Tonnis Grade of Hip Osteoarthritis
- Reading the film, not the patient. The Tonnis grade describes the radiograph — symptoms correlate poorly, especially at grades 0–1 (a grade-1 hip can be severely symptomatic from a labral tear / FAI). Always correlate with symptoms, MRI and demand.
- Grading on a supine film. Use a weight-bearing AP pelvis — a supine film underestimates joint-space narrowing and under-grades severity.
- Calling definite narrowing 'grade 1'. Grade 1 is doubtful/minimal; definite sclerosis + narrowing (space under ~2 mm) is grade 2 — and grade ≥2 is the threshold for radiographic OA.
- Missing the pattern. Primary OA narrows superolaterally/eccentrically (earliest sign); medial/concentric narrowing raises inflammatory arthropathy, protrusio or chondrocalcinosis.
- Forgetting the dysplasia companion. Pair the grade with the lateral centre-edge angle (Wiberg) — a grade-2 hip with LCEA under 20° follows a PAO pathway, not straight to replacement.
- Over-trusting the number at boundaries. Inter-observer reliability is only fair-to-moderate (worst at the 1/2 boundary) — be cautious where the grade changes the treatment.
The Tonnis grading system
Each hip is graded 0, 1, 2, or 3 on a standardised AP pelvis radiograph by assessing four radiographic parameters. The highest applicable grade is assigned.
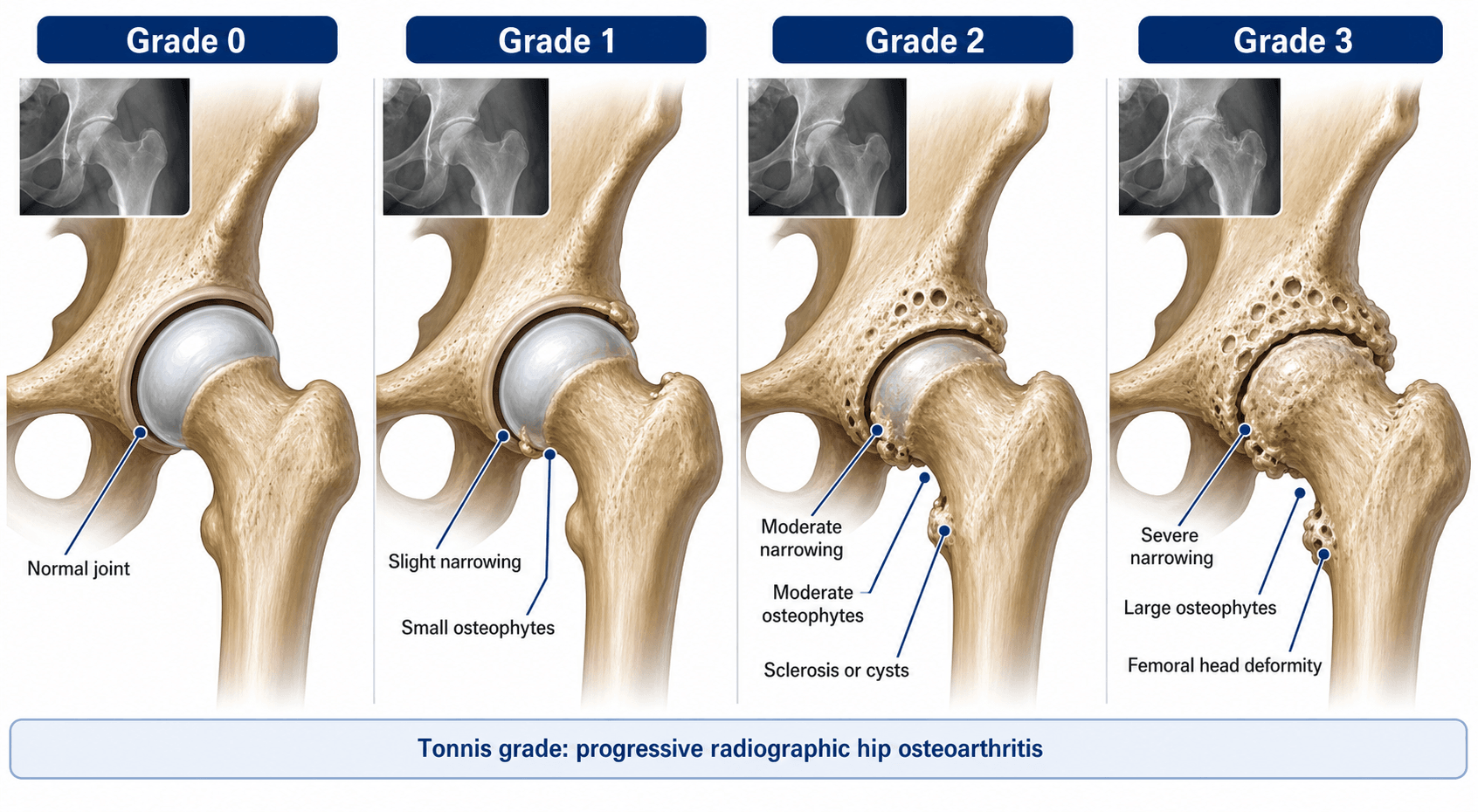

- Grade 0 (Normal)
- None
- Grade 1 (Doubtful)
- Possible slight sclerosis
- Grade 2 (Moderate OA)
- Definite sclerosis of femoral head or acetabulum (or both)
- Grade 3 (Severe OA)
- Marked sclerosis, broad zone
- Grade 0 (Normal)
- Normal (2 mm or greater superiorly)
- Grade 1 (Doubtful)
- Possible slight narrowing
- Grade 2 (Moderate OA)
- Definite narrowing, less than the normal minimum
- Grade 3 (Severe OA)
- Severe narrowing, near obliteration
- Grade 0 (Normal)
- None
- Grade 1 (Doubtful)
- None
- Grade 2 (Moderate OA)
- Possible small cysts
- Grade 3 (Severe OA)
- Definite large subchondral cysts
- Grade 0 (Normal)
- Spherical, normal contour
- Grade 1 (Doubtful)
- Normal contour
- Grade 2 (Moderate OA)
- Possible slight flattening or oval deformation
- Grade 3 (Severe OA)
- Definite flattening, mushroom deformity, or large osteophytes
Grade each hip independently on a weight-bearing AP pelvis radiograph centred over the symphysis pubis, and compare with the contralateral side. Use the strictest parameter that applies: if sclerosis is grade 3 but narrowing is grade 2, the hip is grade 3.
The superior joint space of a normal adult hip measures at least 2 mm on an AP radiograph, taken at the narrowest point of the superolateral weight-bearing zone. A space under 2 mm constitutes definite narrowing (Tonnis grade 2 or higher).
Primary hip OA is typically superolateral and eccentric, and narrowing appears here first — it is the single most sensitive early radiographic sign, so always state the pattern when you grade. Medial or concentric narrowing instead raises differentials: inflammatory arthropathy, protrusio acetabuli, or chondrocalcinosis.
Grade interpretation & clinical decision-making
- 1Grade on a weight-bearing AP pelvisAssign 0–3 by the strictest of the four parameters; note the narrowing pattern (superolateral vs medial/concentric) and the lateral centre-edge angle for dysplasia.
- 2Grade 0–1 → preserveNon-operative management; offer joint-preserving surgery (PAO for dysplasia, arthroscopy/osteochondroplasty for impingement) only if there is a correctable mechanical problem driving symptoms.
- 3Grade 2 → personaliseThe decision zone. Joint preservation is still reasonable in young, motivated patients with good range and correctable deformity; replacement becomes reasonable in older/lower-demand patients.
- 4Grade 3 → replaceTotal hip arthroplasty is the standard and most reliable option; joint-preserving surgery has essentially no role at end-stage.
- Radiographic meaning
- No OA features
- Non-operative options
- Lifestyle/activity modification, analgesia as needed
- Joint-preserving surgery
- Not applicable
- Replacement
- Not indicated
- Radiographic meaning
- Doubtful/minimal — does not meet radiographic OA criteria
- Non-operative options
- Weight loss, physiotherapy, analgesia, activity modification
- Joint-preserving surgery
- Consider for associated pathology (impingement, dysplasia) if symptoms warrant
- Replacement
- Not indicated
- Radiographic meaning
- Definite radiographic OA — moderate
- Non-operative options
- Still first-line in older or low-demand patients
- Joint-preserving surgery
- PAO (if dysplasia), arthroscopy (impingement with limited OA), surgical dislocation/osteochondroplasty in selected younger patients
- Replacement
- THA if joint-preserving surgery is unsuitable/failed; reasonable over ~55–60 with significant symptoms
- Radiographic meaning
- Advanced — end-stage
- Non-operative options
- For patients unfit for or declining surgery
- Joint-preserving surgery
- Very limited role (e.g. very young patient declining replacement, prohibitive comorbidity)
- Replacement
- Total hip arthroplasty is the standard — the most predictable, durable option
The Tonnis grade describes the radiograph, not the patient. Symptomatic hip pain correlates poorly with radiographic grade, especially at grades 0–1 — patients with minimal radiographic change can have severe symptoms from labral pathology, femoroacetabular impingement, or chondral damage not yet visible on plain film. Always correlate the grade with the clinical picture, MRI findings, and the patient's functional demands before deciding on surgery.
The topic keeps noting that a grade-0/1 hip can be severely symptomatic from FAI or a labral tear — here are the bony measures that find it:
- Cam FAI (an aspherical head–neck junction): the alpha angle — measured on a lateral view (cross-table lateral or Dunn 45°/90°) between the femoral neck axis and the point where the head–neck contour exits a best-fit circle of the head; abnormal over ~55 to 60°; look also for a reduced head–neck offset / "pistol-grip" deformity on the AP.
- Pincer FAI / acetabular retroversion (focal over-coverage): the triad of the crossover sign (the anterior wall line crosses the posterior wall line proximally), the posterior-wall sign (the posterior wall lies medial to the head centre), and the prominent ischial-spine sign; coxa profunda/protrusio indicates global over-coverage.
- So a near-normal Tönnis hip can still be disabling — image the labrum and cartilage on MRI and measure the bony morphology before attributing pain to "early OA".
Limitations & modern context
- Plain radiograph is a surrogate for cartilage loss. The Tonnis grade measures the bone reaction to cartilage depletion, not the cartilage itself; early OA may have significant chondral damage that is radiographically silent (MRI with dGEMRIC/T2 mapping detects this but is not used for grading).
- Inter-observer agreement is only fair-to-moderate. Reported inter-observer kappa ranges from fair (~0.30 among hip-preservation surgeons) to moderate (~0.59), with the greatest disagreement at the grade 1/2 boundary; intra-observer agreement is higher. Reliability is good enough for use but should temper treatment decisions made at grade boundaries.
- It does not capture symptoms or function. Read the grade alongside the pain pattern, range of motion and functional limitation — a grade-1 hip can be devastatingly symptomatic from a labral tear or impingement.
- The lateral centre-edge angle of Wiberg is a companion measurement in dysplasia: a grade-2 hip with an LCEA under 20° has a different pathway (periacetabular osteotomy) than a grade-2 hip with a normal LCEA.
- Alternative systems exist. Kellgren–Lawrence is more common in knee OA and large epidemiological studies; the Croft grade and minimum-joint-space-width criteria are used in some hip epidemiology; Tonnis is the standard in adult hip reconstruction and joint-preserving literature.
- Weight-bearing radiographs are essential — a supine film underestimates joint-space narrowing and may under-grade severity. The false-profile (Lequesne) view adds anterior coverage information but does not replace the AP grading view.

Beware the eponym: "Tönnis" names both this OA grade and the Tönnis angle — a different, equally examinable measurement.
- The Tönnis angle (the acetabular index of the weight-bearing zone / acetabular roof obliquity) is the inclination of the acetabular sourcil (weight-bearing zone): drawn between a horizontal reference and a line from the medial to the lateral edge of the sourcil.
- Normal ~0 to 10°. An increased angle (over ~10°, a steep/oblique roof) = acetabular under-coverage / dysplasia; a negative angle (a flat or down-sloping roof) = over-coverage / pincer / acetabular retroversion.
- Read it with the LCEA: both quantify superolateral coverage, and together they place a dysplastic hip (PAO) or a pincer hip (rim trim) on the right pathway rather than straight to replacement — exactly the companion role this section gives the LCEA.
Viva practice
Exam viva
Practise clinical reasoning and management decisions out loud
“A 34-year-old woman presents with a two-year history of right groin pain exacerbated by running and prolonged sitting. Her AP pelvis radiograph shows definite superior joint-space narrowing of the right hip to approximately 1.5 mm, definite subchondral sclerosis, no cysts, and a normal femoral head contour. The lateral centre-edge angle is 18 degrees. What is the Tonnis grade and how would you manage her?”
“A 58-year-old man with a 10-year history of left hip pain presents with worsening symptoms despite physiotherapy and analgesia. AP pelvis radiograph shows marked superolateral joint-space narrowing with near obliteration, severe subchondral sclerosis of both the femoral head and acetabulum, multiple subchondral cysts, and a flattened femoral head with superior osteophyte formation. The right hip has normal joint space and no sclerosis. What is the grade, what type of OA pattern is this, and what are your surgical options?”
Exam cheat sheet
SSCCThe four parameters
Hook:Sclerosis, Space, Cysts, Contour — the four features that define each Tonnis grade.
0–1–2–3The grade thresholds & what they decide
Hook:0–1 Preserve, 2 Personalise, 3 Replace. Grade ≥2 = radiographic OA.
- Four parameters (sclerosis, narrowing, cysts, contour) graded 0–3 on a weight-bearing AP pelvis; assign by the strictest parameter.
- Grade ≥2 = radiographic hip OA; grade 1 is doubtful/minimal.
- Superolateral narrowing is the earliest sign — state the pattern; medial/concentric raises other differentials.
- 0–1 preserve, 2 personalise, 3 replace — but correlate with symptoms, MRI, age, demand and the LCEA.
- Reliability is only fair-to-moderate, worst at the grade 1/2 boundary — be cautious where the grade changes the treatment.
- The grade describes the radiograph, not the patient.
The four parameters (AP pelvis, weight-bearing)
- Subchondral sclerosis: none (0) → marked broad zone (3)
- Joint-space narrowing: normal ≥2 mm (0) → near obliteration (3)
- Subchondral cysts: none (0/1) → definite large cysts (3)
- Femoral head contour: normal (0/1) → flattening + osteophytes (3)
Clinical decision thresholds
- Grade 0–1: non-operative; joint-preserving surgery only for associated pathology (impingement, dysplasia)
- Grade 2: decision zone — preserve in young selected patients, replace in older
- Grade 3: total hip arthroplasty is the standard — joint preservation has no reliable role
- Always correlate the grade with symptoms, function, MRI and patient demands
Key exam points
- Grade ≥2 defines radiographic hip OA
- Superolateral narrowing is the earliest, most sensitive sign — state the pattern
- Preoperative OA grade predicts joint-preserving (PAO) survival — higher grade, worse outcome
- Weight-bearing AP pelvis is mandatory — supine films under-grade severity
- Inter-observer reliability only fair-to-moderate; pair the grade with the lateral centre-edge angle in dysplasia
Evidence Base
Defining osteoarthritis of the hip for epidemiologic studies
- Compared seven radiologic indices of hip OA in 1315 British men aged 60–75 to find the best epidemiological definition.
- Minimal joint space (the shortest femoral-head-to-acetabulum distance) was the index most strongly associated with other OA features and, with measures of joint space generally, the most reproducible.
- The overall qualitative grade, minimal joint space and subchondral sclerosis were the indices most predictive of hip pain.
The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip
- Multicentre development of ACR classification criteria for hip OA from 201 patients with hip pain.
- The combined clinical + radiographic criteria — hip pain plus at least two of: osteophytes, joint-space narrowing, and ESR under 20 mm/hr — gave 89% sensitivity and 91% specificity.
- The radiographic presence of osteophytes best separated OA patients from those with hip pain of other causes.
The reliability of the Tönnis grading system in patients undergoing hip preservation
- Eight experienced hip-preservation surgeons graded 100 radiographs (50 patients) on two occasions.
- Tönnis inter-observer reliability was only FAIR (kappa 0.30); intra-observer reliability was moderate (kappa 0.55). Subchondral cysts were the most reliable individual feature.
- Given the limited inter-observer reliability, the authors caution against using the Tönnis grade to dictate treatment algorithms.
Radiographic evaluation of the hip has limited reliability
- Six hip specialists performed a blinded review of 77 hips (control, dysplasia, FAI) for standard radiographic parameters.
- Inter-observer reliability was highest for acetabular inclination (kappa 0.61) and Tönnis OA grade (kappa 0.59); most other parameters and the radiographic diagnosis itself had kappa under 0.55.
- Many standard radiographic parameters used to diagnose dysplasia/FAI are not reproducible, so clearer definitions are needed.
According to PubMed, the minimum-joint-space epidemiological criterion comes from Croft et al. 1990 (DOI), the ACR radiographic classification from Altman et al. 1991 (DOI), and the reliability data from Pullen et al. 2023 (DOI; inter-observer kappa 0.30) and Clohisy et al. 2009 (DOI; Tönnis kappa 0.59). The four-parameter grade definitions and the joint-preserving-vs-replacement thresholds are standard hip-reconstruction teaching.