Flexion Gap | Extension Gap | Constraint | Revision
- Gap imbalance most common cause
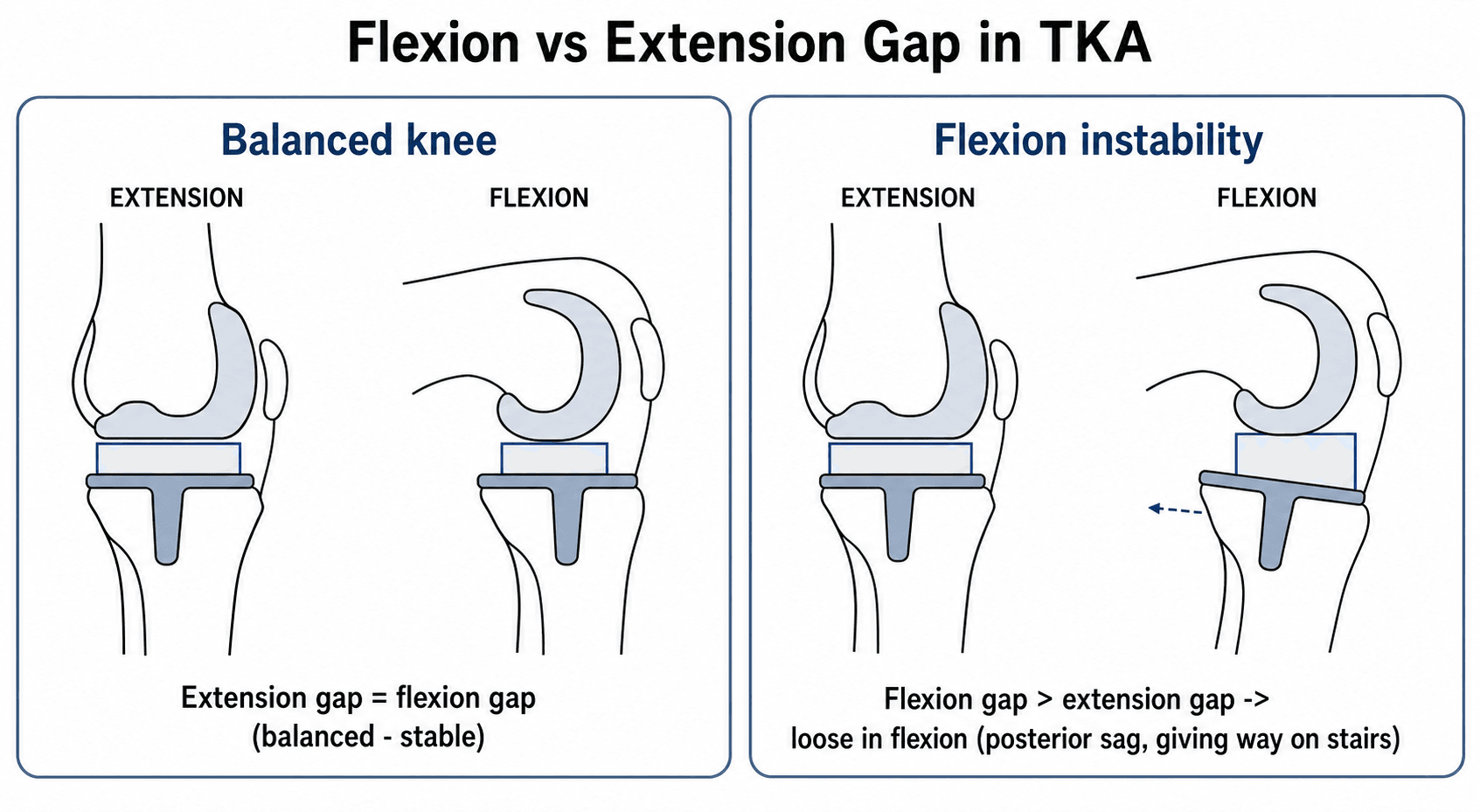
- Flexion instability: loose in flexion
- Extension instability: recurvatum tendency
- Component malposition key factor
- Revision with increased constraint if failed
- “Flexion gap: posterior femoral condyle resection
- “Extension gap: distal femur resection
- “PCL incompetent = flexion instability in CR
- “Increase constraint level for revision
Knee unstable in flexion. Caused by excessive posterior femoral condyle resection, flexion gap too large, PCL incompetence in CR TKA, component malrotation.
Knee unstable in extension. Caused by excessive distal femur resection, extension gap too large, MCL/LCL laxity, recurvatum tendency.
Unstable 30-60 degrees. Femoral component too small or internally rotated. Polyethylene wear. Difficult to address.
Unstable in all positions. Severe ligamentous laxity. Requires higher constraint level (VVC or hinge).
- Key Finding
- Loose in flexion, stairs difficulty
- First-line Treatment
- Thicker polyethylene
- Revision Approach
- PS conversion or downsize femur
- Key Finding
- Recurvatum, loose standing
- First-line Treatment
- Bracing trial
- Revision Approach
- Distal femoral augment
- Key Finding
- 30-60 degree laxity
- First-line Treatment
- PT, bracing
- Revision Approach
- Correct rotation, VVC
- Key Finding
- All positions unstable
- First-line Treatment
- Hinged brace
- Revision Approach
- VVC or rotating hinge
- Cause
- Excessive posterior condyle resection
- Solution
- Downsize femur or use PS
- Cause
- Excessive distal resection
- Solution
- Augment distal femur
- Cause
- Global ligament laxity
- Solution
- Increase constraint level
- Cause
- Under-resection
- Solution
- Additional bone cuts
PCPSFlexion Gap Components
Hook:PCPS determines Posterior (flexion) Gap!
DMCExtension Gap Components
Hook:DMC = Distal femur determines extension gap!
CPVHConstraint Level Selection
Hook:CPVH = Constraint rises from C to H!
Overview and Epidemiology
Most TKA instability results from gap imbalance - mismatch between flexion and extension gaps, or global ligamentous laxity. Component malpositioning is the underlying cause.
Pathophysiology and Mechanisms
Gap Balancing Concepts:
The stability of TKA depends on equal and balanced flexion and extension gaps. Understanding the structures that contribute to each gap is essential for both prevention and treatment of instability.
- Structures removed: Distal femur resection
- Stabilizers: MCL, LCL, posterior capsule
- Assessment: Knee fully extended (0 degrees)
- Gap size: Determined by distal femur cut depth
- Structures removed: Posterior femoral condyle resection
- Stabilizers: PCL (in CR), MCL, LCL
- Assessment: Knee at 90 degrees flexion
- Gap size: Determined by posterior condyle cut and femoral sizing
- Distal femur resection primarily affects extension gap
- Posterior condyle resection primarily affects flexion gap
- Femoral sizing affects flexion gap (larger femur = smaller flexion gap)
- Posterior tibial slope affects flexion gap (more slope = larger flexion gap)
- Collateral ligaments contribute to both gaps
TKA implants provide varying degrees of intrinsic constraint:
- Mechanism
- Relies on intact PCL
- Indications
- Normal ligaments
- Mechanism
- Cam-post replaces PCL
- Indications
- PCL deficiency
- Mechanism
- Taller post, deeper box
- Indications
- Collateral laxity
- Mechanism
- Linked axis
- Indications
- Global instability
Increasing constraint increases stress at fixation interface - use minimum constraint necessary.
Classification and Mechanism
Flexion Gap Too Large
- Excessive posterior condyle resection
- Femoral component too small (anterior referencing)
- PCL rupture/incompetence in CR TKA
- Excessive posterior tibial slope
- Instability/giving way with stairs, sitting
- Knee feels loose in flexion
- Posterior subluxation
Address by reducing flexion gap or increasing constraint.
Bone Defect Classification (AORI)
Revision for instability frequently uncovers metaphyseal bone loss that dictates the reconstruction. The Anderson Orthopaedic Research Institute (AORI) classification grades the defect separately for the femur (F) and tibia (T) and maps directly onto the fixation strategy.
- Defect
- Intact metaphyseal bone; minor contained defect; joint line near normal
- Typical reconstruction
- Cement, morselised graft, small modular augments
- Defect
- Damaged metaphyseal bone of ONE condyle or plateau
- Typical reconstruction
- Modular augments, with or without cement; stem
- Defect
- Damaged metaphyseal bone of BOTH condyles or plateaus
- Typical reconstruction
- Augments plus metaphyseal cones/sleeves; stem
- Defect
- Deficient metaphyseal segment, often with collateral or extensor-mechanism compromise
- Typical reconstruction
- Metaphyseal cones/sleeves, structural allograft, or a hinge
Classify the defect separately for femur and tibia (F1-F3, T1-T3) and let it drive fixation: type 1 takes cement and small augments, type 2 needs augments and often metaphyseal cones or sleeves, and type 3 (segmental loss, frequently with ligament loss) needs cones/sleeves, structural graft or a hinge. Modern revision aims for zonal fixation - secure purchase in at least two of the three zones (epiphysis, metaphysis, diaphysis), the metaphyseal zone being the one that cones and sleeves restore.
Clinical Assessment
- Giving way episodes
- When does instability occur
- Stairs vs walking vs rising
- Pain location and character
- Time from primary surgery
- Previous surgeries
Timing of symptoms helps classify.
- Varus/valgus stress at 0 and 30 degrees
- Anterior/posterior drawer
- Recurvatum assessment
- Compare to contralateral
- ROM assessment
- Gait evaluation
Document degree and position of laxity.
Differential Diagnosis of the Painful, Unstable-Feeling TKA
The patient who reports "giving way" or recurrent effusion does not always have mechanical instability. Distinguishing true ligamentous/gap instability from its mimics is a high-yield exam point and changes management entirely.
- Discriminating Features
- Reproducible laxity on stress; effusion; stairs or recurvatum symptoms
- Key Test
- Stress exam at 0 and 90 deg, stress radiographs
- Pitfall if Missed
- Revising the wrong way (e.g. liner alone) fails
- Discriminating Features
- Rest pain, warmth, persistent effusion, raised CRP/ESR
- Key Test
- Aspiration: synovial WCC and differential, cultures
- Pitfall if Missed
- Missed infection turns a 1-stage into a disaster
- Discriminating Features
- Anterior knee pain, maltracking, instability 30-60 deg
- Key Test
- CT rotational profile (epicondylar axis, tibial tubercle)
- Pitfall if Missed
- Constraint added without correcting rotation re-fails
- Discriminating Features
- Start-up pain, progressive radiolucency/subsidence
- Key Test
- Serial weight-bearing radiographs, bone scan
- Pitfall if Missed
- Mislabelled as instability; loose component missed
- Discriminating Features
- Extension lag, quadriceps weakness, buckling
- Key Test
- Active extension lag, patellar tracking assessment
- Pitfall if Missed
- Quads-avoidance buckling mistaken for laxity
- Discriminating Features
- Late onset (usually over 10 years), effusion, lysis on film
- Key Test
- Radiographs for lysis, insert thickness assessment
- Pitfall if Missed
- Late wear can coexist with secondary laxity
Every painful/effusing TKA must have periprosthetic joint infection (PJI) excluded before it is attributed to mechanical instability. Screen with serum CRP and ESR; if either is raised (or clinical suspicion is high) aspirate the joint. Widely-used 2018 International Consensus Meeting (ICM) thresholds for chronic knee PJI are a synovial-fluid white-cell count above ~3,000 cells/microlitre and polymorphonuclear cells above ~70%, supported by a positive alpha-defensin, raised synovial CRP, and culture. A missed infection turns a planned single-stage revision into a catastrophe.
Investigations
Radiographic Assessment
- Weight-bearing AP
- Lateral
- Skyline
- Component position
- Joint line position
- Polyethylene wear
- Alignment
Stress views may demonstrate laxity.




Management Algorithm
Conservative Trial
- Mild instability
- Poor surgical candidate
- Recent surgery (give time to stabilize)
- Bracing (hinged knee brace)
- Physical therapy (quad strengthening)
- Activity modification
Limited success for true mechanical instability.
Surgical Technique
Implant Constraint Options
- Indication
- Normal knee
- Mechanics
- Relies on PCL
- Indication
- PCL deficient
- Mechanics
- Cam-post mechanism
- Indication
- Collateral laxity
- Mechanics
- Taller post, more constraint
- Indication
- Global instability
- Mechanics
- Linked mechanism
Increase constraint as needed for stability.
Use minimum constraint necessary. Higher constraint transfers more stress to fixation interface, potentially increasing loosening risk. Balance with need for stability.
Joint Line Restoration and Pseudo-Patella Baja
Restoring the native joint line is one of the most important and most often-missed goals of revision, because elevating the joint line causes mid-flexion instability and a low-riding patella.
- About 1 cm proximal to the fibular head.
- About 1.5 cm distal to the medial epicondyle and about 2.5 cm distal to the lateral epicondyle.
- About 3 cm distal to the adductor tubercle.
- The meniscal scar and the inferior pole of the patella also help.
- Raising the joint line (for example by over-resecting the distal femur, or over-stuffing the tibia to fill a gap) shifts the flexion-extension kinematics and is a recognised cause of mid-flexion instability.
- It also produces pseudo-patella baja: the patellar tendon length is unchanged, but because the joint line has moved proximally the patella now sits low relative to the new joint line, causing anterior knee pain, reduced flexion and extensor dysfunction. This is distinct from true patella baja (a genuinely shortened or scarred patellar tendon).
Aim to restore the joint line to within about 5 to 8 mm of native using the epicondylar and fibular-head landmarks. Suspect pseudo-patella baja when the patella looks low after a revision: the Insall-Salvati ratio is normal (the tendon is unchanged) but a joint-line-referenced index (Blackburne-Peel or the modified Insall-Salvati) is abnormal - the give-away that the joint line, not the tendon, has shifted. Joint-line elevation and patella baja both correlate with worse function, so re-establish the joint line rather than just chasing the gaps.
Complications
- Incidence
- 5-10%
- Prevention/Management
- Appropriate constraint, good balance
- Incidence
- Variable
- Prevention/Management
- Aggressive early ROM
- Incidence
- Increased with constraint
- Prevention/Management
- Adequate fixation, stems
- Incidence
- 2-3% revision
- Prevention/Management
- Prophylaxis, staged if indicated
Complication Prevention Strategies
- Confirm gap balance before final cementation
- Assess stability through full ROM under anesthesia
- Document constraint level selection rationale
- Use adequate stem fixation for constrained implants
- Consider staged approach if any infection concern
- Regular clinical and radiographic follow-up
- Early identification of recurrent symptoms
- Low threshold for aspiration if effusion recurs
- Long-term outcomes depend on initial balance
Postoperative Care
Revision TKA Rehabilitation
Weight-bearing as tolerated. Brace if needed. ROM exercises.
Progressive strengthening. ROM focus. Stairs training.
Full activities. Quad and hamstring focus. Balance training.
Return to normal activities. Long-term follow-up.
Outcomes and Prognosis
Prognostic Factors
Correct diagnosis, appropriate constraint, good bone stock.
Global instability, multiple prior surgeries, poor soft tissues.
Guidelines, Registries & Global Practice
Global epidemiology of TKA instability:
Instability is consistently reported as the second most common indication for TKA revision after aseptic loosening, accounting for roughly 15-20% of all revision TKAs across multi-centre and registry datasets. It is disproportionately an early failure: more than a third of all revisions occur within 2 years of the index procedure, and around half of these early revisions are attributable to instability, malposition or fixation failure - all surgeon-dependent technical factors.
National joint registry signals (cross-registry consensus):
- Region
- UK
- Instability-related observation
- Instability among leading non-infective revision indications; constraint escalation common at revision
- Region
- USA
- Instability-related observation
- Instability a top-three revision cause; documents rising use of constrained and hinge designs at revision
- Region
- Australia/New Zealand
- Instability-related observation
- Instability a major revision indication; younger age at revision associated with higher re-revision risk
- Region
- Sweden
- Instability-related observation
- Long-term survivorship data; emphasises balanced gaps and alignment to reduce revision
- Region
- New Zealand
- Instability-related observation
- Captures constraint level and re-revision; corroborates higher re-revision in younger patients
Registries agree on three points: instability is largely preventable at the index operation, adequate constraint at revision reduces re-revision for instability, and younger patients carry a higher re-revision risk.
Side-by-side guidance from major societies:
- Region
- USA
- Position relevant to TKA instability
- Evidence-based work-up of the painful TKA; rule out infection before attributing symptoms to instability; CT for suspected malrotation
- Region
- UK
- Position relevant to TKA instability
- Revision arthroplasty should be undertaken in networks with appropriate expertise and implant availability (constraint ladder, stems, augments)
- Region
- Global
- Position relevant to TKA instability
- Stepwise constraint principle - use the minimum constraint that restores stability; protect fixation with stems
- Region
- Europe
- Position relevant to TKA instability
- Systematic diagnostic algorithm for the unstable TKA; gap balancing and component re-positioning before defaulting to high constraint
Every society places exclusion of periprosthetic joint infection (serum CRP/ESR, aspiration with synovial WBC and differential) ahead of attributing a painful, effusing TKA to mechanical instability.
- Well-resourced settings: ready access to CT rotational profiling, the full constraint ladder (PS, CCK/VVC, rotating hinge), metaphyseal cones/sleeves and modular augments, and revision arthroplasty networks.
- Limited-resource settings: CT and the higher-constraint/hinge inventory may be scarce; greater reliance on clinical examination and stress radiographs, prolonged bracing trials, and primary-implant-based solutions. The biomechanical principles (balance the gaps, correct rotation, use the least constraint that works) are universal even where the implant menu is narrower.
- Instability as the second leading cause of revision and its early, technique-related nature
- The constraint ladder (CR to PS to CCK/VVC to rotating hinge) and the "minimum constraint" principle
- Why a CR knee with an incompetent PCL becomes flexion-unstable and is converted to PS
- Interpretation of CT rotational studies (epicondylar axis, tibial tubercle)
- Mandatory exclusion of infection before revising for presumed instability
Controversies and Areas of Uncertainty
There is no agreed quantitative threshold for diagnosing flexion instability. Testing positions and laxity grades vary between surgeons, and revision for flexion instability shows the least improvement of any failure etiology - partly because the diagnosis is imprecise. Mechanical symptoms, recurrent effusion and posterior sag remain the practical triad.
Isolated polyethylene liner exchange is attractive (shorter stay, fewer complications) but carries a higher re-revision rate for instability than full component revision. The debate centres on patient selection: well-fixed, well-positioned, correctly rotated components are the only reasonable candidates.
Whether gap-balancing or measured-resection technique better prevents instability remains unsettled; large series report acceptable results with both. Surgeon familiarity and accurate rotational referencing likely matter more than the philosophy chosen.
Higher constraint restores stability but transfers load to the fixation interface and the stems. The "minimum necessary constraint" principle is widely endorsed, yet the exact threshold for stepping from CCK/VVC to a rotating hinge in borderline collateral incompetence is judgement-based, not evidence-defined.
MCQ Practice Points
Q: What does resecting more posterior femoral condyle do? A: Increases the flexion gap. Posterior condyle resection primarily affects flexion gap.
Q: What does resecting more distal femur do? A: Increases the extension gap. Distal femur resection primarily affects extension gap.
Q: What happens if PCL is incompetent in CR TKA? A: Flexion instability. PCL is primary flexion restraint. Need to revise to PS.
Q: What constraint level for moderate collateral laxity? A: VVC (varus-valgus constrained). Taller post provides more coronal stability.
Q: What does internal rotation of femoral component cause? A: Mid-flexion instability. The tibia externally rotates relative to internally rotated femur.
Q: Why use stems with constrained TKA revision? A: To bypass stress transfer to metaphysis. Higher constraint increases fixation stress.
Clinical Imaging
Imaging Atlas
Radiographic assessment of the painful or unstable total knee replacement combines an AP and lateral of the prosthesis with full-length standing alignment films; component position and limb alignment are central to diagnosing instability, malalignment and loosening.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A patient 6 months after primary CR TKA reports instability going downstairs and difficulty rising from a chair. Examination shows increased anterior-posterior translation in flexion but stable in extension. X-rays show well-fixed components. What is your diagnosis and management?”
“A 70-year-old woman with severe RA has had 2 previous TKA revisions. She now has gross instability in all positions and cannot walk without aids. What are your options?”
“A 62-year-old man, 18 months after a primary PS TKA, complains of anterior knee pain, a feeling of the knee 'shifting', and recurrent effusions. He is stable on varus/valgus stress at full extension and reasonably stable at 90 degrees, but feels unstable in the mid-arc. Radiographs show well-fixed components and a slightly laterally tracking patella. How do you work this up and manage him?”
Types
- Flexion: loose in flexion, stairs/sitting
- Extension: recurvatum, loose standing
- Mid-flexion: 30-60 degree laxity
- Global: all positions unstable
Gap Balancing
- Posterior condyle = flexion gap
- Distal femur = extension gap
- Equal gaps for stability
- Flexion gap tight = limited bend
- Extension gap tight = flex contracture
Causes
- Gap imbalance most common
- Component malposition
- PCL incompetence (CR)
- Ligament laxity
Constraint Levels
- CR: relies on PCL
- PS: cam-post for PCL deficiency
- VVC: collateral laxity
- Hinge: global instability
Treatment Principles
- Minimum constraint needed
- Balance gaps at revision
- Address malposition
- Use stems in revision
Outcomes
- 80-85% good after revision
- Re-revision 5-10%
- Match constraint to laxity
- Early instability: technical error likely
- Late instability: polyethylene wear/laxity
Evidence Base and Key Studies
Instability as a Leading Cause of TKA Failure (Insall Award)
- 212 revision TKAs reviewed; instability was a leading failure mode after polyethylene wear and aseptic loosening
- More than half of revisions occurred under 2 years from the index operation
- 50% of early revisions were due to instability, malalignment/malposition or failure of fixation
- Early failure mechanisms are predominantly technique-related
Etiology of Modern TKA Revision (Multicentre)
- Six-centre review: aseptic loosening 31.2% and instability 18.7% were the two leading revision causes
- Instability was the second most common indication overall
- 35.3% of revisions occurred under 2 years and 60.2% within 5 years of index surgery
- Polyethylene wear was uncommon before 15 years; early failure is surgeon-dependent
Across the failure-etiology literature instability is consistently a leading indication for TKA revision - the second commonest after aseptic loosening in contemporary multicentre data (Schroer 2013, 18.7%) and a top-three cause historically (Sharkey 2002, after polyethylene wear and aseptic loosening) - and most early instability is technical. Revision strategy follows a constraint ladder: re-balance and convert CR to PS for flexion instability (Pagnano 1998), constrained condylar for collateral laxity (Mancino 2020), and rotating hinge as salvage for global instability (Kouk 2017).