Diagnostic Criteria | Treatment Algorithm | Prevention Strategies
- MSIS criteria requires 1 major (sinus tract, purulence) OR 4/6 minor criteria for definite PJI
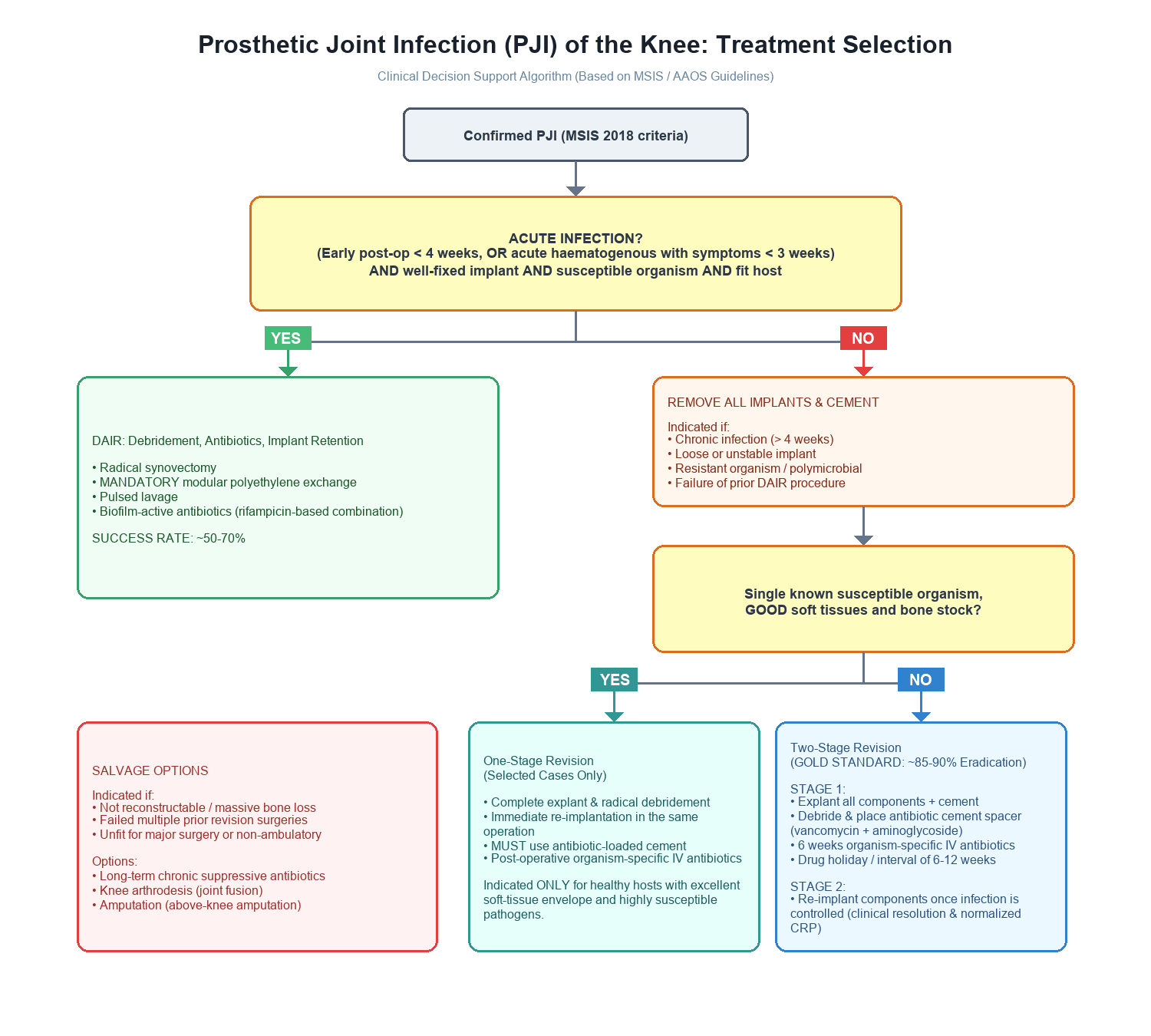
- DAIR indications: Early infection (under 4 weeks), acute hematogenous (symptoms under 3 weeks), stable implant, non-resistant organism
- 2-stage revision is gold standard for chronic PJI: sensitivity 90-95%, specificity 75-80% for eradication
- Antibiotic cement spacer maintains joint space, delivers local antibiotics (4-6g vancomycin + 3-4g aminoglycoside per 40g cement)
- Risk factors: Diabetes (OR 2.5), obesity (BMI over 30: OR 2.0), rheumatoid arthritis (OR 2.4), previous surgery (OR 3.7)
- “MSIS 2018 criteria are Orthopaedic exam standard - know the scoring system (1 major = definite, 6 points = definite, 2-5 points = possible)
- “Alpha-defensin synovial fluid test: sensitivity 97%, specificity 96% for PJI diagnosis
- “Antibiotic holiday: minimum 2 weeks (ideally 6 weeks) before obtaining cultures for optimal yield
- “Streptococcus agalactiae (Group B Strep) is dental prophylaxis indication even in presence of prosthetic joint
1 major criterion = definite PJI. Major: sinus tract or purulence. Minor: elevated CRP/ESR, positive alpha-defensin, elevated synovial WCC/PMN%, positive culture, positive histology. Score 6 or more = definite.
KLIC score predicts DAIR failure (Tornero 2015). K: kidney (chronic renal failure). L: liver cirrhosis. I: index surgery (revision or fracture). C: cemented prosthesis. Plus CRP over 11.5 mg/dL. Failure rises from approximately 4.5% (score 2 or less) to 100% (score 7 or greater).
4-6g vancomycin + 3-4g aminoglycoside per 40g cement. Maximum 10% antibiotic by weight to maintain mechanical properties. Static (block) vs articulating (mobile) - similar infection eradication, articulating better function.
No evidence that longer interval improves eradication. Standard: 6-12 weeks based on CRP normalization and clinical resolution. Some centres: 2-4 weeks for virulent organisms with good spacer function.
- Classification
- Type I - Early
- Treatment
- DAIR + organism-specific IV antibiotics 6 weeks
- Key Pearl
- Success 50-60% if under 3 weeks, organism sensitive
- Classification
- Type III - Acute hematogenous
- Treatment
- DAIR + antibiotics if implant stable, organism not resistant
- Key Pearl
- Window of opportunity: under 3 weeks symptom duration
- Classification
- Type II - Late chronic
- Treatment
- 2-stage revision with antibiotic spacer 6-12 weeks
- Key Pearl
- Gold standard: 90% eradication, but 2 surgeries required
- Classification
- Salvage scenario
- Treatment
- Resection arthroplasty OR suppressive antibiotics
- Key Pearl
- Last resort: arthrodesis rarely feasible in knee
STEADIDAIR Indications
Hook:Keep it STEADI for DAIR success - timing, organism, and implant stability are everything!
Overview and Epidemiology
Periprosthetic joint infection is the most devastating complication following TKA. It represents 25% of all revision TKA burden (AOANJRR 2023), with higher mortality than hip fracture at 1 year (7% vs 4%). The economic burden is enormous: 2-stage revision costs approximately $100,000-150,000 AUD, with prolonged disability averaging 6-12 months from diagnosis to full recovery. Success rates plateau at 60-90% infection eradication depending on organism and host factors, meaning 10-40% face salvage procedures (resection arthroplasty, arthrodesis, or amputation).
- Primary TKA: 1-2% infection rate
- Revision TKA: 3-5% infection rate
- Bimodal distribution: Early (under 3 months) vs late (over 2 years)
- Mean age at diagnosis: 68 years (range 45-85)
- Male predominance: 1.4:1 (conflicting data - some show female predominance)
- Increasing incidence: Absolute numbers rising with TKA volume growth
- Hospital costs: $100,000-150,000 AUD per 2-stage revision
- Extended LOS: 10-14 days first stage, 7-10 days second stage
- Lost productivity: 6-12 months total recovery time
- Re-infection rate: 10-30% require further revision
- Litigation risk: 15% of PJI cases result in medicolegal action
- Mortality: 1-year mortality 7% (higher than hip fracture)
Diagnostic Criteria: MSIS 2018 Definition
The Musculoskeletal Infection Society (MSIS) 2018 criteria are the international standard for PJI diagnosis. The Orthopaedic examiners expect fluency with this scoring system.
Diagnostic Framework
DEFINITE infection if any of:
- 1 Major criterion present, OR
- Score 6 or greater from minor criteria, OR
- ICM 2018: Minor criteria score 2-5 = Possible infection (treat as infection if clinical suspicion high)
Major Criteria (Either = Definite PJI)
Communicating sinus tract from skin to prosthesis confirmed by:
- Direct visualization at surgery
- Sinogram/fistulogram demonstrating connection
- Probing to prosthesis through skin wound
Specificity 100% - pathognomonic for infection.
Gross purulence in:
- Joint aspiration (pre-op)
- Intraoperative tissue/fluid
Must be purulent appearance (not just turbid). Examiner may ask: "What if cloudy but not frankly purulent?" Answer: Score as minor criteria (elevated WCC/PMN).
Minor Criteria Scoring System
- Threshold
- Greater than 10 mg/L
- Points
- 1 point
- Notes
- Non-specific. Elevated in 80% PJI but also inflammatory arthritis
- Threshold
- Greater than 860 ng/mL
- Points
- 2 points
- Notes
- High sensitivity (89%) but low specificity (65%). Added in ICM 2018
- Threshold
- Greater than 30 mm/hr
- Points
- 1 point
- Notes
- Non-specific. Less useful than CRP
- Threshold
- Greater than 3000 cells/μL
- Points
- 2 points
- Notes
- Lower threshold if chronic (3000) vs acute (10,000). TKA: 3000 is standard
- Threshold
- Greater than 70%
- Points
- 1 point
- Notes
- Polymorphonuclear cell predominance. Counts as same test as WCC (do not double-score)
- Threshold
- Positive (signal-to-cutoff ratio over 1.0)
- Points
- 3 points
- Notes
- 97% sensitivity, 96% specificity. Best single synovial marker
- Threshold
- ++
- Points
- 3 points
- Notes
- Point-of-care test. Positive (++) = 3 points, + = 2 points
- Threshold
- Same organism from 2 or more samples
- Points
- 3 points
- Notes
- Single positive = 2 points. Virulent organisms (S. aureus) = 2 points if single culture
- Threshold
- Greater than 5 PMN/hpf in 5 hpf (400x)
- Points
- 3 points
- Notes
- Intraoperative frozen section or permanent. Type II/III interface membrane
Viva scenario: 72-year-old, TKA 18 months ago, 3-week history knee pain and effusion. CRP 45, ESR 55, synovial WCC 8000, PMN 85%, alpha-defensin positive, culture negative.
Answer: "This meets MSIS criteria for definite PJI with score of 9 points: CRP over 10 (1 point), ESR over 30 (1 point), synovial WCC over 3000 (2 points), PMN over 70% (1 point - note we do not double-score WCC and PMN, count only WCC 2 points), alpha-defensin positive (3 points). Total = 1 + 1 + 2 + 3 = 7 points, which exceeds threshold of 6 for definite infection. I would proceed with treatment for PJI despite negative cultures - likely prior antibiotic exposure."
Common trap: Students double-count synovial WCC and PMN%. Only count the WCC (2 points) when both are positive.
Investigations Protocol
Diagnostic Workup Sequence
Blood tests:
- CRP (threshold over 10 mg/L)
- ESR (threshold over 30 mm/hr)
- D-dimer (threshold over 860 ng/mL) - ICM 2018 addition
- WCC (usually normal unless acute severe infection)
Sensitivity: CRP 80%, ESR 75%, D-dimer 89% Specificity: CRP 70%, ESR 65%, D-dimer 65%
Interpretation: Elevated markers increase suspicion but are non-specific. Normal CRP does not exclude PJI (20% of chronic PJI have normal CRP, especially low-virulence CNS).
Technique:
- Lateral or superolateral approach to avoid suprapatellar pouch (higher yield)
- Send: Cell count/differential, culture (aerobic + anaerobic, hold 14 days), alpha-defensin
- Volume: Minimum 3-5 mL for adequate culture yield
Antibiotic holiday: Minimum 2 weeks off antibiotics (ideally 6 weeks)
Synovial fluid analysis:
- WCC over 3000 cells/μL = 2 points
- PMN over 70% = 1 point (do not double-score with WCC)
- Alpha-defensin positive = 3 points (best single marker: 97% sensitivity, 96% specificity)
Culture yield: 65-90% sensitivity (higher if off antibiotics 6 weeks)
Plain radiographs:
- Progressive periprosthetic lucency (over 2mm or progressive)
- Periosteal reaction
- Component subsidence or migration
- Sensitivity 50% (late finding)
Nuclear medicine:
- Bone scan: Sensitive (90%) but non-specific (50%)
- Labeled WBC scan + sulfur colloid: 90% sensitivity, 85% specificity for PJI
- PET-CT: Emerging, 85-95% sensitivity but expensive
MRI: Limited by metal artifact. Consider MARS (metal artifact reduction) sequences.
Sample collection:
- Minimum 3-5 tissue samples from different sites (capsule, interface, bone)
- Avoid superficial tissue (contamination risk)
- Send for culture (aerobic, anaerobic, fungal if immunosuppressed) AND histology
Frozen section:
- Over 5 PMN/hpf in 5 hpf at 400x = positive for infection
- Sensitivity 80-85%, specificity 90-95%
- Result in 20-30 minutes intraoperatively
Permanent histology:
- Type II/III interface membrane (lymphocytic infiltration)
- More sensitive than frozen section but delayed result
SPACEDMSIS Major and Minor Criteria
Hook:PJI diagnosis is SPACED out: 2 MAJOR criteria (Sinus, Purulence) give instant diagnosis, then score the minor criteria!
Pathophysiology and Microbiology
Biofilm Formation
The hallmark of PJI is bacterial biofilm formation on the prosthetic surface. This occurs in stages:
- Attachment (0-4 hours): Bacteria adhere to implant surface via adhesins
- Accumulation (4-24 hours): Microcolony formation with extracellular matrix production
- Maturation (1-7 days): Three-dimensional biofilm structure with nutrient channels
- Detachment (ongoing): Planktonic bacteria shed from biofilm to colonize new areas
Clinical significance: Biofilm bacteria are 100-1000x more resistant to antibiotics than planktonic forms. Minimum biofilm eradication concentration (MBEC) exceeds achievable systemic antibiotic levels for most organisms, necessitating implant removal for chronic infection.
Biofilm-protected bacteria resist host immunity and antibiotics. This explains why DAIR fails in chronic infection (over 4 weeks): mature biofilm cannot be eradicated with antibiotics alone. Only fresh biofilm (under 3 weeks) or acute contamination (under 4 weeks post-surgery) has sufficient antibiotic susceptibility for retention strategies. Beyond this window, implant removal is mandatory for infection clearance.
Microbiology Profile
- Frequency
- 30-40%
- Virulence
- High virulence, acute presentation
- Treatment Considerations
- DAIR possible if early. Rifampicin + flucloxacillin biofilm penetration
- Frequency
- 5-15%
- Virulence
- High virulence, resistant
- Treatment Considerations
- DAIR contraindicated. Vancomycin + rifampicin. Higher failure rates
- Frequency
- 25-35%
- Virulence
- Low virulence, chronic/late
- Treatment Considerations
- Often antibiotic-resistant. 2-stage usually required
- Frequency
- 8-12%
- Virulence
- Moderate virulence
- Treatment Considerations
- DAIR success higher if acute. Penicillin-based therapy
- Frequency
- 5-10%
- Virulence
- Variable, often nosocomial
- Treatment Considerations
- Fluoroquinolone + rifampicin. P. aeruginosa difficult to eradicate
- Frequency
- 10-15%
- Virulence
- High biofilm burden
- Treatment Considerations
- Poor prognosis. 2-stage mandatory
- Frequency
- 5-10%
- Virulence
- Unknown organism
- Treatment Considerations
- Broad-spectrum empiric therapy. Consider biofilm dispersal agents
Minimum 2 weeks antibiotic-free interval (ideally 6 weeks) before obtaining cultures is essential for optimal organism identification. Antibiotics suppress planktonic bacterial release from biofilm without eradicating infection, leading to false-negative cultures in 30-40% if obtained on antibiotics. However, in acutely unwell patients, cultures should be obtained urgently without waiting, as organism identification guides definitive treatment even if delayed.
Classification Systems
Tsukayama Classification (Most Clinically Useful)
Based on timing and presentation, which guides treatment selection.
- Definition
- Under 4 weeks post-surgery
- Treatment
- DAIR + antibiotics 6 weeks
- Success Rate
- 50-70% if under 3 weeks, organism sensitive
- Definition
- Over 4 weeks post-surgery
- Treatment
- 2-stage revision
- Success Rate
- 85-90% eradication with 2-stage
- Definition
- Acute onset (under 3 weeks symptoms) in previously well-functioning TKA
- Treatment
- DAIR if under 3 weeks symptoms, stable implant, sensitive organism
- Success Rate
- 60-75% if window under 3 weeks, drops to 30% if over 3 weeks
- Definition
- Unexpected positive cultures during aseptic revision
- Treatment
- Organism-specific antibiotics 6 weeks (no implant removal if stable)
- Success Rate
- 90% success if single organism, low virulence
Type III (acute hematogenous) PJI is time-critical. DAIR success is 75% if symptoms under 3 weeks, but drops to 30% if over 3 weeks symptom duration. This is independent of time since index surgery - even a 5-year-old TKA with acute onset (fell, developed pain/fever/effusion, presenting 2 weeks later) qualifies for DAIR if symptom duration is under 3 weeks. Examiners may ask: "TKA 5 years ago, 2-week history of pain - DAIR or 2-stage?" Answer: "Depends on symptom duration and implant stability - if truly acute onset under 3 weeks and stable implant, DAIR is reasonable. If insidious onset suggesting chronic smoldering infection, 2-stage preferred."
This classification guides treatment pathways better than alternatives.
Clinical Assessment
History Taking
Timeline:
- Time since index surgery (early under 4 weeks vs late over 4 weeks)
- Symptom onset (acute under 3 weeks vs insidious chronic)
- Ever pain-free postoperatively? (No = concerning for persistent infection)
Symptoms:
- Pain: Constant vs activity-related. Night pain (infection hallmark)
- Swelling: Progressive effusion
- Warmth/erythema: Local inflammation
- Drainage: Persistent wound drainage over 7 days (high PJI risk)
- Systemic: Fever, chills, night sweats (acute infection)
Function:
- Sudden loss of function after good initial recovery (suggests acute infection)
- Never achieved good function (suggests early chronic infection)
Patient factors:
- Diabetes (HbA1c current and perioperative)
- Obesity (BMI at surgery)
- Immunosuppression (steroids, biologics, chemotherapy)
- Smoking status
- Rheumatoid arthritis or inflammatory arthritis
- Previous joint surgery (infection risk OR 3.7)
- Chronic kidney disease, liver disease
Perioperative factors:
- Wound complications (dehiscence, hematoma, prolonged drainage)
- Postoperative blood transfusion
- Return to OR for any reason under 90 days
- Recent bacteremia (dental, urinary, skin infection)
Any of these findings require urgent investigation for PJI:
- Persistent wound drainage over 7 days post-surgery
- Acute onset pain in previously well-functioning TKA (acute hematogenous)
- Never pain-free after surgery (early chronic infection)
- Systemic symptoms: Fever, rigors, sepsis
- Sinus tract: Visible drainage from wound to joint (pathognomonic for PJI)
- Rapid onset stiffness with loss of previously achieved range of motion
Physical Examination
Systematic Examination
Wound:
- Erythema (diffuse vs localized)
- Swelling (effusion vs soft tissue edema)
- Sinus tract or draining wound (MAJOR criterion if communicates with prosthesis)
- Surgical scars (assess healing, any dehiscence)
Limb:
- Leg alignment (varus/valgus deformity suggests loosening)
- Muscle wasting (chronic infection impairs function)
- Skin changes (chronic venous stasis, dependent rubor)
Local temperature: Warmth over joint (compare to contralateral)
Effusion: Moderate to large effusion common in PJI (but also aseptic loosening)
Tenderness: Diffuse joint line tenderness (infection) vs focal (mechanical)
Lymphadenopathy: Inguinal nodes may be enlarged in chronic infection
Range of motion:
- Active and passive ROM (stiffness suggests infection or arthrofibrosis)
- Painful arc or end-range pain
- Loss of ROM compared to prior assessments (concerning for infection)
Stability:
- Varus/valgus stress (loosening vs intact collaterals)
- Anteroposterior drawer (implant stability)
Crepitus: Suggests polyethylene wear or loosening (not specific for infection)
Neurovascular assessment:
- Pulses (dorsalis pedis, posterior tibial)
- Sensation (common peroneal nerve distribution - dorsal foot)
- Motor (ankle dorsiflexion - common peroneal; plantarflexion - tibial)
Systemic examination:
- Temperature (fever in acute infection)
- Signs of sepsis (tachycardia, hypotension, confusion in severe cases)
Examiners often ask: "How do you clinically distinguish infection from aseptic loosening?"
Answer: "Clinical differentiation is difficult - both present with pain and effusion. However, infection tends to have:
- (1) Earlier onset (within 2 years) vs aseptic loosening (over 5 years typically)
- (2) Acute or subacute symptoms (weeks) vs insidious chronic pain (months to years)
- (3) Systemic features (fever, night sweats) vs purely mechanical symptoms
- (4) Constant pain including night pain vs activity-related pain relieved by rest
- (5) Warmth and erythema over joint vs normal overlying skin
However, definitive diagnosis requires MSIS criteria with serology, aspiration, and imaging. I maintain low threshold for aspiration in any painful TKA - better to over-investigate than miss infection. Clinical suspicion guides investigation, not diagnosis."
Differential Diagnosis of the Painful TKA
Every painful TKA must be screened for infection first, but the differential is broad. PJI and aseptic causes can coexist, so aspiration is the discriminating test.
- Typical features
- Rest/night pain, effusion, warmth, raised CRP/ESR, possible sinus or drainage
- Key discriminator
- MSIS criteria positive; positive aspirate (raised synovial WCC/PMN, alpha-defensin, culture)
- Typical features
- Activity-related start-up pain, usually over 2-5 years, progressive lucency
- Key discriminator
- Normal inflammatory markers and sterile aspirate; radiographic loosening
- Typical features
- Mechanical symptoms, giving way, recurrent effusion, wear on imaging
- Key discriminator
- Sterile aspirate; instability on stress exam; wear pattern on radiographs
- Typical features
- Acute pain after trauma, deformity, inability to weight-bear
- Key discriminator
- Fracture on radiographs; trauma history
- Typical features
- Acute hot swollen joint, may mimic acute PJI
- Key discriminator
- Crystals on synovial polarised microscopy; cultures negative
- Typical features
- Pain not localised to joint line, normal local exam and aspirate
- Key discriminator
- Examine hip and spine; normal joint markers; consider vascular/neuropathic causes
- Typical features
- Anterior pain, extensor lag, crepitus, no systemic features
- Key discriminator
- Focal tendon/patellar signs; sterile aspirate; dynamic imaging
Investigations
The investigative approach follows a stepwise protocol from serum markers to imaging to aspiration, culminating in intraoperative sampling if surgery is required.
Diagnostic Investigation Protocol
Tests to order:
- CRP (threshold over 10 mg/L = 1 MSIS point)
- ESR (threshold over 30 mm/hr = 1 MSIS point)
- D-dimer (threshold over 860 ng/mL = 2 MSIS points) - ICM 2018 addition
- WCC (usually normal unless acute severe infection)
Interpretation:
- Sensitivity: CRP 80%, ESR 75%, D-dimer 89%
- Specificity: CRP 70%, ESR 65%, D-dimer 65%
- Non-specific: Elevated in inflammatory arthritis, recent surgery, obesity
- Normal CRP does NOT exclude PJI: 20% of chronic low-virulence CNS infections have normal CRP
Serial markers: Trend more useful than single value (rising CRP concerning even if under 10)
Plain radiographs (AP, lateral, skyline views):
- Lucency: Greater than 2mm periprosthetic lucency (suggests loosening, may be septic or aseptic)
- Progressive lucency: Serial films showing widening (infection or loosening)
- Periosteal reaction: New bone formation along femoral or tibial cortex (chronic infection)
- Subsidence: Component migration (loosening - cause unclear without aspiration)
- Sensitivity: 50% only (late finding)
Utility: Rules out obvious loosening/osteolysis but does NOT diagnose infection
Critical preparatory step: Antibiotic holiday minimum 2 weeks (ideally 6 weeks) before aspiration
Technique:
- Sterile prep (chlorhexidine, drape)
- Approach: Lateral or superolateral (avoids suprapatellar pouch - better yield)
- Volume: Aspirate minimum 3-5 mL for adequate culture and cell count
- Send: Cell count/differential, culture (aerobic + anaerobic + fungal if immunosuppressed, hold 14 days), alpha-defensin, leukocyte esterase
Synovial fluid analysis (MSIS scoring):
- WCC over 3000 cells/μL = 2 points
- PMN over 70% = 1 point (do NOT double-score with WCC - count only WCC 2 points)
- Alpha-defensin positive = 3 points (best single marker: 97% sens, 96% spec)
- Leukocyte esterase ++ = 3 points (point-of-care, + = 2 points)
Culture yield: 65-90% sensitivity (higher if adequate antibiotic holiday)
Dry tap: If aspiration yields no fluid, consider saline injection (5-10mL sterile saline, agitate knee, re-aspirate) to lavage joint and improve yield
Nuclear medicine:
- Bone scan (Tc-99m MDP): Sensitive (90%) but non-specific (50%) - positive in infection AND aseptic loosening
- Labeled WBC scan (In-111 or Tc-99m HMPAO): 85% sensitivity, 80% specificity for infection
- Combined WBC + sulfur colloid: Improves specificity to 85% (photopenic mismatch suggests infection)
PET-CT:
- Emerging modality
- Sensitivity 85-95%, specificity 80-90%
- Expensive, limited availability
- Useful if aspiration non-diagnostic and high clinical suspicion
MRI: Limited by metal artifact. MARS (metal artifact reduction sequences) may help assess soft tissue but does NOT reliably diagnose PJI
Sample collection protocol:
- Minimum 5-6 tissue samples from different sites (capsule, bone-implant interface, femoral canal, tibial plateau, medial gutter, lateral gutter)
- Avoid superficial tissue (contamination risk)
- Send for: Aerobic culture, anaerobic culture, fungal culture (if immunosuppressed), permanent histology
- Hold cultures 14 days for slow-growing organisms
Frozen section histology:
- Threshold: Over 5 PMN/hpf in 5 high-power fields at 400x magnification = positive for infection
- Sensitivity 80-85%, specificity 90-95%
- Result in 20-30 minutes - allows intraoperative decision (proceed with reimplantation vs abort)
Permanent histology:
- Type II/III interface membrane (lymphocytic infiltration with PMN predominance)
- More sensitive than frozen section but delayed result (3-5 days)
- Useful for confirmation if frozen section borderline
Intraoperative purulence: MAJOR criterion (definite PJI) - if frankly purulent fluid/tissue encountered, infection confirmed regardless of cultures
Concept: When components are removed, sonication of the explanted prosthesis in a sealed container uses ultrasound to dislodge adherent biofilm bacteria from the implant surface; the resulting sonicate fluid is then cultured. This samples organisms where they actually live (on the implant) rather than relying on periprosthetic tissue alone.
Evidence (Trampuz, NEJM 2007):
- Sonicate-fluid culture sensitivity 78.5% vs periprosthetic-tissue culture 60.8% (specificity similar, around 99%)
- Advantage greatest in patients given antibiotics within 14 days before surgery (sensitivity 75.0% vs 45.0% for tissue) - exactly the prior-antibiotic / culture-negative scenario this chapter highlights
Use: A key adjunct for culture-negative PJI and any case with recent antibiotic exposure; combine with multiple tissue cultures and prolonged incubation. (Generic biofilm science is developed in the biofilm-formation topic.)
If asked "cultures are negative but you strongly suspect infection - how do you improve the microbiological yield?", a high-value answer is sonication of the explanted implant. Because organisms live in biofilm on the prosthesis, sonicate-fluid culture is more sensitive than periprosthetic-tissue culture (78.5% vs 60.8%, Trampuz NEJM 2007), and the gap widens to 75% vs 45% when the patient had antibiotics in the preceding 14 days. Pair it with multiple tissue samples, prolonged incubation (14 days for indolent organisms such as Cutibacterium), and an adequate antibiotic holiday.
Management Algorithm
Treatment Selection Framework
DAIR Protocol
Concept: Aggressive surgical debridement + biofilm-active antibiotics while retaining stable implant.
Indications (ALL must be met):
- Timing: Early postoperative (under 4 weeks) OR acute hematogenous with symptom duration under 3 weeks
- Implant stability: Well-fixed components, no loosening
- Tissue quality: Intact polyethylene, no gross contamination, viable soft tissue
- Organism: Susceptible to biofilm-penetrating antibiotics (avoid MRSA, fungi, resistant GNR)
- Host: Immunocompetent, low KLIC score (under 3)
The KLIC score (Tornero et al, Clin Microbiol Infect 2015) is a validated preoperative predictor of early DAIR failure. The acronym stands for:
- K: Kidney - chronic renal failure
- L: Liver - cirrhosis
- I: Index surgery - revision arthroplasty or surgery for femoral neck fracture (vs primary)
- C: Cemented prosthesis
- plus elevated CRP (over 11.5 mg/dL), the strongest single weight
Outcomes (total score 0-9.5):
- Score 2 or less: 4.5% failure
- Score 4-5: 55% failure
- Score 7 or greater: 100% failure
Application: A high KLIC score is a relative contraindication to DAIR - consider two-stage even with early presentation. Beware the common exam trap of mis-expanding KLIC as "immunosuppression/chronicity"; immunosuppression and chronic symptoms are separate, real risk factors but are not the letters of the KLIC acronym.
DAIR Surgical Steps
Radical synovectomy:
- Remove ALL synovium (anterior, posterior, medial, lateral compartments)
- Debride interface membrane around components
- Remove cement if gross contamination visible
- Excise any devitalized tissue or hematoma
Polyethylene exchange:
- Mandatory exchange of modular polyethylene insert
- New insert from sterile tray (not re-sterilized used insert)
- Consider exchange of femoral component if modular cemented (controversial)
Volume: Minimum 6-9 liters normal saline pulsed lavage
Technique:
- Pulsed lavage to mechanically disrupt biofilm
- Avoid high-pressure jet (drives bacteria into bone)
- Change gloves, instruments after debridement before irrigation
No chlorhexidine, betadine, or antibiotic solutions (cytotoxic to tissue, no proven benefit).
Closure:
- Layered closure (capsule, subcutaneous, skin)
- No dead space
Drain:
- Consider closed suction drain for 24-48 hours
- Some evidence: Prolonged drainage (over 7 days) increases reinfection risk - remove early
Empiric (until cultures result):
- Vancomycin 15-20 mg/kg IV q12h (target trough 15-20 μg/mL)
- PLUS meropenem 1g IV q8h OR ceftazidime 2g IV q8h
Organism-specific (adjust based on culture):
- MSSA: Flucloxacillin 2g IV q6h + rifampicin 300-450mg PO q12h
- MRSA: Vancomycin (as above) + rifampicin
- Streptococcus: Penicillin G 3 million units IV q4h OR ceftriaxone 2g IV q24h
- GNR: Fluoroquinolone (ciprofloxacin 750mg PO q12h) + rifampicin (if E. coli, not Pseudomonas)
Duration:
- IV antibiotics: 2-6 weeks (debate ongoing - some centers 2 weeks, others 6 weeks)
- Oral suppression: 3-6 months with biofilm-active agent (rifampicin-based combinations)
Rifampicin importance: Penetrates biofilm, active against stationary-phase bacteria. NEVER use as monotherapy (resistance develops rapidly). Always combine with flucloxacillin, vancomycin, or fluoroquinolone.
ALWAYS exchange modular polyethylene during DAIR. Studies show 50% reduction in failure rate with insert exchange. The biofilm on polyethylene cannot be adequately debrided, and bacteria within the polyethylene matrix (absorbed during sterilization and implantation) serve as a reservoir for reinfection. This is non-negotiable even if insert appears pristine. Examiners may ask: "The insert looks perfect - do you still exchange it?" Answer: "Yes, absolutely. Biofilm on polyethylene is invisible and impossible to eradicate with debridement alone. Exchange is mandatory for any chance of DAIR success."
Success Rates:
- Early infection (under 4 weeks): 50-70%
- Acute hematogenous (under 3 weeks symptoms): 60-75%
- S. aureus: 45-60% (lower than Strep)
- Streptococcus: 70-85% (best prognosis)
- GNR/Polymicrobial: 30-50% (poor prognosis)
DAIR is a single-stage retention strategy but has lower success than 2-stage revision.
Complications of PJI Treatment
Complications by Treatment Modality
- Incidence
- 30-50% overall
- Risk Factors
- KLIC score over 2, MRSA, symptom duration over 3 weeks, biofilm maturity
- Management
- Proceed to 2-stage revision. Early recognition (CRP not declining by 2 weeks) allows earlier conversion
- Incidence
- 10-25%
- Risk Factors
- Static spacer (higher), non-weight-bearing non-compliance, osteoporotic bone
- Management
- Spacer revision if early (first 4 weeks). If near Stage 2 timing, proceed to reimplantation
- Incidence
- 15-30%
- Risk Factors
- Static spacer, prolonged interval (over 12 weeks), poor nutrition, osteoporosis
- Management
- Requires stems, augments, or allograft at Stage 2. May necessitate more constrained implant
- Incidence
- 10-15%
- Risk Factors
- Immunosuppression, resistant organism, inadequate debridement, early reimplantation (under 6 weeks)
- Management
- Half are recurrence (same organism) - repeat 2-stage. Half are new organism - treat as primary PJI
- Incidence
- 5-15% after 2-stage
- Risk Factors
- Multiple surgeries, poor soft tissue quality, constrained implant, aggressive debridement
- Management
- Immobilization 6 weeks, aggressive quadriceps rehab. If complete disruption, may require allograft reconstruction or chronic brace
- Incidence
- 20-40% after 2-stage
- Risk Factors
- Prolonged immobilization (static spacer), multiple surgeries, patient factors (diabetes, smoking)
- Management
- Manipulation under anesthesia at 6-12 weeks. Arthroscopic lysis of adhesions if manipulation fails. Accept limited ROM in exchange for infection control
- Incidence
- 15-25%
- Risk Factors
- Neuropathic pain from nerve injury, bone loss, soft tissue scarring, constrained implant
- Management
- Multimodal pain management. Rule out recurrent infection (aspiration). Gabapentin for neuropathic component. Salvage if intractable
- Incidence
- 3-7%
- Risk Factors
- Prolonged broad-spectrum antibiotics (over 6 weeks), older age, prior CDI, fluoroquinolone use
- Management
- Discontinue inciting antibiotic if possible. Vancomycin PO or fidaxomicin for CDI treatment. Consider fecal microbiota transplant if recurrent
Examiners often ask: "Patient has recurrent PJI after 2 failed 2-stage revisions. What next?"
Answer: "This is a difficult scenario requiring shared decision-making. I would have an honest conversation about the three options: (1) Third attempt 2-stage revision - success rate drops to 60-70% after second failure, but preserves potential for functional knee. (2) Resection arthroplasty - infection control 90%, but poor function requiring brace and crutches lifelong. (3) Chronic suppressive antibiotics - temporizing if organism is low-virulence and sensitive, but not curative. If young active patient with good bone stock, I would consider one more attempt at 2-stage with extended antibiotic holiday (12 weeks) and aggressive debridement. If elderly low-demand or immunosuppressed, resection or suppression may be more realistic. If life-threatening sepsis uncontrolled, amputation is last resort. The key is tempering expectations - recurrent PJI often means accepting functional compromise to achieve infection control."
Surgical Technique
The surgical management of PJI involves either DAIR (retention strategy) or 2-stage revision (explantation strategy). Detailed technique is critical for exam viva scenarios.
Debridement, Antibiotics, Implant Retention (DAIR)
Positioning: Supine, tourniquet applied but NOT inflated during debridement (allow bleeding to flush bacteria).
DAIR Procedure
Approach: Use prior incision, excise wound edges if contaminated.
Arthrotomy: Standard medial parapatellar approach, evert patella.
Initial assessment: Assess polyethylene condition, implant stability (varus/valgus stress, AP drawer).
Remove ALL synovium:
- Anterior compartment (suprapatellar pouch)
- Medial and lateral gutters
- Posterior compartments (difficult access - use curved curettes)
- Intercondylar notch
Interface debridement:
- Curette bone-implant interface (femoral component undersurface, tibial baseplate undersurface)
- Remove interface membrane and granulation tissue
- If gross purulence or cement contamination, consider cement removal (convert to 2-stage)
Technique: Aggressive synovectomy is KEY. Incomplete removal leaves biofilm reservoir leading to DAIR failure.
Remove modular insert:
- Unlock mechanism (varies by implant system)
- Remove polyethylene insert completely
- Inspect tibial baseplate and femoral component for damage
Insert new polyethylene:
- From STERILE UNOPENED tray (NOT re-sterilized used insert)
- Same thickness or adjust for soft tissue tension
- Lock securely into tibial baseplate
Rationale: Biofilm on polyethylene cannot be debrided. Bacteria absorbed into polyethylene matrix serve as infection reservoir. Exchange is MANDATORY - reduces failure rate 50%.
Volume: 9-12 liters normal saline pulsed lavage (minimum 6 liters).
Technique:
- Pulsed lavage with moderate pressure (NOT high-pressure jet - drives bacteria into bone)
- Change gloves, instruments, gown AFTER debridement BEFORE irrigation (avoid recontamination)
- No additives: Do NOT use chlorhexidine, betadine, or antibiotic solutions (cytotoxic to cartilage and tissue)
Goal: Mechanical biofilm disruption and bacterial washout.
Layered closure:
- Capsule (absorbable suture, watertight)
- Subcutaneous (eliminate dead space)
- Skin (absorbable subcuticular OR staples)
Drain: Closed suction drain for 24-48 hours (remove when output under 30mL/8h).
Dressing: Occlusive dressing for 48 hours minimum.
Postoperative antibiotics: IV organism-specific 2-6 weeks, then oral suppression 3-6 months (rifampicin-based combinations).
Success factors: Early timing (under 4 weeks), sensitive organism, complete synovectomy, polyethylene exchange.
Indications to ABORT Stage 2 and place new spacer:
- Positive intraoperative cultures (same organism or new organism)
- Frozen section over 5 PMN/hpf (suggests persistent infection)
- Gross purulence encountered during spacer removal
- Uncontrolled soft tissue infection (cellulitis, drainage)
Do NOT proceed with reimplantation if infection suspected - reinfection rate approaches 50-70% if reimplanted in presence of infection. Better to extend interval and place new spacer. Patient will be disappointed, but this is the safest approach.
Postoperative Care and Rehabilitation
Postoperative management differs significantly between DAIR and 2-stage revision, and between Stage 1 and Stage 2 of the 2-stage protocol.
DAIR Rehabilitation
DAIR Recovery Timeline
Antibiotics: Continue empiric IV antibiotics (vancomycin + meropenem OR ceftazidime) until cultures result, then switch to organism-specific.
Drain management: Remove closed suction drain at 24-48h when output under 30mL/8h.
Wound care: Occlusive dressing intact for 48h minimum. Inspect at 48h for erythema, drainage.
Mobilization: Day 0 or Day 1 - sit to stand, ambulation with walker. Full weight-bearing as tolerated (implant retained, stable).
ROM: Start passive ROM exercises Day 1 (CPM OR physiotherapy). Goal: Maintain preoperative ROM.
DVT prophylaxis: Aspirin 100mg daily OR rivaroxaban 10mg daily for 14 days. Mechanical prophylaxis (TED stockings, foot pumps).
Antibiotics:
- IV organism-specific for 2-6 weeks (debate: some centres 2 weeks, others 6 weeks)
- Common regimens: (MSSA) Flucloxacillin 2g IV q6h + rifampicin 450mg PO q12h. (Strep) Penicillin G 3M units IV q4h OR ceftriaxone 2g IV q24h.
- Outpatient parenteral antibiotic therapy (OPAT): PICC line, home IV administration OR daily infusion clinic visits
Clinical monitoring:
- CRP weekly (should decline by 50% at 2 weeks post-DAIR - if not, DAIR failing)
- Wound inspection weekly (no persistent drainage)
- Pain and function assessment
Physiotherapy: Progressive ROM and strengthening. Goal: 0-110 degrees by 6 weeks.
Weight-bearing: Full weight-bearing, progress from walker to cane to independent.
Transition to oral:
- After 2-6 weeks IV, switch to oral suppression for 3-6 months
- Biofilm-active agents: Rifampicin combinations (NEVER rifampicin monotherapy - resistance develops in days)
- (MSSA) Rifampicin 450mg PO q12h + flucloxacillin 1g PO q6h
- (Strep) Amoxicillin 1g PO q8h (rifampicin not required)
- (GNR E. coli) Ciprofloxacin 750mg PO q12h + rifampicin 450mg PO q12h
Monitoring: CRP monthly, clinical assessment monthly. Rising CRP = DAIR failure, consider 2-stage.
Function: Return to activities of daily living by 3 months. Avoid high-impact sports lifelong.
Follow-up: 3 months, 6 months, 12 months, then yearly.
Assessment: Pain, function, ROM, stability. CRP annually.
Radiographs: Yearly to assess for loosening or progressive lucency (late failure).
Education: Prompt reporting of acute pain, swelling, fever (acute hematogenous infection risk lifelong).
DAIR success indicators: CRP declining by 50% at 2 weeks, symptom resolution by 4-6 weeks, stable ROM. Failure indicators: Persistent pain, rising CRP, recurrent effusion → proceed to 2-stage.
Outcomes and Prognosis
Outcomes differ significantly by treatment modality and patient factors. Understanding prognosis is essential for counseling and shared decision-making.
DAIR Outcomes
- Success Rate
- 60-70%
- Failure Predictors
- Symptom duration over 3 weeks reduces success to 30-40%
- Success Rate
- 60-75%
- Failure Predictors
- Over 3 weeks symptom duration drops success to 30%
- Success Rate
- 70-85%
- Failure Predictors
- Best prognosis if early and sensitive
- Success Rate
- 45-60%
- Failure Predictors
- More virulent than Strep, forms biofilm faster
- Success Rate
- 20-40%
- Failure Predictors
- DAIR contraindicated - proceed to 2-stage
- Success Rate
- 60-70%
- Failure Predictors
- Low KLIC score predicts success
- Success Rate
- Under 20%
- Failure Predictors
- High KLIC score predicts failure - avoid DAIR
DAIR failure timeline: Most failures occur within 6 months (80%). Late failures (over 2 years) rare. Early recognition of failure (CRP not declining, persistent symptoms) allows timely conversion to 2-stage.
2-Stage Revision Outcomes
Success rate: 85-90% infection eradication at 5 years (most reliable treatment for PJI).
Reinfection: 10-15% develop recurrent or new infection:
- Half are recurrence (same organism - inadequate debridement or persistent biofilm)
- Half are new organism (new contamination, immunocompromised host)
Salvage after failed 2-stage: Second 2-stage attempt (60-70% success), resection arthroplasty, suppressive antibiotics, amputation (last resort).
Knee Society Score: 70-80 (vs 90+ for uncomplicated primary TKA).
ROM: Average 90-100 degrees (vs 120 for primary). Limited by arthrofibrosis and multiple surgeries.
Pain relief: 70-80% achieve satisfactory pain relief. 20-30% have residual pain (neuropathic, bone loss, soft tissue damage).
Return to activities: Low-impact only (walking, swimming, cycling). High-impact sports contraindicated lifelong.
Patient satisfaction: 70-75% satisfied (vs 85-90% for primary TKA). Lower expectations due to prolonged treatment.
1-year mortality: 7% (higher than hip fracture at 4%). Elderly immunosuppressed patients highest risk.
Complications: 20-30% experience major complication (extensor lag, stiffness, instability, recurrent infection).
Reoperations: 25-35% require further surgery within 5 years (infection, instability, aseptic loosening, manipulation for stiffness).
Economic burden: Average total cost $100,000-150,000 AUD (two surgeries, prolonged antibiotics, complications).
Recovery timeline: 6-12 months total (vs 3-6 months for primary TKA).
Disability duration: Average 9 months unable to work or perform ADLs.
Psychological impact: Depression common (30-40%) due to prolonged treatment, uncertainty, functional limitations.
Social impact: Relationship strain, financial burden (lost wages, medical costs), activity restrictions.
Patient education critical: Realistic expectations, prolonged recovery, functional compromise, lifelong surveillance.
Prognostic Factors for Reinfection After 2-Stage
- Reinfection Risk
- 20-30% reinfection
- Management Strategy
- Extended interval (12+ weeks), targeted antibiotics, consider chronic suppression
- Reinfection Risk
- 20-35% reinfection
- Management Strategy
- Medical optimization, extended antibiotics, lower threshold for salvage
- Reinfection Risk
- 25-40% reinfection
- Management Strategy
- Meticulous Stage 1 technique, remove ALL foreign material
- Reinfection Risk
- 30-50% reinfection
- Management Strategy
- Wait for CRP under 10, clinical resolution before Stage 2
- Reinfection Risk
- 25-35% reinfection
- Management Strategy
- Gastrocnemius flap, plastic surgery involvement, wound VAC if needed
Viva question: "How do you counsel a patient about expected outcomes after 2-stage revision for PJI?"
Answer: "I have an honest conversation about the three key outcomes: (1) Infection control: 85-90% chance we eradicate infection, but 10-15% risk of reinfection requiring further treatment, possibly salvage procedures. (2) Function: Your knee will NOT return to normal. Average range of motion is 90-100 degrees (unable to fully kneel). Knee scores average 70-80 vs 90+ for uncomplicated TKA. You'll be able to walk, swim, cycle - but no high-impact sports like running or tennis. (3) Timeline: This is a long journey - two surgeries 6-12 weeks apart, then 6-12 months full recovery. You'll be on antibiotics for months, multiple hospital admissions, physiotherapy for months. Most patients are back to their baseline function by 9-12 months, but some never fully recover. I emphasize that the goal is infection control first, function second. We accept functional compromise to eliminate infection. If infection recurs despite best efforts, we may need salvage procedures like permanent removal of the prosthesis. I document this discussion thoroughly and encourage questions."
Prevention Strategies
Evidence-Based Prevention Bundle
PJI prevention is multifactorial. No single intervention eliminates risk, but bundled strategies reduce incidence by 50-70%.
Preoperative Risk Modification
- Target
- HbA1c under 7.0%
- Evidence
- HbA1c over 7.5% increases PJI risk OR 1.7. Every 1% increase = 30% higher infection
- Implementation
- Postpone elective TKA if HbA1c over 8%. Endocrinology referral. Recheck 3 months
- Target
- BMI under 35 (ideally under 30)
- Evidence
- BMI over 40 increases PJI risk OR 3.0. Every 5-unit BMI increase = 20% higher infection
- Implementation
- Bariatric surgery if BMI over 40. Weight loss program 6-12 months. Counsel realistic expectations
- Target
- Zero tobacco use 8+ weeks before surgery
- Evidence
- Current smoking increases PJI risk OR 2.0. Nicotine impairs wound healing and immune function
- Implementation
- Smoking cessation program. Nicotine replacement therapy. Postpone surgery until 8 weeks smoke-free
- Target
- Albumin over 3.5 g/dL, lymphocyte count over 1500
- Evidence
- Malnutrition doubles PJI risk. Albumin under 3.0 = OR 2.5 for infection
- Implementation
- Nutritionist referral. Protein supplementation (1.5g/kg/day). Delay surgery if albumin under 3.0
- Target
- Nasal swab PCR positive for S. aureus
- Evidence
- Mupirocin nasal ointment + chlorhexidine body wash reduces PJI 50% in carriers
- Implementation
- Screen all patients. Mupirocin 2% intranasal BID 5 days + chlorhexidine 4% wash 5 days before surgery
- Target
- Rheumatoid arthritis, inflammatory arthritis on biologics, steroids
- Evidence
- Biologics increase PJI risk OR 2.0-3.0. Chronic steroids (over 10mg prednisone daily) increase OR 1.5
- Implementation
- Hold biologics: TNF-inhibitors 2-4 weeks, rituximab 6 months. Wean steroids to under 10mg daily if possible. Coordinate with rheumatology
Question: "Should we screen all TKA patients for S. aureus colonization?"
Answer: "Yes, universal screening is cost-effective. 20-30% of population are nasal S. aureus carriers, and carriers have 3-fold higher PJI risk. The decolonization bundle (mupirocin intranasal + chlorhexidine body wash for 5 days before surgery) reduces PJI by 50% in carriers with NNT of 30. This is one of the most effective single interventions for PJI prevention. Australian hospitals increasingly adopt universal screening at pre-admission clinic 2-4 weeks before surgery, allowing time for decolonization protocol."
Preoperative optimization targets modifiable patient risk factors.
STOP-PJIPrevention Bundle Components
Hook:STOP-PJI before it starts - prevention is better than 2-stage revision cure!
Guidelines, Registries & Global Practice
PJI is the leading or second leading indication for revision TKA in virtually every national registry, and its absolute burden is rising worldwide as primary arthroplasty volume grows.
- Reported figure
- PJI 2.0-2.4% of primary THA/TKA; projected cost over $1.62 billion/year by 2020
- Note
- Largest published cost projection; rising incidence over time
- Reported figure
- Infection approximately 25% of all revision TKA; primary TKA infection 1.8% at 5 years
- Note
- Registry surveillance; infection is a leading revision cause
- Reported figure
- Primary TKA PJI roughly 1-2%; revision PJI 3-5%
- Note
- Consistent with international ranges
- Reported figure
- 2.5- to 3-fold higher infection risk than primary
- Note
- Re-operation and host compromise drive excess risk
According to PubMed, the US economic-burden data are from Kurtz et al, J Arthroplasty 2012 DOI. Across high-income registries the primary TKA infection rate clusters around 1-2% and revision around 3-5%, but absolute numbers are climbing everywhere with arthroplasty demand.
Consent requirement: PJI must be discussed when consenting for primary TKA, even though the risk is only about 1-2%, because it is the most serious complication and carries major implications (revision surgery, prolonged recovery, functional compromise). This reflects the international "material risk" standard for informed consent (for example the Rogers v Whitaker principle in Australia and the Montgomery principle in the UK).
Minimum consent elements:
- Infection risk: "1-2%, higher if diabetic, obese or immunosuppressed"
- Treatment: "may require removal of the prosthesis, antibiotics and a second operation to replace it (two-stage revision)"
- Timeline: "treatment can take 6-12 months from diagnosis to full recovery"
- Outcomes: "even with successful treatment function may not return to normal - average flexion 90-100 degrees versus around 120 for an uncomplicated TKA"
- Salvage: "a small risk (5-10%) of repeated failed treatment requiring permanent implant removal"
Document this discussion in the consent form and clinic notes; patients who develop PJI are more likely to litigate if they feel they were not warned.
MCQ Practice Points
Q: A patient undergoing aspiration for suspected PJI has synovial WCC 4000 cells/μL with 75% PMN, CRP 25 mg/L, ESR 40 mm/hr, and alpha-defensin positive. Culture is negative. What is the MSIS score and diagnosis?
A: MSIS score = 8 points (definite PJI). CRP over 10 = 1 point, ESR over 30 = 1 point, synovial WCC over 3000 = 2 points, PMN over 70% counts with WCC (do NOT double-score, so 0 additional points), alpha-defensin positive = 3 points. Total 1+1+2+3 = 7 points. Wait - I made error. PMN over 70% = 1 point separately, so actually 1+1+2+1+3 = 8 points (definite infection, threshold is 6). Proceed with treatment despite negative culture (likely prior antibiotics).
Q: Which scenario is the BEST candidate for DAIR: (A) 6 weeks post-TKA, 2-week history of pain and swelling, MSSA, stable implant. (B) 2 weeks post-TKA, 1-week history of pain, MRSA, stable implant. (C) 3 years post-TKA, acute onset (5 days), Streptococcus, stable implant. (D) 8 weeks post-TKA, insidious onset over 4 weeks, CNS, stable implant.
A: Answer (C). Acute hematogenous PJI (Type III) with symptom duration under 3 weeks, Streptococcus (favorable organism), stable implant. DAIR success 75%. (A) fails because chronic infection (6 weeks post-op with insidious 2-week symptoms suggests smoldering infection over 4 weeks - KLIC C criterion). (B) fails because MRSA is relative contraindication to DAIR (biofilm difficult to eradicate). (D) fails because chronic (8 weeks post-op, insidious onset over 4 weeks) and CNS (low virulence but antibiotic-resistant).
Q: What is the standard antibiotic formulation for a 2-stage revision antibiotic cement spacer?
A: Vancomycin 4-6g + tobramycin 3-4g per 40g cement (Palacos R or equivalent PMMA). Maximum 10% antibiotic by weight to maintain mechanical properties. Vancomycin provides Gram-positive coverage (including MRSA), aminoglycoside provides Gram-negative coverage and synergy. Dual kinetic profile: aminoglycoside elutes rapidly (peak 24-48h), vancomycin elutes slowly (sustained over 6-12 weeks).
Q: A 65-year-old diabetic patient (HbA1c 8.5%) with BMI 42 who smokes 10 cigarettes daily is scheduled for elective TKA in 6 weeks. What preoperative interventions reduce PJI risk?
A: Postpone surgery and optimize: (1) Glycemic control - HbA1c target under 7.0% (ideally 6.5%). HbA1c 8.5% increases PJI risk 70%. Endocrinology referral, consider insulin if needed. Recheck in 3 months. (2) Weight reduction - BMI 42 triples PJI risk. Bariatric surgery referral or intensive weight loss program. Realistic target: Reduce to BMI under 35 over 6-12 months. (3) Smoking cessation - doubles PJI risk. Smoking cessation program, nicotine replacement. Require 8 weeks smoke-free minimum before surgery. (4) S. aureus screening and decolonization - nasal swab PCR, if positive mupirocin 2% intranasal BID + chlorhexidine 4% body wash for 5 days before surgery. This patient is NOT a safe candidate for elective TKA without risk modification. Counsel honestly: Operating now has 6-10% infection risk vs 1-2% if optimized.
Q: What factors determine the interval duration between Stage 1 and Stage 2 of a two-stage revision?
A: Standard interval 6-12 weeks, but varies based on: (1) Organism virulence - MSSA/Strep: 6-8 weeks. MRSA/resistant GNR: 12+ weeks. Fungi: 12-24 weeks. (2) Clinical response - CRP normalization (under 10 mg/L), symptom resolution (no pain, swelling, drainage). If poor response, extend interval. (3) Host factors - Immunosuppressed: Longer interval (12+ weeks). Diabetic with poor control: Optimize first. (4) Spacer function - Articulating spacer well-tolerated: Can wait 12 weeks. Static spacer with pain/bone loss: Consider shorter (6-8 weeks). No evidence that longer interval improves eradication beyond 6 weeks if clinical resolution achieved. Emerging practice: Shorter intervals (2-4 weeks) for virulent organisms with rapid response (requires close monitoring).
Q: A patient has failed two 2-stage revisions for recurrent MRSA PJI. She is 70 years old with diabetes, ESRD on dialysis, and limited mobility (walks with frame indoors only). What are her management options and which would you recommend?
A: Options: (1) Third 2-stage attempt - success rate 60-70% after second failure, but requires good host and aggressive debridement. Her ESRD and diabetes make poor candidate (KLIC score 4 = 100% failure). (2) Resection arthroplasty - removes all hardware, 90% infection control. She would require long leg brace and crutches/walker (already using frame, so functional impact moderate). (3) Chronic suppressive antibiotics - MRSA is difficult to suppress (need vancomycin IV or linezolid PO, both have toxicity). ESRD complicates dosing. Not curative but temporizing. (4) Amputation - last resort, but mortality 10-15% and she may not ambulate with prosthesis given limited baseline mobility. My recommendation: Resection arthroplasty. She is poor candidate for reconstruction (multiple failures, high KLIC score, MRSA). Chronic suppression is risky with ESRD (vancomycin dosing, linezolid bone marrow toxicity). Amputation too aggressive for current presentation. Resection gives 90% infection control, allows mobilization with brace (similar to her current frame), avoids lifelong antibiotics. Counsel: This is permanent - reimplantation rarely successful after resection. Quality of life limited but infection resolved.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old man presents 18 months after primary TKA with 6-week history of progressive knee pain and effusion. No fever. CRP 42 mg/L, ESR 65 mm/hr. Radiographs show 2mm tibial lucency. How do you assess and manage this patient?”
“A 55-year-old woman is 3 weeks post-primary TKA. She develops acute onset knee pain, swelling, erythema over 5 days. Temp 38.2°C, CRP 85, WCC 14. She has well-controlled diabetes (HbA1c 6.8%) and rheumatoid arthritis on methotrexate (held 2 weeks before surgery). Aspiration grows MSSA sensitive to flucloxacillin. Radiographs show well-fixed components. She asks: 'Do I need another surgery or can antibiotics cure this?' How do you proceed?”
“You performed Stage 1 explantation and antibiotic spacer for chronic TKA PJI with CNS (coagulase-negative Staph) 8 weeks ago. Patient returns with acute pain and inability to bear weight. Radiograph shows spacer fracture with displacement. CRP was 8 last week (normalized from 45 at Stage 1), now CRP is 15. Aspiration of spacer grows no organisms. She is scheduled for Stage 2 next week. What do you do?”
MSIS Diagnostic Criteria
- 1 Major (sinus tract OR purulence) = definite PJI
- Score 6+ from minor = definite. 2-5 = possible
- Minor: CRP over 10 (1pt), ESR over 30 (1pt), D-dimer over 860 (2pt)
- Synovial WCC over 3000 (2pt), PMN over 70% (1pt - no double-score with WCC)
- Alpha-defensin positive (3pt) - best single marker 97% sens, 96% spec
- Culture: 2+ same organism (3pt), 1 virulent (2pt)
- Antibiotic holiday: Min 2 weeks off (ideally 6 weeks) before cultures
Classification (Tsukayama)
- Type I: Early (under 4 weeks) = DAIR + antibiotics 6 weeks
- Type II: Late chronic (over 4 weeks) = 2-stage revision
- Type III: Acute hematogenous (acute onset, under 3 weeks symptoms) = DAIR if stable implant
- Type IV: Positive intraop cultures = antibiotics 6 weeks, no removal if stable
DAIR Indications (STEADI)
- S: Symptoms under 3 weeks duration
- T: Timing early (under 4 weeks post-op) OR acute hematogenous any time
- E: Eradicable organism (sensitive, NOT MRSA/fungi)
- A: Articulating surfaces intact (no poly damage)
- D: Definitely stable implant
- I: Immunocompetent (KLIC under 3)
- Success: 50-70% if favorable factors. Polyethylene exchange MANDATORY
2-Stage Revision Protocol
- Stage 1: Remove all components/cement, radical debridement, antibiotic spacer
- Spacer: Vancomycin 4-6g + tobramycin 3-4g per 40g cement
- Interval: 6-12 weeks standard (shorter 2-4 weeks emerging for virulent organisms)
- Criteria for Stage 2: CRP under 10, clinical resolution, no drainage
- Stage 2: Remove spacer, 5+ cultures, revision implants with stems/augments
- Success: 85-90% eradication, but 10-15% reinfection
Prevention Bundle (STOP-PJI)
- S: S. aureus screening + decolonization (mupirocin + chlorhexidine 5 days) - reduces 50%
- T: Timely antibiotics (cefazolin 2g within 60 min of incision)
- O: Optimize comorbidities (HbA1c under 7%, BMI reduction, smoking cessation 8 weeks)
- P: Prepare skin (chlorhexidine-alcohol superior to iodine)
- P: Perioperative normothermia (over 36°C reduces infection 30%)
- J: Joint manipulation gentle (minimize operative time, gentle tissue handling)
- I: Implant antibiotic cement (in high-risk: revision, immunosuppressed)
Key Evidence and Outcomes
- MSIS 2018: 97.7% sensitivity, 99.5% specificity for PJI diagnosis
- KLIC score (Tornero 2015): predicts DAIR failure. K=kidney (renal failure), L=liver cirrhosis, I=index surgery (revision/fracture), C=cemented prosthesis, plus CRP over 11.5 mg/dL. Failure approximately 4.5% (2 or less) to 100% (7 or greater)
- Articulating vs static spacer: Equal infection eradication (89%), articulating better ROM
- 2-stage interval: 2-week vs 8-week equivalent eradication for virulent organisms, no immunosuppression
- AOANJRR 2023: PJI 25% of revision burden, 1.8% primary at 5yr, 4.5% revision at 5yr
Evidence Base and Key Trials
2018 Definition of Periprosthetic Hip and Knee Infection (ICM/MSIS criteria)
- Multi-institutional development cohort (684 PJI defined by major criteria, 820 aseptic) with external validation (222 PJI, 200 aseptic)
- New weighted scoring: serum CRP and D-dimer 2 points each, ESR 1 point; synovial WCC, alpha-defensin and leukocyte esterase 3 points each, PMN over 80% and synovial CRP 2 and 1 point
- Preoperative aggregate score 6 or greater = infected, 2-5 = inconclusive (add intraoperative findings), 3 or less = not infected
- Sensitivity 97.7% versus 79.3% for the 2011 MSIS criteria, with specificity 99.5%
KLIC Score for DAIR Failure Prediction
- Single-centre prospective cohort of 222 early PJIs treated with debridement, antibiotics and implant retention (DAIR); 23.4% early failure
- KLIC preoperative score (Kidney/chronic renal failure, Liver cirrhosis, Index surgery being revision or fracture, Cemented prosthesis, CRP over 11.5 mg/dL) ranges 0-9.5 points
- Failure by stratum: score 2 or less 4.5%, over 2-3.5 19.4%, 4-5 55%, over 5-6.5 71.4%, 7 or greater 100%
- Independent predictors included CRP over 11.5 mg/dL (OR 12.3) and cemented prosthesis (OR 8.7)
Static vs Articulating Spacers for Infected TKA: Systematic Review
- Systematic review of 7 Level-III comparative studies and 32 Level-IV case series of antibiotic spacers for infected TKA
- Reinfection rate similar: 7% articulating versus 12% static (p=0.2)
- Range of motion after reimplantation significantly greater with articulating spacers (101 degrees versus 91 degrees, p=0.0002)
- Functional scores and wound/spacer complication rates similar between the two spacer types
Single-Stage vs Two-Stage Exchange for Chronic Knee PJI
- Systematic review of 32 studies (14 single-stage, 687 patients; 18 two-stage, 1086 patients) for chronic knee PJI
- Average eradication rate 87.1% single-stage versus 84.8% two-stage
- Knee Society Knee Score similar (80.0 single-stage versus 77.8 two-stage)
- Average range of motion 91.4 degrees single-stage versus 97.8 degrees two-stage
S. aureus Screening, Decolonisation and Targeted Prophylaxis Bundle
- Pragmatic multicentre study, 20 US hospitals, cardiac and hip/knee arthroplasty (over 42,000 operations across pre-intervention and intervention periods)
- Bundle: nasal screening, mupirocin plus chlorhexidine for S. aureus carriers, and vancomycin-containing prophylaxis for MRSA carriers
- Complex S. aureus SSI fell from 36 to 21 per 10,000 operations overall (RR 0.58, 95% CI 0.37-0.92)
- For hip/knee arthroplasty specifically, RR 0.48 (95% CI 0.29-0.80)
AOANJRR 2023 Annual Report: PJI Epidemiology in Australia
- PJI accounts for 25% of all revision TKA burden (AOANJRR; second only to aseptic loosening at 30%)
- Primary TKA infection rate: 1.8% at 5 years, 2.2% at 10 years (increasing over time)
- Revision TKA infection rate: 4.5% at 5 years (2.5-fold higher than primary)
- Cemented TKA has lower PJI risk vs uncemented (1.8% vs 2.4% at 5 years, p less than 0.01)
- Obesity (BMI over 35) increases PJI revision rate 2-fold
Economic Burden of PJI in the United States
- Nationwide Inpatient Sample 2001-2009: PJI incidence 2.0-2.4% of total hip and knee arthroplasties, increasing over time
- Annual US hospital cost of infected revisions rose from $320 million to $566 million over the study period
- Projected to exceed $1.62 billion per year by 2020 as arthroplasty volume grows
- Mean cost to treat a hip PJI exceeded knee PJI by approximately $5965
IDSA Clinical Practice Guideline: Diagnosis and Management of PJI
- Comprehensive evidence- and opinion-based guideline from the Infectious Diseases Society of America
- Defines pathways for DAIR (debridement and retention), resection arthroplasty with or without staged reimplantation, one-stage reimplantation and amputation
- Endorses DAIR only for well-fixed implants, short symptom duration and susceptible organisms
- Recommends rifampicin-based combinations for staphylococcal PJI managed with retention
Antibiotic Route and Duration: Landmark RCTs
The route and duration of antibiotics referenced throughout this chapter (the "IV 2-6 weeks", "oral suppression" and post-Stage-2 duration debates) are now informed by two landmark randomised trials. These resolve the PJI-specific decisions raised here; general antibiotic pharmacology and resistance are developed in the orthopaedic-antibiotic-therapy topic.
OVIVA: Oral versus Intravenous Antibiotics for Bone and Joint Infection
- Multicentre randomised noninferiority trial, 1054 adults at 26 UK centres with bone or joint infection (including prosthetic joint infection), randomised within 7 days of surgery to IV versus oral antibiotics for the first 6 weeks
- Definitive treatment failure at 1 year: 14.6% IV versus 13.2% oral
- Risk difference (oral minus IV) -1.4 percentage points (90% CI -4.9 to 2.2), within the 7.5-point noninferiority margin
- Catheter complications more common with IV (9.4% versus 1.0%); serious adverse events similar between groups
DATIPO: Six versus Twelve Weeks of Antibiotic Therapy for Prosthetic Joint Infection
- Open-label randomised noninferiority trial, 410 patients at 28 French centres with microbiologically confirmed PJI managed with appropriate surgery, randomised to 6 versus 12 weeks of antibiotics
- Persistent infection within 2 years: 18.1% (6 weeks) versus 9.4% (12 weeks)
- Risk difference 8.7 percentage points (95% CI 1.8 to 15.6), exceeding the 10-point margin - noninferiority was NOT shown
- No significant between-group difference in new infection, probable failure or serious adverse events
Keep the two questions separate. Route (OVIVA): an early switch to oral antibiotics is noninferior to IV for bone and joint infection when a suitable oral agent and adherence are assured - so prolonged PICC-line IV therapy is not mandatory. Duration (DATIPO): for PJI overall, 6 weeks was inferior to 12 weeks (persistent infection 18.1% vs 9.4%), so do not reflexively shorten the total course - 12 weeks remains the safer default for established PJI, with shorter courses reserved for selected DAIR or single-stage cases.