Patient Selection | Pain and Disability | Failed Conservative Treatment | Quality of Life
- Pain and disability refractory to conservative management is the primary indication
- Radiographic severity alone does not determine need for THA - symptoms drive decision
- 6 months of conservative treatment (physio, analgesia, weight loss) should be trialled first
- Active infection is an absolute contraindication - must be eradicated first
- AOANJRR data shows 95% survivorship at 15 years for modern THA implants
- “Indication = pain + disability + radiographic OA + failed conservative Rx
- “Beware young patients (under 50) - higher revision burden, consider alternatives
- “AVN: Stage III-IV (collapse) = THA. Stage I-II = consider hip preservation
- “DDH patients need preoperative templating and may require specialized implants
Pain + Disability + Failed Conservative. THA requires all three: (1) significant pain affecting quality of life, (2) functional disability, (3) adequate trial of non-operative management. Radiographic severity alone is not an indication.
50-80 years is optimal. Younger patients (under 50) have higher lifetime revision risk and may benefit from hip preservation surgery. Older patients (over 80) have higher perioperative risk but excellent implant survival if they survive surgery.
Active infection is absolute. Relative contraindications include: active medical comorbidities, poor bone stock, neuromuscular disease affecting function, patient unable to comply with rehabilitation, ongoing substance abuse.
"AOANJRR data mandatory. Know: (1) Over 50,000 THAs/year, (2) 95% survivorship at 15 years, (3) cemented femoral stems best in older patients, (4) bearing surface choice affects longevity. Quote registry data in viva."
- Pathology
- Early OA, mild AVN (Ficat I-II)
- Treatment
- Hip preservation (osteotomy, arthroscopy)
- Key Pearl
- Delay THA as long as possible - lifetime revision burden
- Pathology
- Symptomatic OA, failed conservative
- Treatment
- Primary THA (uncemented or hybrid)
- Key Pearl
- Optimal age group - balance of activity and longevity
- Pathology
- Symptomatic OA or fractured NOF
- Treatment
- Primary THA (cemented femoral stem)
- Key Pearl
- AOANJRR: cemented stems superior in over 75s
- Pathology
- AVN Stage III-IV with collapse
- Treatment
- THA (consider dual mobility if young)
- Key Pearl
- Core decompression fails after collapse occurs
- Pathology
- Dysplastic acetabulum, high hip center
- Treatment
- THA with specialized planning
- Key Pearl
- Preoperative templating essential, may need structural graft
MEDICALPREOPERATIVE ASSESSMENT - MEDICAL Framework
Hook:MEDICAL workup ensures patient is optimized and surgical plan is clear
REGISTRYAOANJRR KEY DATA - REGISTRY Framework
Hook:REGISTRY data from AOANJRR is essential exam knowledge for evidence-based practice
Overview and Epidemiology
Total hip arthroplasty (THA) is one of the most successful surgical procedures in modern medicine. The primary indication for THA is end-stage hip arthritis causing pain and disability that has failed conservative management.
Historical perspective:
- Sir John Charnley pioneered modern THA in the 1960s with the low-friction arthroplasty concept
- Cemented metal-on-polyethylene became the gold standard
- Evolution to modular implants, improved bearing surfaces, and minimally invasive techniques
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) established 1999 - world-leading registry
THA works because it: (1) reliably eliminates pain from arthritic hip, (2) restores function and mobility, (3) has predictable long-term outcomes with modern implants (95% survival at 15 years), (4) significantly improves quality of life. The key is patient selection - matching the right patient to the right procedure at the right time.
Epidemiology (AOANJRR 2023 data):
- Over 50,000 primary THAs performed annually (AOANJRR)
- Increasing trend due to aging population
- Bilateral THA common (10-15% of patients eventually need contralateral)
- Male:Female ratio approximately 1:1.2 (OA slightly more common in women)
- Osteoarthritis: 85-90% (primary or secondary)
- Avascular necrosis: 5-10%
- Inflammatory arthritis: 2-5% (RA, AS)
- Fracture sequelae: 2-3%
- DDH and other: 1-2%
Access Criteria: Optimise Modifiable Risk Factors, Do Not Ration
The contraindications table and the ACTIVE mnemonic list severe obesity (BMI over 40), smoking/substance use and young age among the relative contraindications - which raises the question this section must answer explicitly: are these access thresholds that disqualify a patient, or modifiable risk factors to be optimised? The modern, guideline-based answer is the latter.
Do not ration by BMI, age or smoking alone. NICE (NG226) explicitly states that access to joint replacement should not be restricted on the basis of age, sex, smoking or BMI alone; the patient should be referred when symptoms substantially affect quality of life and non-surgical care has been ineffective. Arbitrary BMI or age cut-offs are not supported by outcome evidence, deny a highly effective operation to patients who would benefit, and worsen health inequity. The absolute pain and function benefit of THA is largely preserved across BMI categories, even though the complication risk is higher.
The correct framing: optimise, then share the decision. A modifiable risk factor is a target for prehabilitation, not a reason to refuse surgery. An absolute contraindication (active infection, inability to participate in rehabilitation, prohibitive medical risk) is a different category, dealt with above.
- Why it raises risk
- Higher wound complication, infection, dislocation and medical risk
- Action - optimise, not ration
- Offer weight management and optimise comorbidities; counsel on raised but not prohibitive risk - BMI alone is not a hard cut-off
- Why it raises risk
- Impaired wound healing, higher infection and perioperative pulmonary/medical complications
- Action - optimise, not ration
- Offer smoking cessation before surgery (even a few weeks helps); support rather than refuse
- Why it raises risk
- Uncontrolled diabetes raises wound infection and systemic complications
- Action - optimise, not ration
- Optimise glycaemic control before elective THA (see patient selection)
- Why it raises risk
- Transfusion, infection and haematogenous seeding risk
- Action - optimise, not ration
- Correct anaemia, optimise nutrition, treat occult sepsis before surgery
- Why it raises risk
- Higher lifetime revision burden
- Action - optimise, not ration
- A counselling and expectation issue, and a prompt to weigh alternatives - not an absolute bar
Blanket policies that refuse THA above a fixed BMI, or above or below a fixed age, conflict with NICE guidance and with the evidence that the functional benefit of THA persists across BMI categories. A higher BMI justifies risk optimisation, counselling and vigilant perioperative care - not automatic denial. Document a shared decision rather than applying an arbitrary rule.
The high-yield distinction: active infection, inability to comply with rehabilitation, and prohibitive uncontrolled medical risk are absolute contraindications; obesity, smoking, poorly controlled diabetes and young age are modifiable or relative factors you optimise and counsel around, not access thresholds. Quoting NICE's position against rationing by age, BMI or smoking alone is a strong exam answer.
Patient Selection and Preoperative Assessment
Patient selection is the single most important determinant of THA outcome.
Ideal THA candidate:
- Age 50-80 years (optimal risk-benefit balance)
- Severe symptomatic hip arthritis (pain, disability)
- Failed adequate conservative trial (6+ months)
- Motivated patient with realistic expectations
- Able to participate in rehabilitation
- Medical comorbidities optimized
- Social support for postoperative period
Preoperative assessment:
Preoperative Workup
- History: Pain severity, functional limitation, previous treatments, medical history
- Examination: Hip ROM, leg length, gait, neurovascular, spine (fixed deformity)
- Imaging: AP pelvis, lateral hip, assess arthritis severity
- Discussion: Diagnosis, natural history, treatment options (conservative vs surgical)
- Confirm failed conservative treatment (6 months minimum)
- Patient-reported outcomes (HOOS, Oxford Hip Score) document severity
- Medical clearance: Cardiac risk assessment (RCRI), pulmonary function if indicated
- Dental clearance: Rule out infection source
- MRSA screening: Nasal swab, decolonization protocol if positive
- Templating: AP pelvis with magnification marker, template component sizes
- Consent: Risks (infection 0.5-1%, dislocation 2-3%, DVT 1-2%, revision 5% at 15 years), benefits, alternatives
- Discuss: Approach (anterior, posterior, lateral), bearing surface, fixation method
- Preoperative education: DVT prophylaxis, mobility restrictions, rehabilitation expectations
Medical optimization:
- RCRI score: Revised Cardiac Risk Index (6 predictors)
- High risk: Recent MI, CHF, CVA, DM, renal insufficiency, high-risk surgery
- Cardiology referral if RCRI greater than or equal to 2
- Beta-blockers, statins perioperatively
- Consider stress test if symptomatic
- COPD: Optimize bronchodilators, stop smoking
- OSA: CPAP compliance, perioperative monitoring
- Respiratory infection: Defer surgery until resolved
- ABG/PFTs if severe disease
- Diabetes: HbA1c under 7% ideal, under 8% acceptable
- Poor control increases infection risk 3-fold
- Anemia: Iron studies, EPO if Hb under 110 g/L
- Renal: Adjust medications, hydration protocol
HbA1c over 8% is associated with significantly higher risk of surgical site infection, wound dehiscence, and periprosthetic joint infection. Guidelines: Ideally HbA1c under 7% before elective THA. If 7-8%, counsel about higher risk. If over 8%, strongly consider delaying surgery for 3 months of glycemic optimization. Emergency surgery (fracture) - proceed with heightened vigilance.
Dental clearance:
Recent dental infection or poor dentition can lead to bacteremia and hematogenous seeding of prosthetic joint.
Protocol:
- All patients: Dental examination within 6 months of THA
- Active dental infection: Treat first, wait 6 weeks minimum
- Poor dentition, multiple caries: Consider extraction and healing before THA
- Routine dental prophylaxis: Per ADA guidelines (not routinely recommended for most patients, consider high-risk)
MRSA screening and decolonization:
MRSA Protocol
Nasal swab for MRSA colonization (PCR test, results in 24-48 hours)
Decolonization protocol:
- Mupirocin nasal ointment (TID for 5 days)
- Chlorhexidine body wash (daily for 5 days)
- Reswab to confirm eradication
If MRSA positive history: Vancomycin instead of cefazolin for prophylaxis
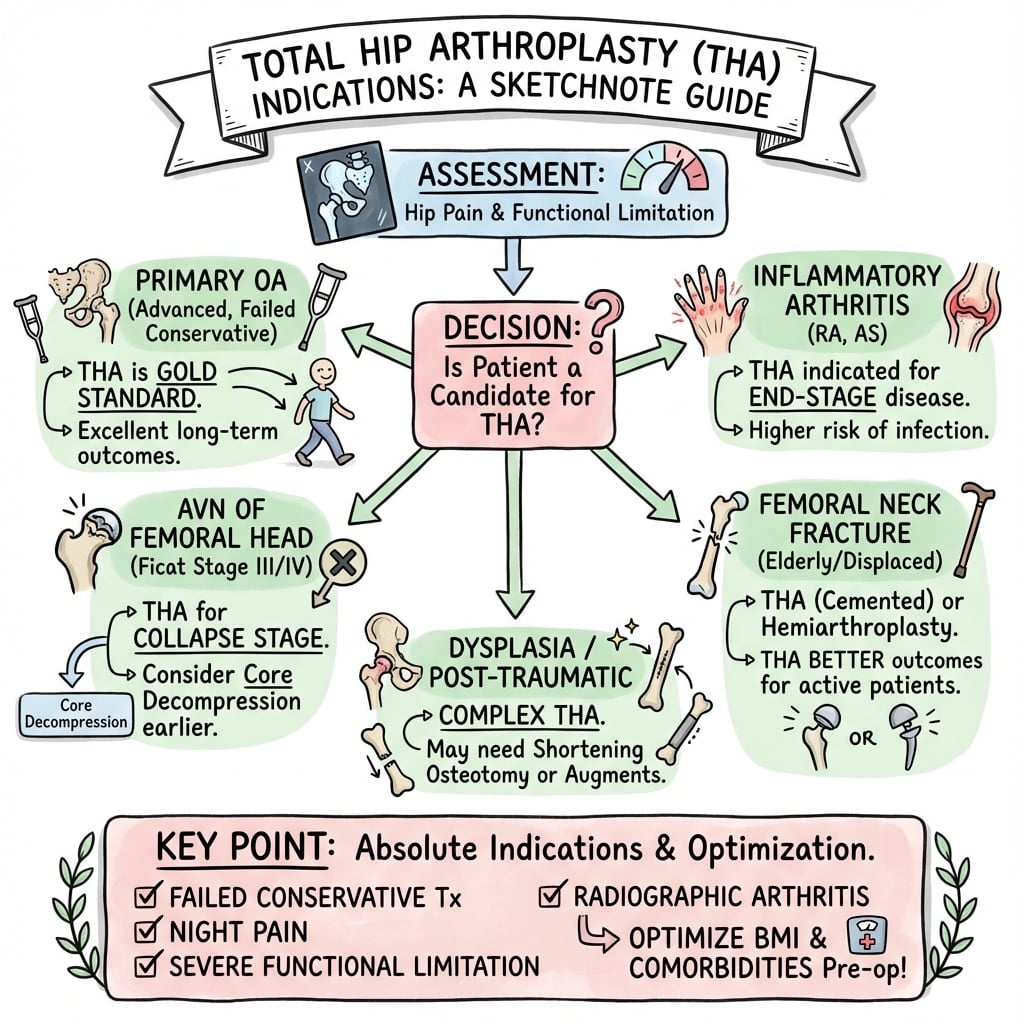
Indications for Total Hip Arthroplasty
End-stage hip arthritis causing pain and functional disability that has failed adequate conservative management.
-
Pain and Disability
- Pain that affects quality of life (sleep, ADLs, recreation)
- Functional limitation (walking distance, stairs, getting out of chair)
- Patient-reported outcome measures (HOOS, WOMAC, Oxford Hip Score) document severity
-
Radiographic Evidence
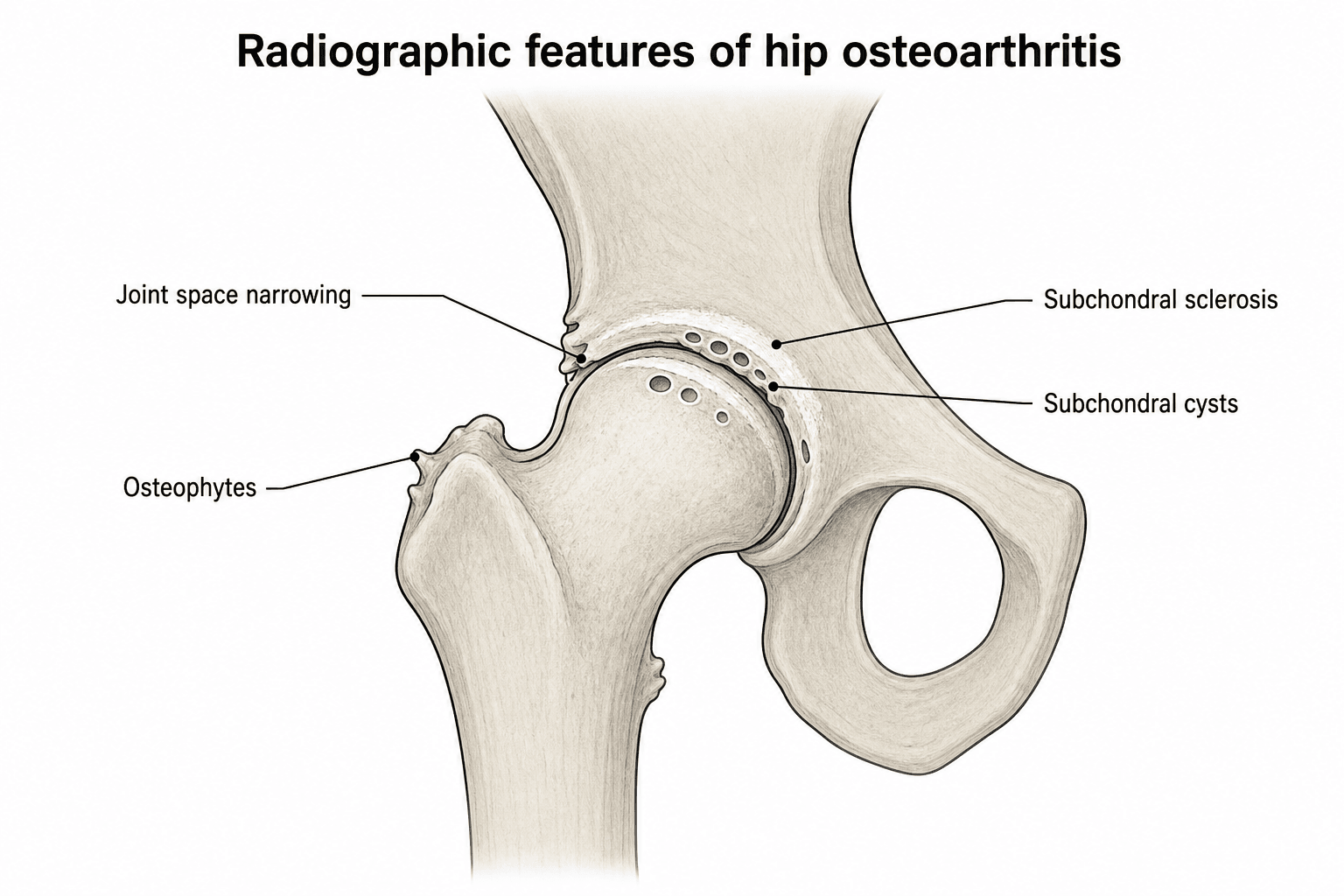
- Plain radiographs show joint space loss, osteophytes, sclerosis, cysts
- Confirms diagnosis but does NOT alone indicate need for surgery
- Severity on X-ray does not correlate perfectly with symptoms
-
Failed Conservative Treatment
- At least 6 months of appropriate non-operative management
- Includes: physiotherapy, weight loss, activity modification, analgesia (NSAIDs, paracetamol), intra-articular injection
- Patient compliance with conservative measures documented
- Severe OA with pain, disability, failed conservative (most common)
- AVN Stage III-IV with collapse and secondary OA
- Failed previous surgery (ORIF for fracture, osteotomy) with persistent pain
- Acute femoral neck fracture in elderly (hemiarthroplasty vs THA decision)
- Young patient (under 50) with severe symptoms - weigh alternatives
- Inflammatory arthritis (RA, AS) with hip involvement
- Post-traumatic arthritis after acetabular fracture, dislocation
- DDH with secondary arthritis
- Failed hip preservation (PAO, femoral osteotomy)
Primary Osteoarthritis
Most common indication (85-90% of THAs)
- Insidious onset of groin pain, may radiate to thigh/knee
- Mechanical pain (worse with activity, better with rest)
- Progressive stiffness (especially internal rotation lost first)
- Gait changes (antalgic, Trendelenburg if abductors weak)
- Joint space narrowing (weight-bearing AP pelvis)
- Osteophyte formation (femoral and acetabular)
- Subchondral sclerosis
- Subchondral cysts (geodes)
- Patient reports pain affecting sleep or ADLs
- Walking distance limited (typically under 500m)
- Failed 6 months of conservative treatment
- Patient motivated for surgery and rehabilitation
- Medical comorbidities optimized
Primary OA = idiopathic, typically over 50 years, no clear cause. Secondary OA = identifiable cause such as DDH, AVN, SCFE, Perthes, post-traumatic. Important to distinguish because secondary OA may require specialized surgical planning (e.g., DDH needs high hip center restoration).
PAINTHA INDICATIONS - PAIN Framework
Hook:PAIN = the patient needs to have PAIN that has failed conservative management
ACTIVECONTRAINDICATIONS - ACTIVE Framework
Hook:ACTIVE contraindications must be addressed before proceeding with surgery
Hip Fracture as an Indication: THA versus Hemiarthroplasty
The absolute-indications list and the AO Foundation guideline row both name the displaced intracapsular femoral neck fracture as a setting where arthroplasty is indicated and where the examiner expects a structured THA-versus-hemiarthroplasty decision. (Undisplaced fractures, younger patients suitable for fixation, and the internal-fixation construct itself are managed on the fracture pathway and are covered in the hip-fracture topics.)
Why arthroplasty rather than fixation in this group. A displaced (Garden III-IV) subcapital fracture in an older patient disrupts the retinacular blood supply to the femoral head, so internal fixation carries a high rate of avascular necrosis and nonunion with a heavy re-operation burden. Replacing the head at the index operation avoids that failure pathway, which is why displaced intracapsular fractures in the older patient are treated by arthroplasty rather than fixation.
Choosing between hemiarthroplasty and THA. The head must be replaced either way; the real question is whether to resurface the acetabulum as well.
- Favours Total Hip Arthroplasty
- Independent community ambulator, higher functional demand
- Favours Hemiarthroplasty
- Low-demand, limited household ambulation
- Favours Total Hip Arthroplasty
- Cognitively intact, can follow precautions
- Favours Hemiarthroplasty
- Cognitive impairment / dementia
- Favours Total Hip Arthroplasty
- Symptomatic acetabular OA or inflammatory arthritis already present
- Favours Hemiarthroplasty
- Normal acetabular cartilage
- Favours Total Hip Arthroplasty
- Reasonable life expectancy (time for acetabular wear to matter)
- Favours Hemiarthroplasty
- Limited life expectancy / frailty
- Favours Total Hip Arthroplasty
- Better function and pain relief, no later acetabular erosion - but higher dislocation
- Favours Hemiarthroplasty
- Faster, lower dislocation - but acetabular erosion can cause groin pain over time
In short, the fit, independent, cognitively intact older patient - especially one who already has acetabular arthritis - is the candidate for THA, which gives modestly better function and avoids the later groin pain of acetabular erosion seen when a hemiarthroplasty head articulates against native cartilage. The frail, low-demand or cognitively impaired patient is better served by hemiarthroplasty, which is quicker, carries a lower dislocation risk and is adequate for limited demand. (Unipolar versus bipolar hemiarthroplasty shows no clear functional difference - that detail belongs with the hip-fracture topics.)
Total Hip Arthroplasty or Hemiarthroplasty for Hip Fracture (HEALTH)
- 1495 independently ambulating patients aged 50 or older with a displaced femoral neck fracture, randomised THA versus hemiarthroplasty across 80 centres in 10 countries
- Secondary hip procedure within 24 months: 7.9% (THA) versus 8.3% (hemiarthroplasty) - no significant difference (hazard ratio 0.95)
- Hip instability or dislocation more common with THA: 4.7% versus 2.4%
- Function and quality of life (WOMAC) modestly favoured THA, but the difference was small and clinically unimportant over 24 months
- Mortality similar between groups (14.3% versus 13.1%)
THA performed for a fracture dislocates more often than elective THA for OA, because fracture patients lack the soft-tissue contracture and capsular thickening of a chronically arthritic hip. If you choose THA for a displaced femoral neck fracture, reduce that risk with a larger femoral head, a dual-mobility construct, and/or an approach that preserves the posterior soft tissues - the same principle examiners expect for any high-dislocation-risk THA.
Contraindications to Total Hip Arthroplasty
- Category
- Absolute
- Management
- Eradicate infection first, stage reconstruction
- Category
- Absolute
- Management
- Treat infection, may need long-term suppression before THA
- Category
- Absolute
- Management
- Defer until cardiac clearance and optimization
- Category
- Absolute
- Management
- CHF, COPD exacerbation, uncontrolled DM - optimize first
- Category
- Absolute
- Management
- Cognitive impairment, psychiatric illness precluding participation
- Category
- Relative
- Management
- Consider alternatives (osteotomy, resurfacing, delay THA if possible)
- Category
- Relative
- Management
- Higher complication risk - consider weight loss program first
- Category
- Relative
- Management
- Higher infection risk, poor compliance - address before surgery
- Category
- Relative
- Management
- May need specialized techniques (impaction grafting, long stems)
- Category
- Relative
- Management
- Assess wound healing potential, vascular surgery input
- Category
- Relative
- Management
- Higher dislocation risk - consider constrained liner, dual mobility
Active infection anywhere in the body is an absolute contraindication to elective THA. This includes: (1) local hip infection (previous septic arthritis), (2) distant infection (UTI, dental abscess, skin infection), (3) bacteremia. Why: Risk of hematogenous seeding to prosthetic joint. Management: Eradicate infection first, minimum 6 weeks antibiotics, inflammatory markers normal before proceeding.
Special contraindication scenarios:
Not absolute contraindication but need careful discussion:
- Lifetime revision risk high (50-year-old may need 2-3 revisions in lifetime)
- Activity level typically higher (increased wear, loosening risk)
- Alternatives: Hip arthroscopy, PAO, femoral osteotomy, resurfacing
- If THA necessary: hard-on-hard bearings (ceramic-on-ceramic), dual mobility
- Counsel: Revision likely, activity restrictions, long-term implications
High dislocation risk:
- Parkinson's disease (rigidity, bradykinesia, falls)
- CVA with spasticity, weakness
- Cerebral palsy, muscular dystrophy
- Mitigation strategies: Dual mobility bearing, constrained liner, large diameter heads
- Patient and family education about dislocation precautions
- Consider if benefits outweigh risks (severe pain, immobility)
Anatomy and Pathophysiology of Hip Arthritis
Normal hip joint anatomy:
- Ball-and-socket joint with excellent stability and range of motion
- Femoral head (2/3 sphere) articulates with acetabulum (horseshoe-shaped lunate surface)
- Articular cartilage 2-4mm thick, allows load distribution and low-friction movement
- Labrum deepens socket and creates suction seal
- Capsule reinforced by ligaments (iliofemoral, pubofemoral, ischiofemoral)
Pathophysiology of osteoarthritis:
Osteoarthritis is not just "wear and tear". It is an active disease process involving: (1) cartilage degradation (matrix metalloproteinases), (2) subchondral bone changes (sclerosis, cysts), (3) synovial inflammation, (4) osteophyte formation. The rate of progression is highly variable - some patients plateau, others progress rapidly.
Radiographic changes:
- Findings
- Joint space narrowing, early osteophytes
- Symptoms
- Mild pain with activity
- Management
- Conservative: weight loss, physio, analgesia
- Findings
- Definite JSN, osteophytes, sclerosis
- Symptoms
- Pain limiting activity, stiffness
- Management
- Consider injection, continue conservative
- Findings
- Bone-on-bone, large osteophytes, cysts
- Symptoms
- Constant pain, night pain, major disability
- Management
- THA if conservative failed for 6+ months
Critical concept: Radiographic severity does NOT always correlate with symptoms. Some patients have severe radiographic OA but minimal symptoms (do NOT offer surgery). Conversely, some have moderate radiographic changes but severe symptoms (may benefit from THA). Symptoms drive the decision, not X-rays alone.
Classification Systems
Tonnis Classification of Hip Osteoarthritis
- Radiographic Features
- Normal
- Clinical Correlation
- No OA
- Radiographic Features
- Sclerosis, mild JSN, osteophytes
- Clinical Correlation
- Mild symptoms, conservative Rx
- Radiographic Features
- Moderate JSN, cysts
- Clinical Correlation
- Moderate symptoms, consider injection
- Radiographic Features
- Severe JSN or bone-on-bone
- Clinical Correlation
- Severe symptoms, THA if conservative failed
Tonnis Grade 3 is the most common indication for THA when combined with failed conservative treatment.
Clinical Assessment
History and physical examination for THA candidacy
- Pain characteristics: Location (groin vs lateral), severity, progression
- Functional limitation: Walking distance, stairs, ADLs, sleep disturbance
- Previous treatments: Physio, injections, medications, duration and response
- Medical comorbidities: Cardiac, pulmonary, diabetes, immunosuppression
- Patient goals: Expectations for pain relief, function, activity level
- Gait: Antalgic, Trendelenburg (abductor weakness), leg length discrepancy
- ROM: Flexion, extension, abduction, adduction, internal/external rotation (IR lost first in OA)
- Leg length: Measure true vs apparent LLD (ASIS to medial malleolus)
- Neurovascular: Femoral/dorsalis pedis pulses, sensation, motor function
- Associated pathology: Spine (flexion deformity), knee (referred pain pattern)
- Oxford Hip Score (0-48, under 30 indicates severe impairment)
- WOMAC (Western Ontario and McMaster Universities Arthritis Index)
- HOOS (Hip disability and Osteoarthritis Outcome Score)
- SF-36 (quality of life measure)
Differential diagnosis of hip-region pain. Before attributing pain to arthritis and offering THA, confirm the pain is genuinely intra-articular hip pain and exclude mimics - a key examiner probe because operating on the wrong source of pain is a classic cause of a dissatisfied "failed" THA.
- Typical pain pattern
- Groin pain, worse on weight-bearing, internal rotation lost first
- Key discriminator
- Pain reproduced on hip ROM, especially IR/flexion
- Confirmatory test
- Weight-bearing AP pelvis: joint space loss, osteophytes
- Typical pain pattern
- Buttock/posterior thigh, below knee, worse on sitting or spinal movement
- Key discriminator
- Normal hip ROM; pain not reproduced by hip rotation
- Confirmatory test
- Spine examination, lumbar MRI; diagnostic intra-articular hip injection negative
- Typical pain pattern
- Lateral hip pain, tender over trochanter, painful lying on side
- Key discriminator
- Point tenderness laterally, pain on resisted abduction, hip joint ROM painless
- Confirmatory test
- Clinical; ultrasound/MRI shows gluteal tendinopathy or bursitis
- Typical pain pattern
- Groin pain in younger patient, catching/clicking, pain on pivoting
- Key discriminator
- Positive anterior impingement (FADIR) test, preserved joint space
- Confirmatory test
- MR arthrogram; CT for bony morphology (alpha angle)
- Typical pain pattern
- Groin pain, often steroid/alcohol history, X-ray may be normal
- Key discriminator
- Pain out of proportion to plain-film changes
- Confirmatory test
- MRI (earliest changes; double-line sign)
- Typical pain pattern
- Constant severe pain, rest and night pain, systemic features
- Key discriminator
- Fever, raised inflammatory markers, refusal to bear weight
- Confirmatory test
- ESR/CRP, joint aspiration for cell count and culture
- Typical pain pattern
- Buttock/thigh pain on walking, relieved by standing rest
- Key discriminator
- Diminished pulses, no pain on hip ROM
- Confirmatory test
- ABPI, CT/MR angiography
Investigations
- AP pelvis (standing, weight-bearing, both hips visible)
- Lateral hip (cross-table or frog-leg)
- Findings: Joint space narrowing, osteophytes, sclerosis, cysts
- Measurement: Hip center, leg length, offset
- MRI: Early AVN detection (Stage I), soft tissue pathology, occult fracture
- CT scan: DDH planning, post-traumatic deformity, bone stock assessment
- Nuclear medicine: Bone scan for infection vs loosening differentiation (rare preoperative)
- FBC: Anemia (may need preoperative iron/EPO)
- UEC: Renal function for NSAID use, perioperative hydration
- HbA1c: If diabetic (target under 8%)
- ESR/CRP: Elevated suggests infection (investigate before elective THA)
- Coagulation studies: If on anticoagulation
- ECG: All patients over 50 or with cardiac history
- Echocardiogram: If cardiac symptoms or murmur
- Pulmonary function tests: If severe COPD
- Urinalysis: Rule out UTI before elective surgery
Preoperative Planning and Templating
Templating is essential for:
- Component size prediction (reduces operative time, inventory needs)
- Leg length restoration planning
- Offset restoration (abductor moment arm)
- Identifying anatomical challenges (DDH, previous surgery, deformity)
Required radiographs:
- Standing, weight-bearing
- Both hips visible, coccyx centered
- Magnification marker (ball bearing of known size, typically 25mm or 30mm, at level of greater trochanter)
- Pelvis level (obturator foramina symmetric)
- Use to template acetabular component size and position
- Cross-table lateral or frog-leg lateral
- Assess femoral offset, canal shape
- Identify deformity (previous fracture, Paget's)
- Template femoral component size, neck cut level
Digital templating process:
Templating Steps
Measure magnification marker on X-ray, input into software to calibrate (typically 110-120% magnification)
- Mark hip center of rotation (COX point at intersection of lines)
- Mark teardrop (medial acetabular wall landmark)
- Mark lesser trochanter
- Measure preoperative leg length (from COX to ischial tuberosity or iliac crest)
- Place cup at anatomic hip center (teardrop plus 5mm medial, 25mm superior to teardrop)
- Template covers subchondral bone, avoids protrusio or overmedialization
- Note size (typically 50-58mm in adults)
- Plan inclination (40-45 degrees) and anteversion (15-20 degrees)
- Place stem in canal, fill metaphysis (press-fit) or 2mm gap (cemented)
- Match native offset (distance from center of head to center of femoral canal)
- Select neck length to restore leg length
- Note stem size (typically 10-14 for uncemented, 2-4 for cemented)
- Measure templated leg length (COX to ischial tuberosity)
- Goal: Restore native length or up to 1cm lengthening if needed for stability
- Over-lengthening (more than 1.5cm) risks nerve palsy, patient dissatisfaction
- Document planned leg length to inform intraoperative measurement
Offset restoration:
Offset (distance from center of rotation to greater trochanter) affects abductor moment arm. Leg length affects limb length equality. They are independent but related. You can have: (1) normal offset, short leg (head too small), (2) normal offset, long leg (head too large), (3) increased offset, normal leg (lateral cup position). Goal: Restore both offset and leg length to within 5mm of native or contralateral side.
Special considerations:
- DDH: High hip center, small canal, increased anteversion - may need structural graft, specialized implants
- AVN in young patient: Consider resurfacing vs THA, templating for both
- Previous surgery: Retained hardware, altered anatomy - plan hardware removal approach
- Leg length discrepancy: Preoperative LLD may be longstanding, patient adapted - discuss postoperative expectations
Alternatives and Hip Preservation
Before proceeding with THA in younger patients, consider alternatives:
- Indication
- FAI, labral tear, early OA
- Age Group
- Under 50
- Outcome
- Good short-term pain relief, may delay THA 5-10 years
- Indication
- Symptomatic DDH, no significant OA
- Age Group
- 20-40
- Outcome
- Good outcomes, delays/prevents THA in 70% at 10 years
- Indication
- Cam FAI, femoral head AVN (pre-collapse)
- Age Group
- Under 50
- Outcome
- Variable, may delay THA
- Indication
- AVN Stage I-II (pre-collapse)
- Age Group
- Any age
- Outcome
- May halt progression, does not work after collapse
- Indication
- Young male, large femoral head, no cysts
- Age Group
- Under 60
- Outcome
- Metal-on-metal concerns, AOANJRR shows higher revision than THA
Refer to hip preservation surgeon if: (1) Patient under 50 years, (2) Radiographic OA mild to moderate (joint space preserved), (3) Identifiable pathoanatomy (FAI, dysplasia), (4) Patient motivated for complex rehab. Don't refer if: Severe OA (Tonnis Grade 3), AVN with collapse, patient wants definitive solution (THA provides better pain relief than osteotomy in end-stage disease).
Hip resurfacing:
Once popular in young males, now declining in use due to:
- Metal-on-metal bearing concerns (pseudotumor, metallosis, ARMD)
- AOANJRR data shows higher revision rate than THA (especially in women)
- Requires large femoral head (over 50mm), good bone quality
- Contraindicated: Renal impairment, metal allergy, osteoporosis, cysts
Still considered in: Young male athlete, very large femoral head, strong bone, patient counseled about risks
Management Algorithm
Initial Conservative Management
All patients with hip OA should undergo trial of conservative treatment before THA:
Conservative Treatment Progression
- Education: Natural history, activity modification, weight loss
- Physiotherapy: Strengthen hip abductors, core, improve gait
- Analgesia: Paracetamol, topical NSAIDs, oral NSAIDs (if tolerated)
- Adjuncts: Walking aids (cane in opposite hand), heat/ice
- Intra-articular injection: Corticosteroid (triamcinolone 40mg)
- Duration of relief: Variable (50% get 3-6 months relief)
- PRP, hyaluronic acid: Evidence limited, Evidence limited
- Modify activities: Avoid high-impact, aggravating movements
If symptoms persist despite compliance with conservative measures → Consider THA
Criteria for surgical referral:
- Pain affecting sleep or ADLs
- Limited walking distance (under 500m)
- Patient-reported outcomes (Oxford Hip Score under 30/48)
- Patient understands risks/benefits and motivated
6 months is the generally accepted minimum duration of conservative treatment before THA. However, this is a guideline, not absolute rule. Exceptions: (1) Rapidly progressive painful AVN with collapse (may operate sooner), (2) Acute fracture in elderly (immediate surgery), (3) Patient tried conservative for years before presenting (don't need another 6 months). Use clinical judgment.
Surgical Technique Overview
Surgical Approaches for THA
- Internervous Plane
- Gluteus maximus (inferior gluteal) / Short external rotators (nerve to QF)
- Key Features
- Most common, excellent femoral exposure
- Internervous Plane
- TFL (superior gluteal) / Sartorius (femoral)
- Key Features
- Tissue-sparing, steep learning curve
- Internervous Plane
- Splits gluteus medius
- Key Features
- Stable, abductor damage risk
Complications
Complications of THA that patients must understand before consenting:
- Incidence
- 0.5-1.0% (AOANJRR)
- Prevention Strategies
- Antibiotic prophylaxis, MRSA screening, minimize operative time
- Impact on Decision
- Devastating complication requiring staged revision, prolonged antibiotics
- Incidence
- 2-3% (higher posterior approach, neuromuscular disease)
- Prevention Strategies
- Large diameter heads, dual mobility, optimal component positioning
- Impact on Decision
- Most dislocations occur in first 3 months. May need revision if recurrent
- Incidence
- 1-2% symptomatic DVT, 0.1-0.4% fatal PE
- Prevention Strategies
- Chemoprophylaxis (LMWH, apixaban), early mobilization, compression stockings
- Impact on Decision
- Major cause of perioperative mortality. Prophylaxis mandatory
- Incidence
- 0.5-2% (sciatic most common)
- Prevention Strategies
- Avoid limb lengthening over 4cm, careful retractor placement
- Impact on Decision
- Femoral nerve (anterior), sciatic (posterior/lateral). Most resolve but may be permanent
- Incidence
- 0.1-0.3%
- Prevention Strategies
- Careful cement pressurization, avoid excessive acetabular reaming medially
- Impact on Decision
- External iliac vessels at risk with anterior approach, obturator with reaming
- Incidence
- 10-15% (over 1cm)
- Prevention Strategies
- Preoperative templating, intraoperative measurement, trial reduction
- Impact on Decision
- Most common cause of patient dissatisfaction. Discuss preoperative LLD
- Incidence
- 5% at 15 years (AOANJRR)
- Prevention Strategies
- Good fixation technique, optimal implant choice, patient activity modification
- Impact on Decision
- May require revision. Modern implants have excellent longevity
- Incidence
- 1-2% intraoperative, 1-2% postoperative
- Prevention Strategies
- Gentle technique, avoid varus malalignment, press-fit technique
- Impact on Decision
- May need revision or ORIF depending on timing and stability


When consenting for THA, must discuss: (1) Benefits - pain relief (90-95% success), improved function, better quality of life. (2) Risks - infection (1%), dislocation (2-3%), DVT/PE (1-2%), nerve injury (1-2%), revision (5% at 15 years), leg length inequality (10%), ongoing pain (5-10%). (3) Alternatives - conservative, hip preservation, other arthroplasty options. (4) Specific to patient - age-related revision risk, comorbidity risks.
Postoperative Care
Immediate postoperative management:
Postoperative Protocol
- Pain control: Multimodal analgesia (regional block, IV paracetamol, opioids as needed)
- DVT prophylaxis: LMWH or apixaban (start 6-12 hours post-op)
- Mobilization: Sit out of bed Day 0, walk with physio Day 1
- Precautions: Approach-specific (posterior = no flexion over 90°, adduction, IR)
- Progressive mobilization with walking aids
- Stair practice
- Discharge planning (home setup, support)
- Wound inspection
- Wound review, suture/staple removal
- Progress mobility, reduce walking aids
- Continue DVT prophylaxis (6 weeks total)
- Hip precautions education reinforcement
- Clinical review, X-ray (AP pelvis)
- Assess healing, component position, no subsidence
- Progress to full weight-bearing, discard aids if able
- Return to driving (if safe, right hip, off opioids)
- Return to work (desk 6 weeks, manual 3 months)
- Return to low-impact sports (swimming, cycling, golf)
- Avoid high-impact (running, jumping sports)
- Clinical examination, X-ray
- PROMs (Oxford Hip Score, satisfaction)
- Long-term surveillance plan (yearly first 5 years, then as needed)
Hip precautions (approach-dependent):
- Posterior approach: No flexion over 90°, no adduction past midline, no internal rotation (6-12 weeks)
- Anterior approach: No extension, external rotation, or adduction (6 weeks)
- Lateral approach: Minimal restrictions, avoid extreme abduction initially
Outcomes and Prognosis
- 90-95% of patients report significant pain improvement
- Most patients pain-free or minimal pain at rest and activity
- Night pain typically completely resolved
- Groin pain may persist in 5-10% (unexplained, may be from spine or soft tissues)
- Walking distance increases dramatically (unlimited in most patients)
- Stair climbing normalized
- ADLs (dressing, bathing, shoe tying) significantly easier
- Return to work: 80-90% return to previous work level
- Return to sport: Low-impact sports encouraged, high-impact discouraged
- 85-90% "very satisfied" with THA outcome
- 5-10% "satisfied with reservations" (ongoing pain, stiffness, LLD)
- Less than 5% "dissatisfied" (persistent pain, complications, unmet expectations)
- 5 years: 97% survival
- 10 years: 95% survival
- 15 years: 93-95% survival (modern implants)
- 25 years: 85-90% survival (projected)
- Impact on Outcome
- Higher lifetime revision risk
- Mitigation
- Counsel about revision burden, activity modification
- Impact on Outcome
- Higher infection, dislocation risk
- Mitigation
- Weight loss preoperatively, vigilant wound care
- Impact on Outcome
- Higher infection risk
- Mitigation
- Glycemic optimization before surgery
- Impact on Outcome
- Higher dislocation risk
- Mitigation
- Dual mobility bearing, constrained liner
- Impact on Outcome
- Better outcomes with high-volume surgeons
- Mitigation
- Refer complex cases to experienced surgeon
Long-term surveillance:
- Annual clinical review first 5 years
- X-rays at 1 year, then every 2-3 years
- Monitor for: pain (loosening, infection), wear, osteolysis
- AOANJRR tracks THA outcomes for long-term evidence
Guidelines, Registries & Global Practice
Global epidemiology. Osteoarthritis is the commonest indication for THA worldwide. The GBD 2021 study estimated 595 million people had osteoarthritis globally in 2020 (7.6% of the population), a 132% rise in cases since 1990, with hip OA cases projected to increase 78.6% by 2050; high BMI accounts for roughly 20% of the burden. This rising, ageing, increasingly obese population is driving worldwide growth in THA demand.
Major guidelines, side by side. Recommendations are broadly concordant: a structured trial of non-operative care first, then THA for symptomatic end-stage disease refractory to that care. The threshold and emphasis differ.
- Key guidance
- Patient education, weight loss, exercise/physiotherapy and NSAIDs first-line; THA for end-stage hip OA after non-operative measures fail
- Evidence emphasis
- Strong for exercise and NSAIDs; limited/short-term for intra-articular corticosteroid
- Key guidance
- Offer therapeutic exercise and weight management to all; refer for joint replacement when symptoms substantially affect quality of life and non-surgical care is ineffective - do not restrict by age, sex, smoking or BMI alone
- Evidence emphasis
- Explicitly warns against arbitrary BMI/age cut-offs for access
- Key guidance
- THA for disabling pain plus radiographic OA after appropriate conservative care; emphasis on shared decision-making and PROMs (Oxford Hip Score)
- Evidence emphasis
- Registry-informed (NJR) implant and bearing selection
- Key guidance
- Concordant indication; strong emphasis on cemented fixation in the elderly and on registry surveillance of implants
- Evidence emphasis
- Registry and RCT-led implant choice
- Key guidance
- For hip-fracture-related arthroplasty: THA preferred over hemiarthroplasty in fit, independent, cognitively intact older patients with displaced intracapsular fractures
- Evidence emphasis
- RCT evidence (HEALTH, FAITH)
Registry evidence. National joint registries are the highest-volume source of revision data and consistently agree on the major messages below.
- Consistent findings
- Tens of thousands of primary THAs/year; ~5% cumulative revision at 15 years; cemented/hybrid fixation lower revision in patients over 75; cross-linked polyethylene and ceramic bearings reduce wear-related revision; metal-on-metal and resurfacing higher revision, especially in women
- Consistent findings
- Largest registry globally; confirms low long-term revision for cemented and hybrid THA; higher revision for metal-on-metal and large-head designs
- Consistent findings
- Rapidly growing capture; predominance of cementless fixation; supports cross-linked polyethylene durability
- Consistent findings
- Pioneered registry methodology; long-standing evidence that cemented fixation is durable and that bearing/fixation choice should be registry-guided
Global practice variation. Fixation philosophy differs by region: cemented and hybrid THA predominate in Scandinavia, the UK and other registry-driven systems (registry-driven), whereas cementless fixation predominates in the USA and much of Asia. In high-resource settings the debate is bearing surface and approach; in limited-resource settings access, implant availability and cost dominate, and conventional rather than cross-linked polyethylene or cemented implants may be used for economic reasons. Across all systems the indication itself - disabling symptomatic end-stage hip disease that has failed appropriate conservative care - is universal.
- Informed consent: Document discussion of risks (infection, dislocation, DVT, revision), benefits (pain relief, function), alternatives (conservative, other surgery)
- Failed conservative: Document duration and compliance with non-operative treatment (minimum 6 months typically)
- Medical optimization: HbA1c if diabetic, cardiac clearance if indicated, MRSA screening
- Preoperative planning: Templating documented, leg length plan documented
- Complications disclosure: Specific percentages (infection 1%, dislocation 2-3%, revision 5% at 15 years)
- Patient expectations: Realistic goals discussed (pain relief yes, perfect hip no), activity restrictions
- Young patients: Lifetime revision burden explicitly discussed and documented
- Leg length discrepancy (most common cause of dissatisfaction) - document preoperative LLD and plan
- Infection (ensure optimization, prophylaxis, technique)
- Nerve palsy (avoid excessive lengthening, document neurovascular exam pre and post)
- Wrong level (confirm hip using imaging in OR)
For any board worldwide, anchor your answer in registry and guideline evidence rather than a single health system: (1) Indication is universal - disabling symptomatic end-stage hip disease refractory to appropriate conservative care; (2) Quote a registry - AOANJRR, NJR (England/Wales, the largest), AJRR (USA) or the Scandinavian registries all show roughly 5% revision at 15 years and lower revision with cemented/hybrid fixation in the elderly; (3) Guidelines concur (AAOS, NICE, BOA, EFORT, AO) on a conservative trial first; (4) NICE explicitly warns against denying surgery on age, BMI or smoking grounds alone; (5) Bearing choice should follow registry wear data because Level I RCT evidence shows no clear early survivorship difference between modern bearings under 65.
MCQ Practice Points
Q: What are the three essential components of the indication for total hip arthroplasty? A: (1) Pain and functional disability affecting quality of life, (2) Radiographic evidence of advanced osteoarthritis, (3) Failed conservative treatment for at least 6 months (physio, analgesia, weight loss, activity modification). All three must be present - radiographic severity alone is not an indication.
Q: What is the cumulative percent revision rate for primary THA at 15 years according to AOANJRR data? A: 5%, meaning 95% survivorship at 15 years for modern THA implants. This is one of the most successful surgical procedures. Key additional AOANJRR findings: (1) Over 50,000 THAs performed annually (AOANJRR), (2) Cemented femoral stems have lower revision rate in patients over 75 years, (3) Metal-on-metal hip resurfacing has higher revision rate than THA.
Q: What is the absolute contraindication to elective total hip arthroplasty? A: Active infection (local or systemic) is an absolute contraindication. This includes active hip infection (previous septic arthritis), distant infection (UTI, dental abscess), or bacteremia. Infection must be eradicated (minimum 6 weeks antibiotics, inflammatory markers normal) before proceeding with elective THA. Risk of hematogenous seeding to prosthetic joint is too high.
Q: What is the lifetime revision burden for a 40-year-old patient undergoing THA? A: High - studies show approximately 25% revision rate by 20 years in patients under 40. This means the patient may need 2-3 revisions over their lifetime. Main indications for revision: aseptic loosening (60%), instability (20%), infection (10%). Important to counsel young patients about this risk and consider hip preservation alternatives when possible.
Q: What HbA1c level is associated with significantly increased infection risk in THA, and what is the recommended management? A: HbA1c over 8% is associated with 3-fold increased risk of deep periprosthetic joint infection. Management: Postpone elective THA for 3 months of glycemic optimization with goal HbA1c under 8% (ideally under 7%). Refer to endocrinology, recheck HbA1c at 8-10 weeks. This is a modifiable risk factor - optimization reduces infection risk.
Q: At what stage of avascular necrosis is THA indicated, and why? A: THA is indicated at Stage III-IV (Ficat classification): Stage III = subchondral collapse (crescent sign), Stage IV = secondary acetabular arthritis. Why: Once collapse occurs, hip preservation (core decompression) is no longer effective. THA provides reliable pain relief and restoration of function. Stage I-II (pre-collapse) can be managed with hip preservation techniques.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old female presents with right hip pain for 3 years. Pain is in the groin, worse with walking, limits her to 200 meters. She has tried physiotherapy and takes paracetamol regularly. X-ray shows severe OA with joint space loss and osteophytes. Her contralateral hip is normal. She asks about hip replacement. What is your assessment and management?”
“A 35-year-old male presents with right hip pain for 6 months. He has a history of steroid use for asthma. X-ray shows collapse of the femoral head consistent with Stage III AVN. MRI shows early changes in the contralateral hip (Stage I). He is a keen footballer and works as a carpenter. He asks about his treatment options. How do you counsel him?”
“A 62-year-old male with severe hip OA is scheduled for THA in 2 weeks. His preoperative workup reveals HbA1c of 9.2%. He is on oral hypoglycemics and has been poorly controlled for several years. He is very keen to proceed as he is in significant pain. How do you manage this?”
Indication Triad
- Pain + Disability (affecting quality of life, sleep, ADLs)
- Radiographic OA (joint space loss, osteophytes, sclerosis)
- Failed conservative Rx (6+ months: physio, analgesia, injection)
- All three required - X-ray severity alone not an indication
Primary Diagnoses
- Osteoarthritis (85-90%) - most common indication
- AVN Stage III-IV (5-10%) - after collapse or secondary OA
- Inflammatory arthritis (2-5%) - RA, AS with joint destruction
- Post-traumatic (2-3%) - failed ORIF, fracture sequelae
- DDH and other (1-2%) - requires specialized planning
Contraindications
- ABSOLUTE: Active infection (local or systemic) - must eradicate first
- RELATIVE: Age under 50 (high revision burden, consider alternatives)
- RELATIVE: Severe obesity BMI over 40 (higher complications)
- RELATIVE: Uncontrolled medical comorbidities (optimize first)
- RELATIVE: Poor bone stock, neuromuscular disease (higher risk)
Age-Based Decision
- Under 40: Exhaust hip preservation, counsel re: 25% revision at 20 years
- 50-65: Optimal age, uncemented/hybrid, excellent outcomes
- Over 75: Cemented femoral stem (AOANJRR), medical optimization critical
- Young = higher revision burden, Old = higher perioperative risk
Preoperative Workup
- Medical: Cardiac risk (RCRI), HbA1c if diabetic (under 8% target), MRSA screen
- Dental: Clearance within 6 months, treat active infection
- Imaging: AP pelvis + lateral hip with magnification marker
- Templating: Predict component sizes, plan leg length restoration
- Consent: Infection 1%, dislocation 2-3%, DVT 1-2%, revision 5% at 15 years
AOANJRR Key Data
- Over 50,000 primary THAs per year (AOANJRR)
- 95% survivorship at 15 years (5% cumulative revision rate)
- Cemented femoral stems better in patients over 75 years
- Metal-on-metal resurfacing higher revision rate than THA
- Ceramic-on-polyethylene excellent long-term outcomes
Evidence Base and Key Studies
AOANJRR Annual Report 2023
- Over 50,000 primary total hip arthroplasties performed annually (AOANJRR)
- 95% cumulative percent revision at 15 years for primary THA (modern implants)
- Cemented femoral stems have lower revision rate than uncemented in patients over 75 years
- Ceramic-on-polyethylene and ceramic-on-ceramic bearings show excellent long-term survival
- Metal-on-metal hip resurfacing has higher revision rate compared to THA, especially in women
The Operation of the Century: Total Hip Replacement
- Landmark review framing THA as one of the most successful and cost-effective operations in medicine
- Charnley low-friction arthroplasty (1960s) transformed care of the arthritic hip with durable long-term results
- Both cemented and cementless fixation provide reliable, durable fixation when correctly indicated
- Younger, more active patients now drive demand and shift bearing-surface and design choices
- Long-term performance must not be compromised for short-term gains (e.g. minimally invasive techniques)
Dislocations After Total Hip-Replacement Arthroplasties (Lewinnek Safe Zone)
- Classic series of 300 THAs with 9 dislocations (3%) and precise measurement of cup orientation
- Defined the 'safe zone': acetabular anteversion 15 degrees plus or minus 10 and inclination 40 degrees plus or minus 10
- Dislocation rate 1.5% inside the safe zone versus 6.1% outside it
- Greatest dislocation risk in the first thirty days and in hips with prior surgery
- Anterior dislocation associated with increased acetabular component anteversion
Glycaemic Control, Diabetes and Perioperative Outcomes in Total Joint Arthroplasty
- Nationwide Inpatient Sample analysis of over 1 million joint replacement patients (1988-2005)
- Uncontrolled diabetes (n=3973) compared with controlled diabetes (n=105,485) and non-diabetic (n=920,555)
- Uncontrolled diabetes: adjusted odds of wound infection 2.28 (95% CI 1.36-3.81) versus controlled diabetes
- Uncontrolled diabetes also raised odds of stroke, urinary tract infection, ileus, transfusion and death
- Glycaemic control - not merely the presence of diabetes - drove the excess perioperative risk
Cementless Acetabular Fixation in Patients 50 Years and Younger
- 144 hips in 118 patients aged 50 years or younger followed 10-18 years after primary THA
- Only 2 cups (1.4%) revised for aseptic loosening - excellent biological fixation
- 24 hips (16.7%) revised for any mechanical acetabular failure, mostly liner wear and osteolysis
- Mean linear polyethylene wear 0.19 mm/year drove osteolysis and reduced overall construct survival
- Demonstrates that wear-related failure, not loss of fixation, limits THA longevity in young patients
Global Burden of Osteoarthritis 1990-2020 and Projections to 2050 (GBD 2021)
- 595 million people had osteoarthritis globally in 2020 - 7.6% of the world population
- Total osteoarthritis cases rose 132% since 1990, driven by ageing and population growth
- Hip osteoarthritis cases are projected to increase 78.6% between 2020 and 2050
- High BMI contributed an estimated 20.4% of the osteoarthritis burden
- Demand for joint replacement, highly effective for late-stage hip and knee OA, will rise in every region
No Survivorship Difference Among THA Bearing Surfaces in Patients Under 65 (Network Meta-analysis)
- Network meta-analysis of 18 RCTs (2599 THAs) in patients with mean age under 65 years
- No significant short- to mid-term survivorship difference between ceramic-on-ceramic, ceramic-on-crosslinked-poly and metal-on-crosslinked-poly
- Risk ratio for revision CoC versus CoPxl 0.65 (95% CI 0.19-2.23); CoC versus MoPxl 0.40 (0.06-2.63)
- Long-term RCT data still required to detect any late benefit in young, active patients
- Provides Level I evidence informing bearing selection in younger THA candidates