Prevention Strategies | MUA Timing | Revision Options | Outcomes
- MUA timing: Most effective between 6-12 weeks post-TKA, avoid after 6 months due to fracture risk
- Flexion under 90° significantly impacts activities of daily living and quality of life
- Risk factors: Previous surgery, infection, CRPS, component malposition, stiff preoperative ROM
- Prevention is key: optimal component positioning, early mobilization, aggressive physiotherapy
- Manipulation success drops significantly after 12 weeks - act early if ROM not improving
- “MUA can be repeated if first attempt unsuccessful, but diminishing returns after second manipulation
- “Arthroscopic lysis of adhesions (6 weeks to 6 months) has better outcomes than late revision
- “Component malposition (especially oversized femoral component) is a correctable mechanical cause
- “Always rule out infection and CRPS before attributing stiffness to arthrofibrosis alone
Stiffness is flexion under 90° at 12 weeks post-TKA. This threshold is critical because it limits stair climbing, rising from chairs, and entering/exiting vehicles. Extension deficits over 10° cause limping and anterior knee pain. Early recognition is essential for successful intervention.
Optimal timing: 6-12 weeks post-TKA. Success rate 75-85% in this window. After 12 weeks, collagen cross-linking matures and manipulation becomes less effective. After 6 months, fracture risk increases significantly. If first MUA fails, repeat within 2 weeks.
Surgical factors: Avoid component oversizing (especially femoral), restore joint line height, balance flexion/extension gaps. Postoperative: CPM machines (controversial), early mobilization, aggressive PT, pain control. Address psychological factors and CRPS early.
Mechanical causes: Component malposition, patella baja, anterior impingement, overstuffing. Failed conservative: MUA unsuccessful, persistent flexion under 70°, significant functional limitation. Arthroscopic lysis (under 6 months) before open revision (after 6 months).
- Timing
- Under 6 weeks post-TKA
- Primary Management
- Aggressive physiotherapy, pain control
- Key Pearl
- Wait until 6-12 week window for MUA if no improvement
- Timing
- 6-12 weeks post-TKA
- Primary Management
- Manipulation under anesthesia (MUA)
- Key Pearl
- Best success window - act now, avoid waiting
- Timing
- 3-6 months post-TKA
- Primary Management
- Arthroscopic lysis of adhesions
- Key Pearl
- Better outcomes than late open revision
- Timing
- Any time
- Primary Management
- Revision TKA to correct alignment
- Key Pearl
- Address mechanical cause - PT alone will fail
REVISERevision Surgery Considerations (Post-MUA Failure)
Hook:REVISE the technical factors if MUA fails - most stiffness has a correctable mechanical cause!
Overview and Epidemiology
TKA stiffness is one of the most common reasons for patient dissatisfaction after an otherwise technically successful arthroplasty. While mild stiffness (flexion 90-110°) may not significantly impact function, flexion under 90° prevents normal activities of daily living including stair climbing, rising from chairs, and entering/exiting vehicles. Extension deficits over 10° cause limping, anterior knee pain, and difficulty with level walking. Early recognition and intervention are critical as outcomes worsen significantly with delayed treatment.
- Walking: 0-70° (extension to 70° flexion)
- Stairs ascending: 0-83° flexion required
- Stairs descending: 0-90° flexion required
- Rising from chair: 95° flexion minimum
- Tying shoes: 110-120° flexion needed
- Sitting comfortably: 90-100° flexion
The functional threshold is 90° flexion - below this, significant ADL limitations occur.
- Weeks 0-6: Gradual ROM improvement with PT
- 6 weeks: Should achieve 90° flexion minimum
- 12 weeks: ROM typically plateaus (110-120° flexion)
- 6-12 months: Minimal further improvement expected
If ROM is not progressing by 6 weeks or plateaus under 90°, intervention should be considered before 12-week mark.
Aetiology and Risk Factors
Non-modifiable: Female gender, previous knee surgery, genetic predisposition, inflammatory arthritis, diabetes
Modifiable: Component positioning, gap balancing, joint line restoration, pain control, early mobilization, psychological factors
Focus prevention strategies on the modifiable factors to minimize stiffness incidence.
Patient Risk Factors
- Female gender: 2-3x higher incidence
- Age under 60: Higher expectations, more active
- BMI over 35: Mechanical disadvantage
- Diabetes: Impaired healing, fibrosis tendency
- Smoking: Delayed healing, fibrosis
- Inflammatory arthritis: RA, psoriatic arthritis
- Preoperative flexion under 90°: Strongest predictor
- Flexion contracture over 10°: Soft tissue contracture
- Previous knee surgery: Scar tissue, adhesions
- Patella baja: Extensor mechanism dysfunction
- Chronic effusion: Synovial inflammation
Surgical Risk Factors
- Mechanism
- Overstuffs patellofemoral joint, limits flexion
- Clinical Finding
- Anterior knee pain, inability to flex past 90°
- Prevention
- Template preoperatively, size down if between sizes
- Mechanism
- Patellar maltracking, Q-angle increase
- Clinical Finding
- Patella subluxation, anterior pain with flexion
- Prevention
- Use transepicondylar axis, avoid rotating internally
- Mechanism
- Patella baja, extensor mechanism tightening
- Clinical Finding
- Difficulty with stairs, anterior impingement
- Prevention
- Restore anatomical joint line (use distal femoral cut)
- Mechanism
- Overstuffed posterior compartment
- Clinical Finding
- Hard endpoint to flexion, pain
- Prevention
- Balance gaps, posterior femoral condyle recession
- Mechanism
- Overstuffing both flexion and extension
- Clinical Finding
- Global stiffness, pain throughout arc
- Prevention
- Choose thinnest poly for balanced gaps
Prevention Strategies
Preoperative Planning:
- Template for component sizing
- Plan osteophyte removal
- Consider preoperative ROM and set realistic goals
- Counsel patients with flexion under 90° about stiffness risk
Intraoperative Technique:
- Restore joint line height (within 5mm of anatomic)
- Balance flexion and extension gaps (within 2mm)
- Avoid component oversizing (size down if borderline)
- Ensure proper rotation (transepicondylar axis, Whiteside's line)
- Remove all osteophytes (especially posterior femoral)
- Test ROM on table - should achieve 120° flexion minimum
These intraoperative measures prevent mechanical causes of stiffness.
STIFF KNEERisk Factors for TKA Stiffness
Hook:A STIFF KNEE won't bend - remember all modifiable and non-modifiable risk factors to prevent this complication!
Anatomy and Biomechanics
Knee Joint Biomechanics in TKA
- Flexion arc: 0-135° in native knee, 0-120° typical post-TKA
- Rollback: Posterior femoral translation with flexion (10-15mm)
- Patellofemoral tracking: Critical for pain-free flexion
- Tibiofemoral contact: Moves posterior with increasing flexion
Stiffness disrupts normal kinematics through adhesions or mechanical impingement.
- Suprapatellar pouch: Adhesions here limit flexion (most common site)
- Posterior capsule: Contracture limits flexion, scar limits rollback
- Quadriceps/patellar tendon: Shortening or tethering impairs gliding
- Periarticular soft tissue: Inflammation causes global fibrosis
Primary arthrofibrosis targets these structures with excessive collagen deposition.
Pathophysiology of Arthrofibrosis
Fibrosis Development Timeline
Process: Surgical trauma triggers inflammatory cascade with cytokine release (IL-1, TNF-α), fibrin deposition, and myofibroblast activation.
Clinical: Swelling, pain, limited ROM from effusion and muscle guarding.
Prevention at this stage focuses on controlling inflammation and early mobilization.
Process: Fibroblasts proliferate and deposit immature collagen (Type III), adhesions form between synovium and surrounding tissues.
Clinical: ROM may plateau as adhesions mature, "rubbery" endpoint to passive flexion.
This is the window where aggressive PT is most effective before collagen matures.
Process: Type III collagen converted to Type I (stronger, less elastic), cross-linking increases tensile strength of scar.
Clinical: Firm endpoint to ROM, adhesions palpable, progressive loss of motion if untreated.
Optimal MUA window - before collagen fully matures (maximal ROM gain with minimal fracture risk).
Process: Dense mature scar with extensive cross-linking, heterotopic ossification may develop in posterior capsule.
Clinical: Hard endpoint, minimal improvement with PT, may feel "bony block" on exam.
MUA less effective, higher fracture risk - consider arthroscopic lysis or revision.
Emerging evidence suggests genetic factors influence fibrotic response after TKA:
- TGF-β1 polymorphisms: Associated with increased collagen production
- MMP gene variants: Reduced matrix metalloproteinase activity impairs scar remodeling
- Family history: Patients with family history of keloids or Dupuytren's contracture at higher risk
While not modifiable, awareness helps identify high-risk patients for closer ROM monitoring postoperatively.
Joint Line Height and Stiffness
Joint line elevation (from excessive distal femoral resection or undersized femoral component) causes:
- Patella baja (Insall-Salvati ratio under 0.8)
- Anterior impingement between patella and polyethylene insert
- Functional extensor mechanism tightening
- Flexion limitation (mechanical block at 70-90°)
This is a correctable mechanical cause requiring revision to restore anatomical joint line height, not amenable to MUA or PT alone.
Localizing the Cause by the Arc Affected
The aetiology section lists the technical causes of stiffness, but a more useful examiner habit is to note WHICH part of the arc is lost - flexion, extension, or both - because the pattern localizes the mechanical cause and tells you which lever to pull. A knee tight only in flexion has a different problem from one that cannot fully extend.
- Likely mechanical cause
- Tight flexion gap; oversized or anteriorly-positioned femoral component; retained posterior femoral osteophytes; patella baja / elevated joint line; inadequate posterior tibial slope
- Corrective lever
- Downsize or reposition the femoral component, remove posterior osteophytes, restore joint-line height, reassess polyethylene thickness
- Likely mechanical cause
- Tight extension gap; retained posterior osteophytes tenting the capsule; posterior capsular contracture; under-resected distal femur
- Corrective lever
- Remove posterior osteophytes, posterior capsular release, recut distal femur or use a thinner polyethylene
- Likely mechanical cause
- Overstuffing (oversized components or polyethylene), true arthrofibrosis, infection, CRPS
- Corrective lever
- Exclude infection and CRPS first; downsize if overstuffed; MUA or arthroscopic lysis for arthrofibrosis
Before labelling a stiff TKA "arthrofibrosis", note WHICH part of the arc is lost - it localizes the mechanical cause. A knee tight only in flexion points to the flexion gap (oversized or anterior femoral component, retained posterior osteophytes, patella baja); a knee that cannot fully extend (fixed flexion deformity) points to the extension gap (retained posterior osteophytes, posterior capsular contracture, an under-resected distal femur); a knee tight throughout suggests overstuffing, true arthrofibrosis, or - never forget - infection or CRPS. The pattern tells you which lever to pull at revision, and a uniformly stiff, hot, painful knee is infection until proven otherwise.
Patellar Clunk Syndrome and Patellar Crepitus
The arthroscopic-lysis section mentions "notchplasty if anterior impingement" and adhesions in the suprapatellar pouch. These point to a specific posterior-stabilized (PS) design complication that is worth naming: patellar clunk syndrome.
A fibrous nodule forms at the junction of the posterior quadriceps tendon and the superior pole of the patella. In PS designs (which have an intercondylar femoral box), as the knee actively EXTENDS from deep flexion (around 30-45 degrees) the nodule catches on the superior edge of the box and jumps free, producing a painful, audible or palpable "clunk" - classically on rising from a chair or climbing stairs. It is distinct from the milder, diffuse patellar crepitus.
- Patellar clunk
- Discrete fibrous nodule at the quadriceps-superior patella junction
- Patellar crepitus
- Diffuse peripatellar fibrosynovial tissue / softer scar
- Patellar clunk
- Painful audible or palpable CLUNK as the knee actively extends from flexion (around 30-45 degrees)
- Patellar crepitus
- Grinding or crepitus through the arc, usually milder
- Patellar clunk
- Nodule catches on the superior edge of the intercondylar femoral box of a posterior-stabilized implant
- Patellar crepitus
- Synovial tissue impinges in the patellofemoral track
- Patellar clunk
- Arthroscopic (or open) excision of the nodule, usually with peripatellar debridement - reliably relieves symptoms
- Patellar crepitus
- Often responds to observation and physiotherapy; arthroscopic debridement if persistent
Patellar clunk syndrome is a posterior-stabilized-design complication: a fibrous nodule at the junction of the quadriceps tendon and the superior patella catches on the superior edge of the femoral intercondylar box, producing a painful clunk as the knee extends from flexion (around 30-45 degrees), classically on rising from a chair or climbing stairs. Suspect it when a "catching" or stiff PS TKA has a discrete, reproducible clunk, and distinguish it from the milder diffuse patellar crepitus. Treatment is arthroscopic excision of the nodule with peripatellar debridement, which reliably relieves symptoms; newer femoral box geometries have reduced its incidence.
Classification of TKA Stiffness
Primary vs Secondary Stiffness
- Definition
- Idiopathic fibrotic response, no clear cause
- Risk Factors
- Genetic predisposition, female, smoking
- Management Approach
- Early aggressive PT, MUA if persistent
- Definition
- Component malposition or sizing error
- Risk Factors
- Oversized components, malrotation, patella baja
- Management Approach
- Identify and correct mechanical cause
- Definition
- Infection, CRPS, inflammatory arthritis
- Risk Factors
- Wound complications, pain out of proportion
- Management Approach
- Treat underlying condition first
Primary arthrofibrosis is a diagnosis of exclusion - always rule out correctable mechanical and inflammatory causes first.
Clinical Assessment
- Onset: Gradual vs sudden (sudden suggests component issue)
- Progression: Improving, static, or worsening
- Pain: Location (anterior = PF, global = overstuffing)
- Functional loss: Specific activities affected
- Compliance: PT attendance, home exercise
- Previous surgery: Prior procedures increase risk
- CRPS symptoms: Pain out of proportion, allodynia
- Flexion ROM: Measure actively and passively (hard vs soft endpoint)
- Extension: Any flexion contracture over 10° is significant
- Wound: Check for persistent drainage (infection)
- Effusion: Chronic effusion suggests infection or instability
- Neurovascular: CRPS signs (allodynia, temperature change)
- Gait: Extension deficit causes limp
- Patella tracking: Maltracking suggests rotation error
Always rule out before attributing to arthrofibrosis:
- Infection: Persistent wound drainage, fever, elevated CRP/ESR
- CRPS: Pain out of proportion, allodynia, temperature asymmetry
- Component loosening: Pain with weight-bearing, radiolucent lines
- Instability: Giving way, effusion, pain with pivoting
- Periprosthetic fracture: Sudden onset after manipulation
- Heterotopic ossification: Palpable mass, progressive loss of ROM
Infection is the most important diagnosis not to miss - low threshold for aspiration if any suspicion.
Differential Diagnosis of the Stiff or Painful TKA
- Typical Features
- Gradual ROM loss, soft/'rubbery' endpoint, no malposition
- Key Discriminator
- Diagnosis of exclusion once mechanical and infective causes excluded
- Confirmatory Test
- Normal inflammatory markers and well-positioned components on imaging
- Typical Features
- Effusion, warmth, rest/night pain, persistent drainage
- Key Discriminator
- Pain out of proportion with raised inflammatory markers
- Confirmatory Test
- ESR/CRP then synovial aspiration (cell count, culture, alpha-defensin)
- Typical Features
- Hard mechanical block, anterior pain, maltracking patella
- Key Discriminator
- Hard endpoint plus malrotation/oversizing on CT
- Confirmatory Test
- CT with metal-artefact reduction (rotation, sizing)
- Typical Features
- Anterior impingement, difficulty on stairs, flexion block
- Key Discriminator
- Low Insall-Salvati ratio (under 0.8), elevated joint line
- Confirmatory Test
- Lateral radiograph (patellar height, joint-line measurement)
- Typical Features
- Allodynia, swelling, temperature/colour change, disproportionate pain
- Key Discriminator
- Pain and autonomic signs out of proportion to findings
- Confirmatory Test
- Clinical (Budapest criteria); imaging to exclude other causes
- Typical Features
- Progressive loss of ROM, palpable firmness, late presentation
- Key Discriminator
- Bone formation (often posterior capsule) limiting the arc
- Confirmatory Test
- Radiographs / CT showing ectopic bone
ROM Documentation
Standardized Measurement:
- Patient supine, knee over edge of bed
- Measure with goniometer (active and passive)
- Document separately: Flexion (0-120° normal) and Extension (0° normal, positive number = flexion contracture)
- Arc of motion = Flexion - Extension lag
Functional Thresholds:
- Extension 0-5°: Normal gait pattern
- Extension 5-10°: Mild limp, anterior knee pain
- Extension over 10°: Significant gait abnormality
- Flexion 0-90°: Severe functional limitation
- Flexion 90-110°: Moderate limitation (cannot rise from low chairs)
- Flexion over 110°: Near-normal function
Investigations
Imaging and Laboratory Protocol
Views: AP, lateral, skyline patella
Assess:
- Component position and alignment (rotation on AP/lateral)
- Joint line height (should be within 5mm of contralateral)
- Patella height (Insall-Salvati ratio under 0.8 = patella baja)
- Heterotopic ossification (posterior capsule)
- Loosening (radiolucent lines, subsidence)
Identify any correctable mechanical cause before planning MUA or revision.
Serum markers:
- ESR (over 30mm/hr concerning)
- CRP (over 10mg/L concerning at 6+ weeks post-TKA)
- WBC (usually normal even in infection)
Synovial fluid analysis (if elevated ESR/CRP or clinical suspicion):
- Cell count (over 3000 cells/μL concerning)
- PMN percentage (over 80% concerning)
- Culture (gold standard but may be negative)
- Alpha-defensin (high sensitivity for infection)
Infection must be ruled out before any manipulation or revision.
CT scan with metal artifact reduction:
- Assess component rotation (femoral and tibial)
- Identify impingement (anterior bone or soft tissue)
- Measure TKA alignment (mechanical axis)
MRI (rarely indicated):
- Soft tissue assessment if considering lysis of adhesions
- Extensor mechanism integrity
CT is most useful when planning revision for component malposition.

Management Algorithm
Non-Operative Treatment (0-6 Weeks)
Indications:
- Under 6 weeks post-TKA with slow but improving ROM
- Flexion over 70° and progressing
- No mechanical cause identified
- Patient compliant with physiotherapy
Conservative Protocol
- Multimodal analgesia (acetaminophen, NSAIDs if not contraindicated)
- Limit opioids (impair rehabilitation motivation)
- Address CRPS early if suspected
- Frequency: 5-7 sessions per week initially
- Focus: Progressive ROM (both flexion and extension)
- Modalities: Heat before stretching, ice after
- Home program: Heel slides, wall slides, prone hangs
- Goal: Gain 10-15° flexion per week
- Measure ROM weekly
- If plateau under 90° by week 6, plan MUA before week 12
- Do not continue PT indefinitely without progress
If no improvement in ROM by 6-8 weeks, conservative management has failed and intervention is indicated.
Surgical Technique: Manipulation Under Anesthesia
Pre-operative Planning
- Fracture: 1-3% risk (supracondylar femur, tibial plateau, patella)
- Recurrence: 30-40% lose some ROM gains over time
- Need for repeat: May require second MUA if first unsuccessful
- No improvement: 15-25% see no benefit
- Anesthesia risks: Standard general/spinal risks
- Need for revision: If underlying mechanical cause found
- Rule out infection: Recent CRP/ESR, consider aspiration
- Imaging review: Confirm no component malposition
- Anesthesia: General or spinal (need complete relaxation)
- Postop PT: Arrange immediate aggressive physiotherapy
- Timing: Ideal 6-12 weeks, avoid after 6 months
- Patient expectations: Discuss realistic ROM goals
MUA Step-by-Step Technique
Manipulation Steps
Patient supine on standard operating table
- Leg free draped to allow full range of motion
- Surgeon at side of operative knee
- Assistant optional (can provide counter-pressure)
- No tourniquet (want to assess vascular status)
Document baseline ROM under anesthesia
- Measure passive flexion and extension before manipulation
- Feel for hard vs soft endpoint (hard = mechanical block)
- Palpate for effusion, crepitus
- If hard mechanical block, stop and obtain imaging (may need revision)
Break extension adhesions FIRST (often overlooked)
- Place hand under heel, apply gentle extension force
- Goal: Achieve full extension (0°)
- If flexion contracture over 10°, may hear/feel "pop" as adhesions release
- Avoid hyperextension force (PCL injury risk)
Distract joint to protect components
- One hand on proximal tibia, one hand on distal femur
- Apply longitudinal traction along tibial axis
- This distracts the joint and reduces compression force on components during flexion
Gradual, controlled flexion to 120° goal
- One hand stabilizes femur, other hand on proximal tibia
- Apply steady, progressive flexion force
- Increase flexion in 10-15° increments
- Listen for crepitus or "pop" as adhesions break
- Goal: 120° flexion minimum
- Avoid: Sudden jerking movements (fracture risk)
Document final ROM and stability
- Measure maximum passive flexion achieved
- Cycle through ROM several times
- Check MCL/LCL stability (laxity after aggressive manipulation)
- Examine for crepitus (component damage)
- Palpate for effusion or hematoma
The entire procedure takes 5-10 minutes - gentle progressive force is safer than aggressive single manipulation.
Highest risk patients:
- Osteoporosis (T-score under -2.5)
- Long-stemmed revision components
- Over 6 months post-TKA (mature bone ingrowth)
- Rheumatoid arthritis (poor bone quality)
Fracture types:
- Supracondylar femur fracture (most common)
- Tibial plateau fracture
- Patellar fracture
If fracture suspected: Obtain immediate post-MUA radiographs before patient awakens. If fracture identified, proceed directly to fixation.
Prevention: Gentle progressive force, avoid manipulation after 6 months, pre-screen with DEXA in high-risk patients.
FLEX-ITMUA Technique Steps
Hook:FLEX-IT describes the systematic approach to manipulation - extension first, then progressive flexion with traction!
Complications
- Incidence
- 1-3% overall, 5-10% after 6 months
- Risk Factors
- Osteoporosis, late manipulation, excessive force
- Management
- ORIF with locking plate, may need revision to long stem
- Incidence
- 30-40% lose some ROM over time
- Risk Factors
- Poor PT compliance, mechanical cause unaddressed
- Management
- Repeat MUA if within 6 months, revision if mechanical
- Incidence
- 5-10% significant bleeding
- Risk Factors
- Anticoagulation, aggressive force
- Management
- Ice, compression, aspiration if tense
- Incidence
- Under 1% with proper technique
- Risk Factors
- Excessive varus/valgus stress during manipulation
- Management
- Bracing, may require ligament reconstruction
- Incidence
- 15-25% see minimal ROM gain
- Risk Factors
- Mechanical cause, mature adhesions (over 12 weeks)
- Management
- Consider arthroscopic lysis or revision
- Incidence
- Under 1% (similar to primary TKA)
- Risk Factors
- Hematoma, wound compromise
- Management
- Aspiration, antibiotics, possible I&D
If first MUA unsuccessful (under 10° gain or ROM lost within 2 weeks):
Options:
- Repeat MUA within 2 weeks (success rate 50-60%)
- Arthroscopic lysis at 3-6 months (if no mechanical cause)
- Revision TKA if mechanical cause identified
- Accept limitation if flexion over 90° and patient satisfied
Do NOT: Continue indefinite physiotherapy without progress or repeatedly manipulate after 2 attempts (diminishing returns and increasing fracture risk).
Postoperative Care and Rehabilitation
Immediate Post-Manipulation Care
MUA Postoperative Rehabilitation
Goals: Control pain and swelling, protect ROM achieved
- Multimodal analgesia (acetaminophen, NSAIDs, consider regional block)
- Cryotherapy 20 minutes every 2 hours
- CPM machine 6-8 hours/day (controversial benefit but may help pain)
- Elevation when at rest
- Document ROM within 24 hours (measure with goniometer)
- Weight-bearing as tolerated (no restriction)
Goals: Maintain ROM achieved during MUA, begin active exercises
- Physiotherapy twice daily (inpatient or home-based)
- Active assisted ROM exercises (heel slides, wall slides)
- Passive stretching by therapist
- Quadriceps sets and ankle pumps
- Goal: Maintain within 5-10° of post-MUA ROM
- Daily ROM documentation by PT
- Ice after each PT session
Goals: Maintain ROM, progress to functional activities
- PT 5-7 sessions per week (critical period)
- Home exercise program 3x/day (heel slides, prone hangs, wall slides)
- Progressive resistance exercises (quad strengthening)
- Functional activities (stairs, transfers)
- Monitor ROM weekly - should maintain or improve slightly
- If plateau or loss over 10°: Consider repeat MUA within 2 weeks
Goals: Return to normal activities, accept gradual ROM loss
- PT 3-4 sessions per week
- Progress to ADL simulation (car transfers, prolonged sitting)
- Continue home exercises daily
- Expected: Gradual 5-10° flexion loss from peak (acceptable)
- Monthly ROM documentation
- Return to driving when flexion over 90° and comfortable
Goals: Maintain functional ROM, monitor for late loss
- PT as needed for maintenance
- Home exercise program 3-4x/week indefinitely
- Monitor for red flags: Sudden ROM loss (infection, component issue)
- Accept gradual loss if ROM remains over 90° (functional threshold)
- Annual follow-up with ROM documentation
Critical Success Factors:
- Immediate aggressive PT (cannot wait 1-2 weeks)
- Patient compliance with home exercises (5-7x/week minimum)
- Weekly monitoring for early detection of ROM loss
- Low threshold for repeat MUA if significant loss within 2 weeks
ROM gains are lost without aggressive postoperative physiotherapy - this is as important as the manipulation itself.
Without aggressive PT, MUA gains are lost:
- 40-50% of patients lose all ROM gains within 6 weeks if poor PT compliance
- Home exercises 3x/day minimum are as important as formal PT sessions
- Patient must understand that passive therapy alone is insufficient - active patient participation required
- Consider psychological barriers to compliance (depression, low motivation, pain catastrophizing)
Surgeon responsibilities:
- Arrange PT before discharge (immediate start critical)
- Weekly ROM monitoring by surgeon or PT for first 6 weeks
- Low threshold to intervene if ROM plateau or loss
- Patient education about importance of exercises (cannot be passive recipient of care)
Outcomes and Prognosis
Predictors of Outcome
- Good Prognosis
- 6-12 weeks post-TKA (75-85% success)
- Poor Prognosis
- Over 12 weeks (50% success) or over 6 months (under 30%)
- Good Prognosis
- Over 70° before MUA (better baseline)
- Poor Prognosis
- Under 70° (likely mechanical cause)
- Good Prognosis
- Primary arthrofibrosis (idiopathic)
- Poor Prognosis
- Mechanical malposition (requires revision)
- Good Prognosis
- Aggressive PT 5-7x/week
- Poor Prognosis
- Poor PT compliance (ROM loss)
- Good Prognosis
- Primary TKA only
- Poor Prognosis
- Multiple prior surgeries (more scar)
After successful MUA:
- Immediate post-MUA: Average 120° flexion achieved
- 6 weeks: Typically maintain 110-115° (expect 5-10° loss)
- 3 months: Stabilize at 105-110° flexion
- 1 year: 60-70% maintain ROM within 10° of post-MUA flexion
- 2 years: 30-40% experience further ROM loss (usually still functional over 90°)
Key message: Some ROM loss over time is expected but most patients maintain functional ROM (over 90°) if initial MUA successful.
Quality of Life Impact
With flexion over 90° (successful treatment):
- Independent ADLs restored
- Stair climbing possible
- Return to driving
- Patient satisfaction 70-80%
With persistent flexion under 90°:
- Significant ADL limitations
- Requires assistive devices
- Cannot drive safely
- Patient dissatisfaction 60-70%
- Absolute ROM: Flexion over 90° critical threshold
- Improvement: Gain of 20°+ perceived as meaningful
- Pain relief: Reduction in anterior knee pain
- Expectations: Realistic preoperative counseling important
- Function: Ability to perform desired activities
Patients value functional improvement over absolute ROM numbers.
Guidelines, Registries & Global Practice
Global Epidemiology
- Stiffness needing intervention: ~1-5% of primary TKAs; a single-centre European series reported a 4.5% MUA rate (Ipach 2011)
- After revision TKA: ~1.7% require MUA, most within 3 months (Dowdle 2017, US database of 5,414 revisions)
- Strongest patient predictors: low pre-operative ROM, younger age, previous knee surgery, inflammatory arthritis
- Stiffness is a leading cause of dissatisfaction despite a technically sound implant, and a recognised but uncommon revision indication worldwide
- No single agreed numeric definition; commonly flexion under 90° and/or a flexion contracture over 10° with functional limitation
- Functional thresholds are broadly consistent across guidelines: ~83° to descend stairs, ~90-95° to rise from a chair
- Reported incidence depends heavily on the threshold and the denominator (primary vs revision), explaining the wide 1-5% range
Guidance and Consensus, Side by Side
- Position on Stiffness & MUA
- Emphasises optimal component positioning, gap balancing and early structured rehabilitation; MUA reserved for failure of supervised therapy, ideally early.
- Evidence Level
- Mostly Level III-IV (expert/registry-informed)
- Position on Stiffness & MUA
- Supports structured post-TKA rehabilitation; reserves manipulation/surgery for persistent functional restriction after physiotherapy. No routine CPM.
- Evidence Level
- Guideline-level, low-moderate underlying evidence
- Position on Stiffness & MUA
- Routine CPM not justified - no clinically important effect on ROM, pain or function (RCT meta-analysis).
- Evidence Level
- Level I (24 RCTs)
- Position on Stiffness & MUA
- Low threshold for MUA within 12 weeks; markedly better flexion gain and Knee Society scores than late MUA.
- Evidence Level
- Level III
- Position on Stiffness & MUA
- Track stiffness/arthrofibrosis as a discrete revision indication; outcomes better than revision for infection or instability when a mechanical cause is corrected.
- Evidence Level
- Registry (Level III)
Registry Evidence
- AOANJRR (Australia), NJR (England & Wales), AJRR (USA) all record stiffness/arthrofibrosis as a distinct, relatively uncommon reason for revision (typically a single-digit percentage of all TKA revisions)
- Peak timing for stiffness-related revision is within the first 6-12 months after the primary
- Re-revision burden is lower for stiffness than for infection or instability
- Registries cannot capture MUA or arthroscopic lysis (non-revision procedures), so they underestimate the true stiffness burden
- Most stiffness is managed without revision - physiotherapy, then MUA, then arthroscopic lysis
- Revision gives good results only when a correctable mechanical cause is identified (malrotation, oversizing, joint-line elevation, patella baja)
- Counsel patients that registry-defined "revision for stiffness" represents the severe end of a much larger spectrum
Key documentation requirements:
Preoperative consent (primary TKA):
- Discuss stiffness risk (1-5% require intervention)
- Document preoperative ROM (low preop ROM predicts postop stiffness)
- Set realistic expectations for ROM improvement
Postoperative management:
- Document ROM at each visit (objective measure)
- Document physiotherapy compliance and progress
- If ROM not improving by 6 weeks, document discussion of MUA option
MUA consent:
- Fracture risk (1-3%, higher if osteoporotic or over 6 months)
- Recurrence risk (30-40% lose some ROM over time)
- Need for repeat MUA or revision if unsuccessful
- Aggressive PT requirement postoperatively
Common litigation issues:
- Delayed recognition of stiffness (waiting too long past 12-week optimal window)
- Component malposition not identified before MUA (should obtain imaging)
- Fracture during MUA in high-risk patient (should screen for osteoporosis)
- Inadequate postoperative physiotherapy arrangement (ROM gains lost)
Defensive strategies:
- Image all stiff knees before MUA (rule out mechanical cause)
- Document ROM objectively with goniometer at each visit
- Discuss MUA early if ROM plateaus under 90° before 12 weeks
- Obtain DEXA in high-risk patients before MUA after 3 months
Global Practice Variation
Where management genuinely differs by region or resource setting:
- CPM use: still common in some North American and parts of European practice despite Level I evidence (Harvey 2014) showing no clinically important benefit; many UK and Australasian units have abandoned routine CPM. The world standard is early active mobilisation and structured physiotherapy.
- Rehabilitation intensity and access: high-resource systems offer frequent supervised physiotherapy, lowering the threshold for early MUA within the 12-week window; in limited-resource settings, home-based or less frequent therapy delays recognition, so stiffness may present later and beyond the optimal MUA window.
- Timing thresholds: most groups favour MUA within 12 weeks (Issa 2014), but some retain a benefit window out to ~6 months before moving to arthroscopic lysis/open arthrolysis (Fitzsimmons 2010), reflecting genuine uncertainty at the margins.
- Referral and follow-up cadence (a sensible global default): physiotherapy review at ~2, 6 and 12 weeks; surgeon review at 6 weeks if flexion under 90°; arrange MUA promptly when indicated within the optimal window; cross-sectional imaging (CT) if a mechanical cause is suspected.
MCQ Practice Points
Q: What is the optimal timing window for manipulation under anesthesia after TKA? A: 6-12 weeks post-TKA. Success rate is highest (75-85%) in this window because adhesions are forming but collagen has not yet matured and cross-linked. After 12 weeks, success drops to 50% or lower. After 6 months, fracture risk increases significantly (5-10%) due to mature bone ingrowth around components.
Q: Which intraoperative technical factor is most commonly associated with postoperative TKA stiffness? A: Femoral component oversizing. Oversizing the femoral component overstuffs the patellofemoral joint, increases patella contact stress, and mechanically limits flexion. This is preventable by templating preoperatively and sizing down if between sizes. Other mechanical factors include internal rotation (femoral or tibial), elevated joint line, and tight flexion gap.
Q: What is the minimum flexion required for activities of daily living, and why is this threshold clinically important? A: 90° flexion. This threshold allows stair climbing (83° required for descent), rising from standard chair (95° ideal but 90° minimum), and entering/exiting vehicles. Flexion under 90° causes significant functional disability and is the definition of TKA stiffness requiring intervention. Extension to 0° is also critical for normal gait.
Q: What is the most serious complication of manipulation under anesthesia after TKA, and what factors increase this risk? A: Supracondylar femur fracture (1-3% overall incidence). Risk factors include osteoporosis (T-score under -2.5), manipulation after 6 months post-TKA (mature bone ingrowth makes fracture more likely), long-stemmed revision components (stress riser), and excessive force. Prevention includes gentle progressive manipulation, pre-screening with DEXA in high-risk patients, and avoiding manipulation after 6 months.
Q: A patient has flexion of 70° at 4 months post-TKA despite two MUAs. Radiographs show proper component alignment. What is the next step in management? A: Arthroscopic lysis of adhesions. At 4 months, the patient is in the 3-6 month window where arthroscopic lysis has better outcomes than open revision TKA. Two failed MUAs indicate mature adhesions unlikely to respond to further manipulation. If no mechanical cause on imaging (ruled out component malposition, patella baja, overstuffing), arthroscopic débridement of suprapatellar scar and adhesion release is the next step before committing to revision surgery.
Q: What does the evidence show regarding continuous passive motion (CPM) machines for preventing TKA stiffness? A: CPM does NOT meaningfully improve final ROM, pain or function. The Cochrane review (Harvey et al, 2014; 24 RCTs, 1,445 patients) found CPM increased short-term active flexion by only about 2° - not clinically important - with no clinically important effect on pain, function or quality of life. A possible reduction in manipulation rate (control 7.2% vs CPM 1.6%) rests on very low-quality evidence. Early active mobilisation and structured physiotherapy are the priorities, and routine CPM is not justified.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman is 8 weeks post-TKA. She is compliant with physiotherapy but has plateaued at 80° flexion for the past 2 weeks. She can walk with a cane but cannot climb stairs or rise from a standard chair. Examination shows flexion 80° actively and passively, extension lag 5°, no effusion, wound healed, neurovascularly intact. What is your assessment and management?”
“Walk me through your technique for manipulation under anesthesia for this patient. What are the key steps, and what complications are you trying to avoid?”
“The same patient underwent MUA at 10 weeks with immediate postoperative flexion of 110°, but at 6-week follow-up she is back to 75° flexion despite compliant physiotherapy. CT scan shows internal rotation of the femoral component by 8° relative to the transepicondylar axis. How do you manage this now?”
Key Definitions
- Stiffness = flexion under 90° at 12 weeks post-TKA with functional limitation
- Functional threshold = 90° flexion (stair climbing, chair rising, vehicle entry)
- Extension deficit over 10° causes limping and anterior knee pain
- Incidence requiring intervention = 1-5% of all TKAs
Risk Factors (STIFF KNEE)
- S = Surgery previous (prior knee procedures increase fibrosis)
- T = Technical malposition (oversizing, internal rotation, elevated joint line)
- I = Infection active (rule out with ESR/CRP before MUA)
- F = Flexion contracture preop (strongest predictor of postop stiffness)
- F = Female gender (2-3x higher incidence than males)
MUA Timing and Technique
- Optimal window = 6-12 weeks post-TKA (75-85% success)
- Success drops to 50% after 12 weeks, under 30% after 6 months
- Technique: Extension first, then progressive flexion with traction to 120° goal
- Complications: Fracture 1-3% (supracondylar femur most common), recurrence 30-40%
- Postop aggressive PT critical to maintain ROM gains
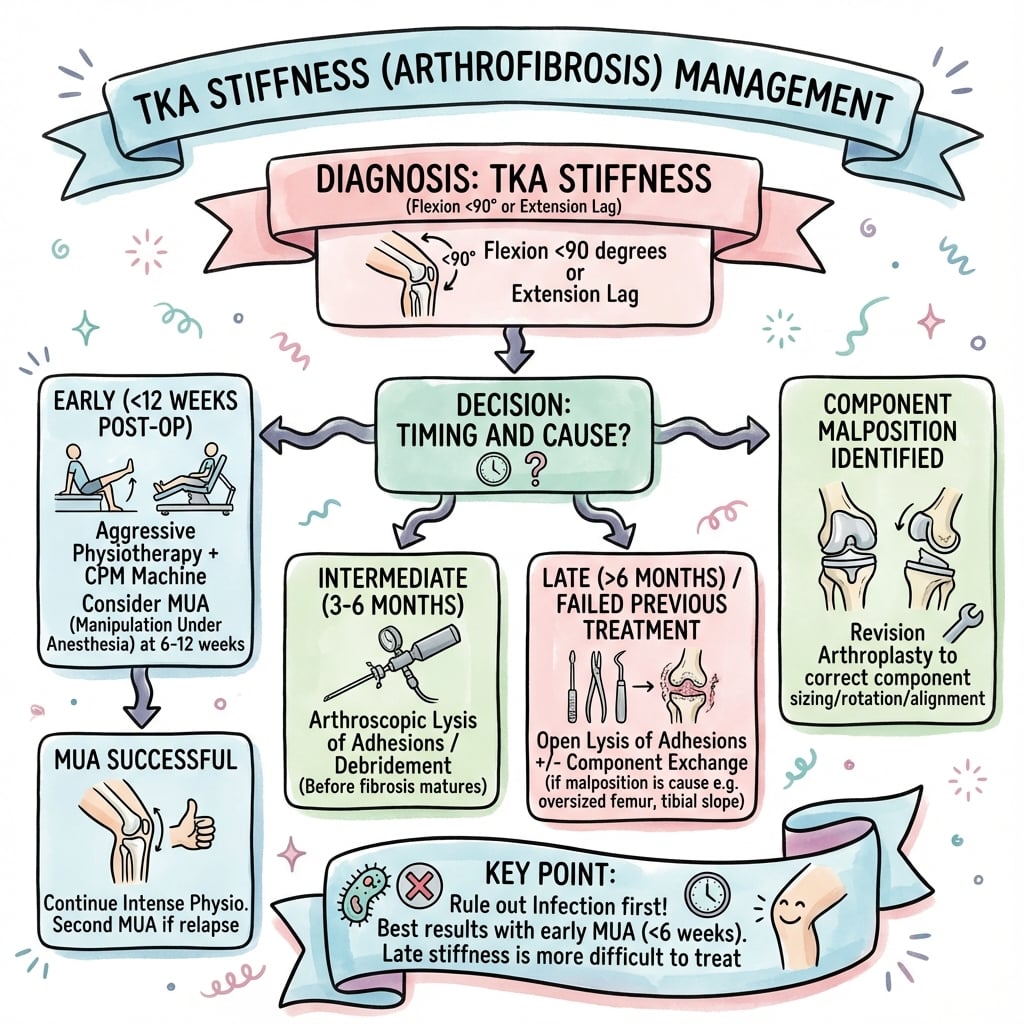
Management Algorithm
- Under 6 weeks + improving = aggressive PT, pain control, wait
- 6-12 weeks + flexion under 90° = MUA (best success window)
- 3-6 months + failed MUA = arthroscopic lysis of adhesions
- Mechanical cause identified = revision TKA to correct (not MUA)
- Always rule out infection and CRPS before attributing to arthrofibrosis
Revision Indications (REVISE)
- R = Rotate components (internal rotation over 5° significant)
- E = Extend poly (downsize if overstuffed)
- V = VMO release (vastus tethering)
- I = Impingement anterior (patella baja, femoral overhang)
- S = Size femoral component (downsize if oversized)
Evidence Base and Key Studies
Effect of Timing of Manipulation Under Anaesthesia on ROM and Functional Outcomes After TKA
- Review of 144 manipulations among 2,128 TKAs; stratified by timing (under 6 weeks, 7-12 weeks, 13-26 weeks, over 26 weeks)
- Early MUA (under 12 weeks): mean flexion gain 36.5° vs 17° for late MUA
- Early MUA: higher final ROM (119° vs 95°) and higher Knee Society objective (89 vs 84) and function (88 vs 83) scores
- No significant difference between Group I (under 6 weeks) and Group II (7-12 weeks)
- Manipulation after 26 weeks gave unsatisfactory clinical outcomes
Stiffness in Total Knee Arthroplasty
- Narrative review of the pathogenesis, risk factors and treatment of the stiff TKA
- Pre-operative range of motion identified as the most important patient risk factor
- Associations described with diabetes, reflex sympathetic dystrophy, juvenile RA and ankylosing spondylitis
- Surgery-related factors (soft-tissue imbalance, component malpositioning, incorrect sizing) cited as the most common cause
- Closed manipulation and arthrolysis give unpredictable results; revision is reserved for documented surgical error
How to Treat the Stiff Total Knee Arthroplasty? A Systematic Review
- Systematic review of 20 studies (mostly Level IV) on MUA, arthroscopy and open arthrolysis for the stiff TKA
- ROM gains after MUA and after arthroscopy (with or without MUA) are broadly similar; open arthrolysis gives inferior gains
- MUA is more successful when performed early but can still be effective when performed late
- Arthroscopy combined with MUA remains useful up to 1 year after the index TKA
- Clinically important complication rates are similar for MUA and arthroscopy
AOANJRR Registry Data: Revision for Stiffness After TKA
- Stiffness/arthrofibrosis is a discrete but relatively uncommon (single-digit percentage) indication among all TKA revisions
- Peak timing for stiffness-related revision is within the first 6-12 months after the primary TKA
- Re-revision burden after revision for stiffness is lower than after revision for infection or instability
- Revision succeeds chiefly when a correctable mechanical cause (malrotation, oversizing, joint-line elevation) is identified and addressed
Continuous Passive Motion Following Total Knee Arthroplasty in People With Arthritis (Cochrane Review)
- Meta-analysis of 24 randomised controlled trials (1,445 participants) of CPM after TKA
- Moderate-quality evidence: CPM increases short-term active flexion by only ~2° (95% CI 0 to 5) - not clinically important
- No clinically important effect on pain, function or quality of life
- Very low-quality evidence suggested CPM may reduce manipulation rate (control 7.2% vs CPM 1.6%, RR 0.3)
- Concluded CPM does not justify routine use after TKA
Arthrofibrosis After TKA: Influence Factors on Absolute Flexion and Gain After Manipulation Under Anaesthesia
- Retrospective study; 39 of 858 TKAs (prevalence of stiffness requiring MUA 4.5%) underwent MUA
- Statistically significant improvement in flexion both immediately and at 6 weeks after MUA
- Two or more previous operations before TKA predicted significantly worse absolute flexion and gain at 6 weeks
- Knees with pre-MUA flexion below 70° had worse absolute flexion but the largest gain in flexion
- Timing of MUA (over vs under 30 days) did not significantly affect absolute flexion or gain in this cohort
Risk Factors for the Development of Stiffness After Revision Total Knee Arthroplasty
- Large multicentre database study of 5,414 revision TKAs (Humana, 2007-2015)
- 1.7% (96 patients) underwent MUA after revision TKA
- 69% of post-revision manipulations occurred within the first 3 months
- Patients under 50 years had ~6.5x higher odds of requiring MUA after revision TKA
- Sex, obesity, diabetes, anxiety/depression, prior narcotic use and smoking did not increase MUA risk