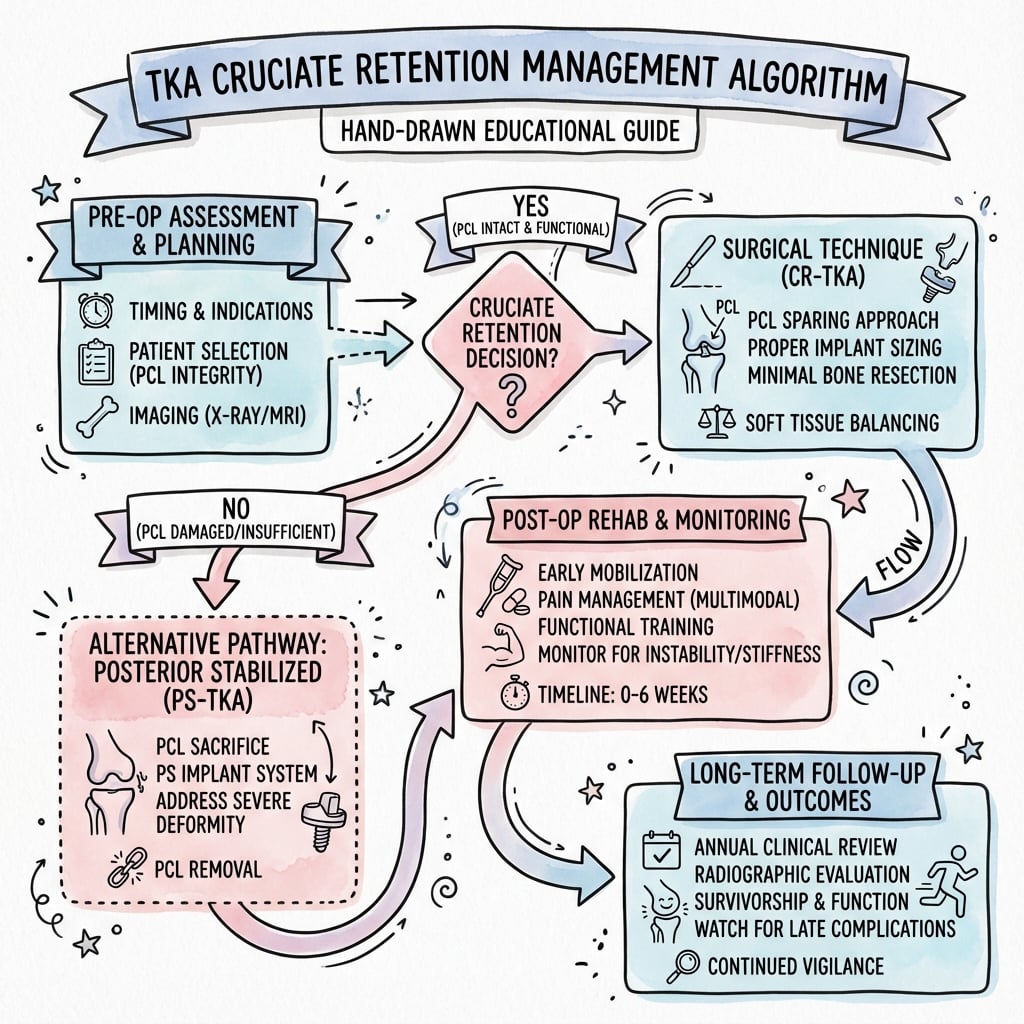
CR vs PS Design | Biomechanical Differences | Evidence-Based Selection
- CR preserves PCL for normal kinematics; PS sacrifices PCL and uses cam-post mechanism
- No clinically significant difference in survivorship or functional outcomes at 10+ years
- PS preferred for PCL deficiency, severe deformity (greater than 15 degrees varus/valgus), or inflammatory arthropathy
- CR requires intact, functional PCL and normal bone stock
- Cam-post impingement and polyethylene wear are PS-specific complications
- “PCL balancing in CR requires careful soft tissue releases to avoid flexion instability
- “PS cam-post engages at 60-70 degrees flexion, providing posterior femoral rollback
- “National joint registries show equivalent revision rates for CR vs PS at 10 years
- “Higher flexion range possible with PS due to cam-post mechanism (130-140 degrees vs 120-130 degrees)
PCL function in normal knee: Prevents posterior tibial translation and guides femoral rollback during flexion. In CR designs, preserved PCL must be balanced to neutral tension. In PS designs, cam-post mechanism substitutes this function from 60-70 degrees flexion onward.
Choose PS for: PCL deficiency, severe deformity (greater than 15 degrees), inflammatory arthritis, revision TKA. Choose CR for: Normal PCL, mild-moderate OA, desire to preserve bone stock. Both achieve excellent long-term outcomes.
CR complications: PCL imbalance causing flexion instability, PCL avulsion. PS complications: Patellar clunk syndrome, cam-post wear and dissociation, posterior femoral bone loss from box cut, anterior tibial post fracture.
Femoral rollback: CR relies on PCL tension (variable, 10-15 degrees). PS uses cam-post contact (consistent, 15-20 degrees). Clinical impact: Greater flexion potential with PS (130-140 degrees vs 120-130 degrees), but no functional difference in daily activities.
- PCL Status
- Intact, functional PCL
- First Choice
- CR or PS (surgeon preference)
- Key Rationale
- Equivalent outcomes, CR preserves bone stock
- PCL Status
- PCL may be contracted or attenuated
- First Choice
- PS (posterior stabilized)
- Key Rationale
- Easier balancing, predictable kinematics
- PCL Status
- PCL often attenuated or dysfunctional
- First Choice
- PS (posterior stabilized)
- Key Rationale
- Avoid reliance on diseased soft tissues
- PCL Status
- PCL absent or insufficient
- First Choice
- PS or CCK (constrained condylar)
- Key Rationale
- Cannot rely on absent PCL, need mechanical stability
Overview and Design Philosophy
The cruciate retention vs substitution debate has evolved over 40+ years. Early TKAs sacrificed both ACL and PCL, leading to instability. CR designs emerged in the 1980s to preserve "normal" kinematics. PS designs followed to address PCL balancing difficulties and deformity correction challenges. Modern evidence shows equivalent long-term survivorship and patient-reported outcomes, making the choice primarily surgeon preference and patient-specific factors.
Fundamental Design Principles
Goal: Preserve native PCL to maintain normal knee kinematics.
Design features:
- Flat or slightly conforming tibial bearing
- No femoral box cut (preserves bone stock)
- Smaller intercondylar notch clearance
- Relies on PCL for posterior stability
Biomechanical reliance: PCL must guide femoral rollback and prevent posterior tibial translation. If PCL is tight, flexion instability occurs. If too loose, posterior translation and wear increase.
Goal: Mechanically substitute PCL function with cam-post articulation.
Design features:
- Central tibial polyethylene post
- Femoral box cut with cam surface
- Higher conformity tibial bearing
- Cam-post engages at 60-70 degrees flexion
Biomechanical independence: No reliance on PCL quality. Cam-post provides predictable femoral rollback (15-20 degrees) and prevents posterior tibial subluxation. Greater constraint allows management of severe deformity.
The Third Option: Condylar-Stabilized / Ultracongruent Design
The OnePager classification and cheat sheet both list CS (condylar-stabilized) as one of the three design philosophies alongside CR and PS - but the body only ever develops CR and PS. CS is the middle path in the cruciate debate and deserves proper treatment (the broader implant taxonomy is covered in the tka-implant-design topic; this is the cruciate-strategy angle).
- What it is. A condylar-stabilized (CS), also called ultracongruent (UC), deep-dish or anterior-stabilized (AS), insert is a polyethylene bearing with a raised anterior lip and a highly conforming, deep-dished articular surface, used on a standard CR femoral component with no box and no post. It provides antero-posterior stability through articular conformity rather than a mechanical cam-post.
- Where it sits between CR and PS. The PCL is usually sacrificed or already deficient, and the deep dish/anterior build-up resists anterior femoral translation (paradoxical slide) and provides posterior restraint - a "PCL substitute without a post". It is the option for the surgeon who wants to sacrifice the PCL for easier balancing but avoid a box cut.
- Advantages. No femoral box cut (preserves posterior femoral bone and avoids box-related fracture) and no post (avoids patellar clunk, post fracture/dissociation and post wear). It is typically interchangeable with the CR femur, so CR-versus-UC can be decided at trialling.
- Trade-offs. Stability depends on good flexion-extension gap balance and conformity, not a hard mechanical stop; there is no guaranteed cam-post rollback (femoral rollback relies on geometry and soft tissues), the high conformity transmits more constraint to the fixation interface (a theoretical loosening concern), and a grossly unbalanced flexion gap can still allow the femur to "jump" the anterior lip (spin-out/dislocation) because there is no post to capture it.
Q: What is a condylar-stabilized (ultracongruent) insert and where does it fit between CR and PS? A: An ultracongruent, deep-dished polyethylene with a raised anterior lip run on a standard CR (box-less) femur; the PCL is sacrificed and AP stability comes from articular conformity, not a cam-post. It avoids the box cut (preserving posterior femoral bone) and avoids post-related complications (clunk, post fracture/wear), but gives no guaranteed mechanical rollback and relies on good gap balance - a grossly unbalanced knee can still spin out because there is no post to capture the femur.
Clinical Presentation and Indications
Patient Assessment for Implant Selection
The choice between CR and PS TKA begins with thorough patient assessment. Key factors include:
Clinical examination:
- PCL integrity: Posterior drawer test at 90 degrees flexion
- Deformity assessment: Varus/valgus alignment and degree
- Range of motion: Flexion contracture and maximum flexion
- Ligamentous stability: Assess collateral ligament competence
Radiographic evaluation:
- Standing AP and lateral radiographs: Measure deformity, bone stock
- Varus/valgus stress views: Assess ligament integrity
- Skyline view: Evaluate patellofemoral joint
Demographics:
- Age: Younger patients may benefit from CR (bone preservation)
- Activity level: High-demand patients may prefer PS (predictable kinematics)
- Cultural practices: Deep flexion requirements (kneeling, squatting)
Comorbidities:
- Inflammatory arthropathy: Strong indication for PS
- Neurological conditions: May benefit from PS constraint
- Previous trauma or surgery: May compromise PCL quality
Pathophysiology and Biomechanics
Normal Knee Kinematics (Intact PCL Function)
Flexion Arc Kinematics
Femoral motion: Minimal translation, primarily rotation. PCL role: Minimal tension, ACL is primary stabilizer. Clinical relevance: Both CR and PS behave similarly in this range.
Femoral motion: Progressive posterior rollback begins (5-10mm). PCL role: Increasing tension guides femoral condyle rollback. Clinical relevance: CR relies on PCL tension; PS cam-post begins engagement at 60-70 degrees.
Femoral motion: Maximal posterior rollback (10-15mm total). PCL role: Maximum PCL tension, prevents posterior translation. Clinical relevance: PS cam-post fully engaged, provides consistent 15-20mm rollback. CR variable depending on PCL tension.
Kinematic Differences: CR vs PS
- Cruciate Retaining (CR)
- 10-15mm (PCL-dependent, variable)
- Posterior Stabilized (PS)
- 15-20mm (cam-post, consistent)
- Clinical Significance
- PS provides more predictable posterior femoral translation
- Cruciate Retaining (CR)
- 120-130 degrees (average)
- Posterior Stabilized (PS)
- 130-140 degrees (average)
- Clinical Significance
- 10-20 degrees greater flexion potential with PS, but minimal functional impact
- Cruciate Retaining (CR)
- Lower conformity, higher stress
- Posterior Stabilized (PS)
- Higher conformity, distributed stress
- Clinical Significance
- PS has lower peak contact stress but higher constraint
- Cruciate Retaining (CR)
- More common (up to 20%)
- Posterior Stabilized (PS)
- Rare (under 5%)
- Clinical Significance
- CR may show anterior femoral translation in mid-flexion if PCL too loose
Investigations and Preoperative Assessment
Imaging Studies for PCL Assessment
- Purpose
- Assess deformity and bone stock
- Key Findings
- Varus/valgus angle, joint space narrowing, bone defects
- Influence on Design Choice
- Severe deformity (over 15 degrees) favors PS
- Purpose
- Evaluate PCL calcification and posterior bone stock
- Key Findings
- PCL calcification, posterior osteophytes, femoral bone loss
- Influence on Design Choice
- PCL calcification suggests poor function (favors PS)
- Purpose
- Detailed PCL and soft tissue assessment
- Key Findings
- PCL integrity, fiber continuity, signal changes indicating degeneration
- Influence on Design Choice
- Attenuated or torn PCL is absolute indication for PS
- Purpose
- Assess ligamentous laxity and deformity correctability
- Key Findings
- Degree of deformity correction with stress, ligament competence
- Influence on Design Choice
- Fixed deformity over 15 degrees favors PS for easier balancing
Final decision on CR vs PS often made intraoperatively. After exposure and initial bone preparation, directly palpate PCL substance. If PCL feels soft, attenuated, or calcified, plan for PS. After trial component insertion, perform posterior drawer test at 90 degrees flexion - if translation exceeds 5mm with soft endpoint, convert to PS. Always have PS instruments available as backup for planned CR cases.
Laboratory Studies
For most primary OA cases, extensive laboratory workup is not required. However, specific scenarios warrant investigation:
- Inflammatory arthropathy: ESR, CRP, RF, anti-CCP antibodies (strong PS indication)
- Infection screening: ESR, CRP, synovial fluid analysis if effusion present
- Metabolic bone disease: Vitamin D, calcium, parathyroid hormone if suspected
- Coagulopathy screening: INR, PT/PTT if on anticoagulation
Management Principles and Implant Selection
Ideal Indications for CR TKA
Absolute requirements:
- Intact PCL: No significant attenuation, calcification, or dysfunction
- Adequate bone stock: Posterior femoral condyles intact, no large defects
- Mild-moderate deformity: Under 15 degrees varus or valgus angulation
- Primary OA: Non-inflammatory etiology with preserved soft tissue quality
Relative advantages:
- Preservation of bone stock (no femoral box cut or tibial post)
- Theoretical proprioception benefit from PCL mechanoreceptors
- Lower polyethylene conformity allows greater rotational freedom
- Avoids cam-post complications (clunk, wear, dissociation)
Intraoperative assessment: After trial reduction, flex knee to 90 degrees and apply posterior drawer. If excessive translation (greater than 5mm) or loose PCL feel, consider converting to PS. Tight PCL requires careful posterior capsule release; if still tight after releases, consider PS to avoid flexion instability.
Patient factors favoring CR:
- Younger, higher-demand patients (preserves bone stock for future revision)
- Patients with good PCL on preoperative imaging (MRI showing intact fibers)
- Cultural practices requiring deep flexion (kneeling, squatting) - controversial, PS may actually be better
These patient factors help guide CR selection when PCL is intact.
Surgical Technique Considerations
PCL Balancing in CR TKA
PCL Assessment and Balancing Steps
Imaging evaluation: Assess PCL integrity on lateral radiograph (calcification?) and MRI if available (intact fibers?). Physical exam: Posterior drawer test at 90 degrees flexion - should be firm endpoint. Excessive laxity suggests PCL incompetence.
Exposure: After arthrotomy and synovectomy, palpate PCL substance. Should feel firm, taut, and continuous. Red flags: Soft, attenuated, or calcified PCL suggests poor function. Consider converting to PS if concerns about PCL quality.
Flexion gap test: With trial components in place, flex knee to 90 degrees. Apply posterior drawer force. Normal PCL: Minimal translation (under 5mm), firm endpoint. Tight PCL: Flexion gap opens posteriorly, difficult to flex to 90 degrees. Loose PCL: Excessive posterior translation (over 5mm), soft endpoint.
If PCL too tight:
- First, release posterior capsule (most common cause)
- If still tight, consider "pie-crusting" PCL with 11-blade (controversial)
- If persistently tight, convert to PS (avoid flexion instability)
If PCL too loose:
- Increase tibial insert thickness (1-2mm increments)
- Ensure adequate femoral component size (not too small)
- If persistently loose, convert to PS (avoid posterior tibial translation and wear)
Overtightening the PCL causes flexion instability, pain, and limited ROM. Patients cannot flex beyond 90 degrees comfortably. Undertightening the PCL leads to posterior tibial subluxation, paradoxical anterior slide, and accelerated polyethylene wear. Golden rule: If in doubt about PCL quality or balance after careful assessment, convert to PS intraoperatively.
CR-Specific Technical Pearls
Technique: Use blunt Hohmann retractor to elevate posterior capsule off posterior femoral condyles. Start medially, work laterally. Release should be subperiosteal to avoid popliteal vessel injury. Goal: Create 1-2mm of additional flexion gap without overstretching PCL.
Danger: PCL inserts just posterior to posterior edge of tibial cut. Overly posterior tibial resection can detach PCL, forcing conversion to PS. Protection: Keep tibial cut at approximately 0 degrees posterior slope (or slightly anterior). Mark PCL insertion before cutting.
These techniques ensure optimal PCL balance and implant function.
Posterior Tibial Slope and the Cruciate Strategy
The CR technique tab gives a specific slope instruction - "keep the tibial cut at approximately 0 degrees posterior slope... overly posterior tibial resection can detach the PCL" - but the topic never explains why posterior slope matters differently for CR and PS, which is a classic viva point (generic alignment is covered in the tka-alignment topics; this is the cruciate-specific interaction).
- What slope does. Posterior tibial slope opens the flexion gap (more slope gives a larger flexion gap and easier deep flexion) and shifts the femoral contact point posteriorly. It must be matched to the specific implant's design intent.
- In CR - protect and respect the PCL. Because the PCL is retained, slope is kept modest and implant-specific (commonly around 0 to 7 degrees). Excessive posterior slope over-opens the flexion gap and alters PCL tension, worsening paradoxical anterior femoral slide and risking flexion instability; a very deep/posterior tibial cut can detach the PCL footprint (forcing conversion to PS). The PCL insertion is protected by not over-resecting posteriorly and keeping slope conservative.
- In PS - more latitude, but new limits. With the PCL excised, slope can be used more liberally to aid flexion, but too much slope in a PS knee risks anterior femoral lift-off, edge-loading or impingement of the cam-post in flexion, and recurvatum/hyperextension instability; excessive slope also increases posterior loading of the fixation. Slope is therefore still set to the manufacturer's recommendation for that PS design.
- Both designs. Avoid excessive slope (over-opens the flexion gap) and avoid anterior (reverse) slope (tightens the flexion gap and can cause flexion stiffness / limited flexion). Match the cut to the implant, not to a single universal number.
Q: Why does posterior tibial slope matter differently in CR versus PS TKA? A: Slope opens the flexion gap. In CR, the retained PCL constrains how much slope you can use - excessive slope over-tensions/alters the PCL, worsens paradoxical anterior slide and can cause flexion instability, and a too-posterior cut can detach the PCL - so slope is kept modest and implant-specific. In PS, the PCL is gone so more slope aids flexion, but too much risks anterior lift-off, cam-post edge-loading/impingement and recurvatum. Always match slope to the specific implant's recommendation, and avoid reverse (anterior) slope, which stiffens flexion.
Complications
- CR-Specific
- PCL too loose or avulsed
- PS-Specific
- Inadequate cam-post engagement
- Incidence
- CR: 2-5%, PS: under 1%
- Management
- CR: Thicker insert or convert to PS; PS: Check post height, consider revision
- CR-Specific
- Rare (no femoral box)
- PS-Specific
- Common (5-10% incidence)
- Incidence
- PS-specific complication
- Management
- Arthroscopic debridement of fibrous nodule (90% resolution)
- CR-Specific
- Not applicable
- PS-Specific
- Tibial post fracture (under 1%)
- Incidence
- PS-specific late failure
- Management
- Revision with thicker insert or constrained condylar knee
- CR-Specific
- PCL incompetence (1-3%)
- PS-Specific
- Rare with functional cam-post
- Incidence
- CR: Higher polyethylene wear
- Management
- CR: Consider revision to PS if symptomatic wear
- CR-Specific
- Minimal (no box cut)
- PS-Specific
- Posterior femoral defect from box
- Incidence
- PS: 5-7mm bone loss
- Management
- Both: Augments or metaphyseal sleeves at revision
Outcomes and Prognosis
Key outcomes (national joint registries, Cochrane and meta-analyses):
- Survivorship: Equivalent revision rates at 10 years, both over 95% survivorship (no significant difference)
- Function: WOMAC and KSS scores equivalent at 5-10 years, patient satisfaction 85-90% for both
- ROM: CR 120-130°, PS 130-140° flexion; meta-analyses show a 5-7° advantage to PS of uncertain clinical relevance
- Complications: PS higher patellofemoral/clunk issues, CR higher instability - small absolute differences
Guidelines, Registries & Global Practice
Global Epidemiology and Practice Variation
TKA is one of the highest-volume elective orthopaedic procedures worldwide, with over 2 million implanted annually and demand rising with ageing populations and increasing obesity. The CR-versus-PS choice varies markedly by region: PS designs dominate in much of North America and parts of Asia, while CR (and minimally-stabilised) designs retain a larger share in Scandinavia and parts of Europe. These patterns reflect training era, implant availability, and institutional standardisation rather than any proven outcome superiority.
Society Guidance and Registry Evidence
- Position on CR vs PS
- No mandate for one design; evidence shows comparable function and survivorship
- Practical Emphasis
- Surgeon judgement and patient factors drive selection
- Position on CR vs PS
- Prioritise implants with strong registry survivorship (ODEP-rated); design class secondary
- Practical Emphasis
- Use benchmarked implants; both CR and PS qualify
- Position on CR vs PS
- Broadly equivalent 10-year revision; failure mode differs (PS patellofemoral, CR instability)
- Practical Emphasis
- Track design-specific revision signals over time
- Position on CR vs PS
- Design choice individualised; PS favoured for marked deformity or PCL incompetence
- Practical Emphasis
- Reserve higher constraint for instability or deficiency
Resource-Setting Variation
- Full inventory of CR, PS and constrained options on the shelf
- Routine intraoperative ability to convert CR to PS
- Preoperative MRI and registry-benchmarked implant selection available
- Choice often driven by institutional standardisation and surgeon training
- Single design platform may be stocked to control cost and complexity
- PS often preferred where soft-tissue quality is unpredictable and balancing expertise variable
- Backup constrained implants may be unavailable, raising the threshold for complex deformity
- Emphasis on a reliable, reproducible technique over design optimisation
Counsel patients that CR and PS achieve equivalent long-term function and survivorship, that intraoperative conversion from CR to PS is possible if the PCL is found incompetent, and that each design carries distinct complications (PS: patellar clunk; CR: flexion instability if the PCL is poorly balanced). Document preoperative PCL assessment, intraoperative findings and the rationale for final implant choice or conversion.
Controversies and Areas of Uncertainty
Meta-analyses (Bercik 2013, Jiang 2016) show a statistically greater ROM with PS (roughly 5-7 degrees), but the clinical relevance is unproven - patient-reported function and satisfaction are equivalent. The difference is unlikely to matter for most daily activities.
It is often claimed CR better suits squatting/kneeling cultures by preserving native kinematics, yet fluoroscopic data show CR can exhibit paradoxical anterior slide, and PS gives more reliable rollback. Evidence does not clearly favour either design for high-flexion lifestyles.
A theoretical proprioceptive benefit from retaining PCL mechanoreceptors is frequently cited, but no robust clinical evidence demonstrates a measurable functional advantage attributable to PCL proprioception after CR TKA.
CR avoids the femoral box cut and theoretically preserves bone for revision. Whether this translates into easier or better revision outcomes is not established; modern revision systems readily manage the box-cut defect.
Mnemonics and Design Frameworks
ROLLPCL Functions (Why CR Needs Intact PCL)
Hook:PCL makes the femur ROLL back - CR designs need this intact!
FACESPS Design Advantages (Cam-Post Mechanism)
Hook:PS design FACES the challenge of PCL loss with cam-post mechanics!
SLIMCR Design Requirements (What You Need)
Hook:Keep it SLIM - CR needs intact structures and mild deformity!
MCQ Practice Points
Q: At what degree of flexion does the cam-post mechanism in PS TKA typically engage to provide posterior femoral rollback? A: 60-70 degrees of flexion. The cam (on the femoral component) contacts the post (on the tibial polyethylene insert) at this flexion range, initiating the mechanical substitute for PCL function. This engagement provides consistent posterior femoral rollback of 15-20mm compared to the variable 10-15mm seen in CR designs (dependent on PCL tension).
Q: What is the deformity threshold (varus or valgus angulation) above which PS TKA is generally preferred over CR TKA? A: Greater than 15 degrees of varus or valgus deformity. Severe deformities require extensive soft tissue releases which may compromise PCL function. PS designs eliminate reliance on PCL quality and provide predictable stability through the cam-post mechanism, making soft tissue balancing more straightforward in these challenging cases.
Q: What is the mechanism and incidence of patellar clunk syndrome in PS TKA? A: Mechanism: Fibrous nodule forms on the superior pole of the patella and catches on the superior aspect of the femoral box during extension from deep flexion, producing a painful, palpable clunk between 100-40 degrees. Incidence: 5-10% in early PS designs, reduced to 2-5% in modern designs with improved femoral box geometry. Treatment: Arthroscopic debridement (85-95% success rate).
Q: According to national joint registries and international evidence, what is the 10-year survivorship comparison between CR and PS TKA in primary osteoarthritis? A: Equivalent survivorship: Both CR and PS designs achieve over 95% survivorship at 10 years. The Cochrane meta-analysis of 17 RCTs (Verra 2013) and large joint registries (AOANJRR, NJR, AJRR) confirm no clinically significant difference in revision rates (both typically under 6% at 10 years). Functional outcomes (ROM, KSS, WOMAC scores) are also equivalent. Complication profiles differ slightly (PS higher patellofemoral/clunk issues, CR higher instability) but overall outcomes are comparable.
Q: What are the critical steps in assessing PCL integrity and balance during CR TKA trial reduction? A: Assessment technique: (1) With trial components in place, flex knee to 90 degrees. (2) Apply posterior drawer force to tibia. (3) Normal PCL should limit translation to under 5mm with firm endpoint. (4) Excessive translation (over 5mm) indicates PCL incompetence. (5) Troubleshoot by increasing insert thickness or checking femoral size. (6) If translation remains over 5mm despite adjustments, convert to PS intraoperatively. Key principle: A loose or insufficient PCL will cause posterior tibial subluxation and accelerated wear in CR designs.
Q: What does the Cochrane systematic review (Verra 2013) conclude about functional outcomes and ROM differences between CR and PS TKA? A: No clinically relevant difference. The meta-analysis of 17 RCTs (1810 patients, 2206 knees) found only two small statistically significant differences, both judged clinically irrelevant: (1) ROM was 2.4 degrees higher with PCL sacrifice (118.3 vs 115.9 degrees; heterogeneous). (2) Functional Knee Society Score was 2.3 points higher with sacrifice (81.2 vs 79.0). (3) WOMAC total, knee pain and patient satisfaction were equivalent. (4) Implant survival could not be assessed - the RCTs lacked long-term follow-up (only 4 revisions in each group), so the equivalence of 10-year survivorship rests on registry data, not this Cochrane review. Clinical implication: choose CR vs PS on patient-specific factors (PCL quality, deformity) and surgeon experience, not expected functional superiority.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman with severe medial compartment osteoarthritis presents for TKA. She has 12 degrees varus deformity and an intact PCL on clinical examination. She asks about the difference between cruciate retaining and posterior stabilized implants. How would you counsel her and what are the key factors in your implant selection?”
“You are performing a CR TKA on a 62-year-old man with primary OA. After inserting the trial components, you notice excessive posterior tibial translation (approximately 8mm) on posterior drawer testing at 90 degrees flexion. The PCL feels somewhat loose. Walk me through your assessment and management options.”
“A 55-year-old woman returns 18 months after PS TKA complaining of a painful, palpable clunk in her knee during extension from deep flexion. She describes it as occurring around 60-70 degrees of flexion during activities like standing from a chair. Examination demonstrates a reproducible clunk with active extension from 100 to 40 degrees. What is your diagnosis and management approach?”
Design Fundamentals
- CR = Preserves PCL for physiologic rollback (10-15mm), requires intact PCL and mild deformity (under 15 degrees)
- PS = Sacrifices PCL, cam-post mechanism provides consistent rollback (15-20mm), independent of PCL quality
- CS = Intermediate design with deep dish polyethylene, no post (less common)
- PCL function: Prevents posterior tibial translation, guides femoral rollback, maintains quadriceps lever arm
Selection Criteria
- CR indications: Intact PCL, mild-moderate OA, deformity under 15 degrees, desire to preserve bone stock
- PS indications: PCL deficiency, severe deformity (over 15 degrees), inflammatory arthritis, revision TKA, flexion contracture over 15 degrees
- Neutral zone: Primary OA with mild deformity (under 10 degrees) - either CR or PS acceptable, surgeon preference
- Intraoperative conversion: CR to PS if PCL loose (over 5mm translation), attenuated, or avulsed
Biomechanics
- Cam-post engagement: 60-70 degrees flexion in PS designs, provides mechanical PCL substitute
- Femoral rollback: CR variable 10-15mm (PCL-dependent), PS consistent 15-20mm (cam-post)
- Flexion range: CR 120-130 degrees average, PS 130-140 degrees (10-20 degrees greater with high-flex designs)
- Paradoxical anterior slide: More common in CR (up to 20%) if PCL too loose, rare in PS (under 5%)
Surgical Technique
- CR PCL balancing: Posterior drawer at 90 degrees should be under 5mm; if tight, release posterior capsule; if loose, thicker insert or convert to PS
- PS femoral box cut: 18-20mm wide, 12-15mm deep, creates 5-7mm posterior femoral bone loss
- Cam-post clearance: 2-3mm at full extension to avoid hyperextension impingement, engagement begins 60-70 degrees
- Conversion CR to PS: Excise PCL, create femoral box cut, verify tibial baseplate accepts PS insert, trial balance
Complications
- PS-specific: Patellar clunk syndrome (5-10%, fibrous nodule on superior patella catches on box), cam-post wear/dissociation (under 1%)
- CR-specific: Flexion instability from PCL imbalance (2-5%), PCL avulsion, posterior tibial translation and wear if PCL loose
- Patellar clunk treatment: Conservative 3-6 months (physio), then arthroscopic debridement (85-95% success)
- Both: Infection, aseptic loosening, stiffness, periprosthetic fracture - no difference in rates between CR and PS
Evidence Base and Key Studies
Key Evidence
Cochrane Review: PCL Retention vs Sacrifice in TKA
- Meta-analysis of 17 RCTs (1810 patients, 2206 knees) for primary OA
- Range of motion 2.4 degrees higher with PCL sacrifice (118.3 vs 115.9 degrees) - heterogeneous, not clinically relevant
- Functional Knee Society Score 2.3 points higher with sacrifice (81.2 vs 79.0) - not clinically relevant
- WOMAC total and patient satisfaction equivalent between groups
- 4 revisions in each group; RCTs lacked follow-up to assess long-term survival
National Joint Registries: CR vs PS Revision Rates
- Large-volume registry data (hundreds of thousands of primary TKAs) compare CR and minimally/posterior-stabilised designs
- Cumulative revision rates are broadly similar between CR and PS at 10 years (both typically under 6%)
- PS designs trend toward more patellofemoral/clunk-related revisions
- CR designs trend toward more instability-related revisions
- Both designs achieve over 95% survivorship at 10 years with modern implants
In Vivo Kinematics: Cruciate Sacrifice vs Substitution
- In vivo weight-bearing videofluoroscopy during gait and deep-knee bend
- Kinematic patterns were similar during gait between PS and cruciate-sacrificing designs
- During deep-knee bend, PS knees showed more posterior femoral rollback of the lateral condyle
- Findings mirror earlier comparisons of fixed-bearing CR vs PS designs
- Differences emerge mainly in deep flexion, not in level gait
Patellar Clunk Incidence: Fixed vs High-Flex Mobile Bearing PS
- 411 PS TKAs reviewed (188 mobile high-flex, 223 fixed bearing)
- Patellar clunk developed in 11.7% of mobile high-flex vs 1.8% of fixed bearing knees (p less than 0.001)
- Intercondylar box geometry is a key driver of clunk development
- 23 of 26 cases resolved with a single arthroscopic debridement; 2 needed a second procedure
- Despite clunk, overall range of motion (mean 122 degrees) and satisfaction remained high
Meta-Analysis of RCTs: CR vs PS Outcomes
- Meta-analysis of RCTs comparing CR and PS designs (1114 patients, 1265 knees)
- Significant difference in flexion and total range of motion favouring PS
- No significant difference in complication rates between designs
- Clinical importance of the ROM difference remains unknown
- Design choice should rest with surgeon preference and familiarity
Meta-Analysis: PCL Retention vs Posterior Stabilization
- Meta-analysis of 14 RCTs comparing CR and PS TKA
- No significant difference in Knee Society Score, pain score, or HSS score
- No difference in component alignment, tibial slope, joint line, or complication rate
- PS superior for postoperative ROM (mean difference approximately 7 degrees) and ROM improvement
- Whether the ROM advantage is clinically meaningful needs longer follow-up