incidence
- 10-15%
- Risk Factors
- Malreduction, inadequate fixation
- Prevention/Management
- Anatomic reduction, secure fixation
- Incidence
- Less than 5%
- Risk Factors
- Inadequate fixation, poor reduction
- Prevention/Management
- Secure fixation, bone bed preparation
- Incidence
- Less than 1%
- Risk Factors
- Crossing physis with fixation
- Prevention/Management
- Avoid physis, use proximal tunnels
- Incidence
- 5-10% (screw)
- Risk Factors
- Prominent hardware, need for removal
- Prevention/Management
- Use suture fixation to avoid removal
- Incidence
- Long-term risk
- Risk Factors
- Malreduction, persistent instability
- Prevention/Management
- Anatomic reduction, restore stability
Arthrofibrosis
Most common complication (5-10%):
- Cause: Prolonged immobilization, delayed ROM
- Prevention: Early ROM (2-4 weeks), aggressive PT
- Management: Manipulation under anesthesia, arthroscopic lysis of adhesions
Residual Laxity
10-15% incidence:
- Cause: Malreduction, inadequate fixation, fragment resorption
- Prevention: Anatomic reduction, secure fixation
- Management: Revision fixation if symptomatic, ACL reconstruction if needed
Nonunion
Less than 5% incidence:
- Cause: Inadequate fixation, poor reduction, fragment devascularization
- Prevention: Secure fixation, bone bed preparation
- Management: Revision fixation with bone graft if needed
ALANComplications
Hook:Complications: Arthrofibrosis (most common), Laxity (residual), Arthritis (long-term), Nonunion (rare)!
Postoperative Care
Immediate Postoperative
- Immobilization: Hinged knee brace locked in extension (2-4 weeks)
- Weight bearing: Non-weight bearing initially (2-3 weeks)
- ROM: Begin passive ROM at 2-4 weeks (unlock brace)
- PT: Quadriceps sets, straight leg raises (immediate)
Rehabilitation Protocol
Weeks 0-2:
- Brace locked in extension
- Non-weight bearing
- Quadriceps sets, straight leg raises
- Ice and elevation
Weeks 2-4:
- Unlock brace for ROM (0-90 degrees)
- Progressive weight bearing (partial to full)
- Stationary bike (when ROM allows)
- Continue quadriceps strengthening
Weeks 4-6:
- Full ROM
- Full weight bearing
- Progressive strengthening
- Balance and proprioception
Weeks 6-12:
- Sport-specific training
- Return to sport (when strength and ROM normal)
- Continue PT for 3-6 months
Return to Sport
Criteria:
- Full ROM (equal to contralateral)
- Quadriceps strength greater than 90% of contralateral
- No instability (negative Lachman, pivot shift)
- Functional testing passed (hop test, agility)
Timeline: Usually 3-6 months postoperatively.
Outcomes and Prognosis
Overall Outcomes
Excellent outcomes with proper treatment:
- Type I-II (non-operative): 90-95% good/excellent results
- Type III-IV (surgical): 85-95% good/excellent results
- Long-term (5-10 years): 85-90% maintain good results
Functional Outcomes
Return to sport:
- Timeline: 3-6 months postoperatively
- Rate: 80-90% return to pre-injury level
- Factors: Age, sport level, rehabilitation compliance
Long-Term Prognosis
Residual laxity:
- 10-15% have some residual anterior laxity
- Usually asymptomatic (does not affect function)
- May require revision if symptomatic
Arthritis risk:
- Low risk with proper treatment (less than 5% at 10 years)
- Higher risk with malreduction or persistent instability
- Proper reduction and fixation minimize risk
Growth disturbance:
- Rare (less than 1%) with proper technique
- Avoid crossing physis with fixation
- Monitor until skeletal maturity if concern
Prevention and Return to Sport
Prevention
Primary prevention:
- Proper landing technique (knee flexion, not hyperextension)
- Strength training (quadriceps, hamstrings)
- Balance and proprioception training
- Sport-specific conditioning
Secondary prevention (after injury):
- Complete rehabilitation before return to sport
- Bracing (controversial - may not prevent reinjury)
- Continued strength and conditioning
Return to Sport Criteria
Clinical:
- Full ROM (equal to contralateral)
- Quadriceps strength greater than 90% of contralateral
- No effusion
- No instability (negative Lachman, pivot shift)
Functional:
- Single-leg hop test (greater than 90% of contralateral)
- Agility testing passed
- Sport-specific drills completed
Timeline: Usually 3-6 months postoperatively, depending on sport and level.
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence: ~3 per 100,000 per year; peak age 8-14 years; male predominance (~2:1).
- Represents roughly 2-5% of paediatric knee injuries with haemarthrosis; rising with youth sport participation.
- Bony ACL avulsion equivalent in the skeletally immature knee; adults more often tear the ACL mid-substance.
Society Guidance (Side by Side)
There is no formal single-society guideline dedicated to tibial spine fractures; the table summarises principles endorsed across major bodies and the Tibial Spine Research Interest Group consensus.
- Classification used
- Meyers-McKeever (+ MRI)
- Operative threshold
- Displaced (type III-IV); irreducible type II
- Emphasis
- Arthroscopic fixation, early ROM
- Classification used
- Meyers-McKeever
- Operative threshold
- Displaced / blocked reduction
- Emphasis
- Refer to paediatric centre, MRI for associated injury
- Classification used
- Meyers-McKeever / OTA
- Operative threshold
- Articular incongruity or instability
- Emphasis
- Stable fixation that respects the physis
- Classification used
- Meyers-McKeever
- Operative threshold
- Displaced; meniscal entrapment
- Emphasis
- Suture over screw; meniscal preservation
Registries and Practice Variation
- Joint registries (NJR, AJRR, AOANJRR, SHAR) do not track tibial spine fixation; they are relevant only for the rare late ACL reconstruction or arthroplasty after malreduction and post-traumatic arthritis.
- High-resource settings: arthroscopic reduction with suture fixation is the prevailing standard, enabling early motion.
- Limited-resource settings: open reduction and internal fixation (screw or suture over bone bridge) remains common and effective where arthroscopy or implants are unavailable; outcomes are good when reduction is anatomic and rehabilitation is supervised.
Controversies and Areas of Uncertainty
Suture (pull-through or suture-bridge) fixation avoids a second operation for implant removal and shows higher patient-reported scores in a randomised trial and systematic review, but screws give immediate compression and excellent results in large series. Choice often reflects fragment size, comminution and surgeon experience rather than proven superiority for every case.
The classic "3 mm" cut-off and the reducibility of type II fractures are debated. Many type II fractures are blocked by the intermeniscal (transverse) ligament or entrapped meniscus, so post-reduction radiographs and a low threshold for arthroscopy are increasingly favoured over a fixed millimetre rule.
MRI is not mandatory but detects entrapped soft tissue, chondral injury and meniscal tears (reported in a notable minority) and refines classification. Routine versus selective MRI remains practice-dependent.
Mild residual anterior laxity (Lachman/KT-1000) is common after healing but is usually asymptomatic and rarely requires later ACL reconstruction. Whether this laxity predisposes to long-term degenerative change is not yet settled.
Residual Anterior Laxity: Why It Persists After Anatomic Union
The topic repeatedly notes that mild anterior laxity is common even when the fragment heals perfectly, but the reason deserves explanation because it is a favourite examiner probe. The anterior cruciate ligament does not fail cleanly at the instant the eminence avulses: it is first plastically (interstitially) elongated — the ligament stretches beyond its elastic limit as the bony attachment peels off. Restoring the bony fragment to its bed therefore restores the footprint but cannot shorten an already-lengthened ligament, so a degree of anterior translation may persist.
- Instrumented testing detects it more than patients do: side-to-side differences on Lachman and KT-1000 arthrometry are found more often than the child reports any symptom. Most such laxity is mild, functionally silent, and does not require later ACL reconstruction — consistent with the excellent Lysholm scores and absence of clinical laxity reported in the operative series in the Evidence Base.
- Clinically important laxity is the minority (the roughly 10-15% figure used throughout this topic) and clusters with malreduction, fragment resorption, inadequate fixation, or a missed concomitant ligamentous injury rather than with the plastic-elongation mechanism alone.
- Do not conflate with a mid-substance ACL tear — the primary treatment of a torn ACL and its reconstruction are covered on the dedicated ACL topics; here the ligament is in continuity but lengthened.
Q: Why can a patient have a positive Lachman test after a tibial spine fracture that has healed in anatomic position? A: The ACL is plastically elongated (interstitial stretch) at the moment of avulsion, so anatomic bony reduction cannot shorten the already-lengthened ligament. The resulting laxity is usually mild and asymptomatic; symptomatic instability instead points to malreduction, fragment resorption, or a missed associated ligament injury.
MCQ Practice Points
Q: What is the most common complication following tibial spine fracture fixation? A: Arthrofibrosis (5-10%) - Stiffness is more common than instability or nonunion. Prevention requires early ROM.
Q: Why do children sustain tibial spine fractures instead of ACL tears? A: Bone is weaker than ligament - The cartilaginous tibial spine avulses before the collagen of the ACL fails midsubstance.
Q: What is the absolute indication for surgery in Meyers-McKeever classification? A: Type III (Complete displacement) - Also Type II if reducible but blocked by meniscus (intermeniscal ligament).
Q: How does ACL function compare between anatomically healed tibial spine fractures and native ACL? A: Normal function expected - Studies show 95% of patients achieve normal Lachman and KT-1000 testing when healed in anatomic position.
Q: What structure may block reduction of a displaced tibial spine fracture? A: Intermeniscal ligament (transverse ligament) - It can become interposed between the fragment and its bed, preventing closed reduction.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old boy presents after falling off a bicycle. Knee is swollen. X-ray shows Meyers-McKeever Type I tibial spine fracture.”
“A 12-year-old female gymnast lands awkwardly. X-ray shows a Type III tibial spine fracture (completely displaced).”
“A patient returns 3 months after fixation of a tibial spine fracture with a 15-degree extension deficit.”
Key Concepts
- Pediatric ACL Equivalent
- Meyers-McKeever Classification
- Hyperextension + Valgus mechanism
- Lachman positive (anterior laxity)
Classification (Meyers-McKeever)
- Type I: Non-displaced → Extension Cast
- Type II: Hinge intact → Reduce/Cast or Surgery
- Type III: Complete → Surgery
- Type IV: Comminuted → Surgery
Surgical Goals
- Anatomic reduction
- Stable fixation (suture preferred over screw)
- Avoid Physis (Growth plate protection)
- Early ROM (Prevent arthrofibrosis)
Complications
- Arthrofibrosis (Most common)
- Residual Laxity (Usually asymptomatic)
- Growth Disturbance (Rare)
- Nonunion (Rare)
Pearl
- Intermeniscal ligament often blocks reduction
- Lateral meniscus tear is most common associated injury
- Lateral X-ray is diagnostic view
- Arthroscopic suture fixation is gold standard
Evidence Base
Meyers-McKeever Classification
- Original radiographic classification (Type I-III) based on displacement of the fragment
- Type I-II reduce with extension and do well non-operatively
- Type III (complete separation) requires reduction and fixation
State of the Art Review (Incidence and Principles)
- Incidence approximately 3 per 100,000 per year, peak age 8-14 years
- Tibial spine fracture is the bony ACL avulsion equivalent in skeletally immature knees
- Most common complications: arthrofibrosis, residual laxity, nonunion/malunion, physeal arrest
Surgical Treatment - Systematic Review (ARIF vs ORIF, Suture vs Screw)
- 12 studies pooled for Meyers-McKeever type II-IV operative outcomes
- Arthroscopic suture fixation gave higher Tegner/IKDC/Lysholm scores than arthroscopic screw fixation (p less than 0.001)
- Screw fixation had higher implant-removal rates; suture fixation had higher arthrofibrosis rates
Arthroscopic Suture vs Screw Fixation - Randomised Trial
- Randomised trial of 90 patients (45 suture vs 45 screw) with tibial ACL avulsion
- Suture group superior subjective IKDC (91.4 vs 85.7) and Lysholm (92.0 vs 86.0), both p=0.001
- 7 screw-fixation patients required reoperation for implant removal; none in the suture group
Arthroscopic Screw Fixation (Type II-III)
- 24 children (mean age 11y), Meyers-McKeever type II (n=15) and III (n=9), intra-epiphyseal ASNIS screws
- Mean Lysholm 99.3 (type II) and 98.6 (type III); no anterior laxity at 12 weeks
- Meniscal entrapment present in 12 cases without affecting functional result
Arthrofibrosis After Surgical Fixation
- 32 children/adolescents who developed arthrofibrosis after fixation of displaced tibial eminence fractures
- 24 required reoperation for loss of motion; manipulation under anaesthesia caused distal femoral fracture and growth arrest in 3
- Stable fixation enabling early rehabilitation is key; manipulation should be combined with lysis of adhesions
Complications - Prevention and Treatment
- Tibial eminence fixation may be complicated by failed fixation, knee stiffness and arthrofibrosis
- Arthrofibrosis is rare in children overall but occurs most frequently after tibial eminence injuries
- Emphasises secure fixation and early controlled motion to limit stiffness