Patient Selection | Failed Conservative | Surgical Timing
- Primary OA is most common indication (95% of TKAs)
- Failed conservative management is prerequisite for surgery
- Radiographic severity must correlate with clinical symptoms
- Patient expectations are critical for satisfaction
- Absolute contraindications: Active infection, severe vascular disease
- “Kellgren-Lawrence Grade 3-4 correlates with surgical candidacy
- “Night pain and rest pain suggest advanced disease
- “BMI greater than 40 increases complications but not absolute contraindication
- “Age extremes require careful counseling regarding outcomes and revision risk
Pain and functional limitation refractory to conservative management including analgesia, physiotherapy, weight loss, injections. Radiographic OA with joint space narrowing, osteophytes, subchondral sclerosis correlating with symptoms.
Absolute: Active sepsis, remote infection, severe peripheral vascular disease, neuropathic joint. Relative: Morbid obesity (BMI greater than 40), poorly controlled diabetes (HbA1c greater than 8), immunocompromise, unrealistic expectations.
Minimum 3-6 months of non-operative treatment before considering surgery. Includes weight loss, physiotherapy, activity modification, analgesia (paracetamol, NSAIDs), walking aids, bracing, intra-articular injections (corticosteroid, hyaluronic acid).
Optimal candidates: Older than 55, unilateral disease, non-obese, motivated, realistic expectations. Higher risk: Younger than 55 (revision risk), morbid obesity, smokers, poorly controlled comorbidities, workers compensation claims.
Overview
Total knee arthroplasty is one of the most successful orthopaedic procedures, providing reliable pain relief and functional improvement for end-stage knee arthritis. Appropriate patient selection is critical for optimal outcomes, as up to 15-20% of patients remain dissatisfied despite technically successful surgery.
Historical Perspective
Modern TKA has evolved significantly since the 1970s. The development of constrained designs, improved polyethylene, and standardized surgical techniques has resulted in excellent long-term survivorship. Current focus is on optimizing patient selection and managing expectations.
Epidemiology
Knee osteoarthritis affects approximately 250 million people worldwide and is a leading cause of disability in older adults. Demand for TKA continues to rise globally with aging populations and increasing obesity prevalence; high-volume registries report annual primary TKA numbers in the hundreds of thousands (over 670,000 per year in the USA, roughly 100,000 per year in the UK via the NJR, and around 65,000 per year in Australia via the AOANJRR). Primary osteoarthritis accounts for around 95% of procedures across registries.
Surgical Approach Overview
Standard Approaches
- Most common approach
- Good exposure, extensile
- Standard for most primary TKA
- Subvastus (less quadriceps disruption)
- Midvastus (compromise approach)
- Lateral (valgus deformity)
- Indication
- Standard primary TKA
- Advantage
- Excellent exposure
- Indication
- Selected patients
- Advantage
- Less quad damage
- Indication
- Valgus deformity
- Advantage
- Better lateral access
Pathophysiology of Knee Arthritis
Osteoarthritis
Primary osteoarthritis is a disease of articular cartilage with progressive loss of hyaline cartilage, subchondral bone changes, osteophyte formation, and synovial inflammation. The process is irreversible once bone-on-bone contact occurs.
Inflammatory Arthritis
Rheumatoid arthritis and other inflammatory conditions cause synovial hypertrophy with pannus formation, leading to cartilage destruction, bone erosion, and ligamentous instability. Medical management with DMARDs has reduced but not eliminated the need for TKA.
Secondary Causes
Post-traumatic arthritis following tibial plateau fractures, ligament injuries, or meniscectomy represents a significant proportion of younger TKA patients. Osteonecrosis, crystal arthropathies, and hemophilic arthropathy are less common causes.
Clinical-radiographic correlation is essential. Some patients with severe radiographic OA have minimal symptoms, while others with mild changes have significant pain. The indication for TKA is failed conservative management of symptomatic arthritis, not radiographic severity alone.
Classification Systems
Kellgren-Lawrence Radiographic Classification
The most widely used grading system for knee osteoarthritis severity based on weight-bearing radiographs.
- Radiographic Findings
- No features of OA
- Clinical Correlation
- Normal knee
- Surgical Candidacy
- No indication
- Radiographic Findings
- Doubtful JSN, possible osteophytes
- Clinical Correlation
- Minimal symptoms
- Surgical Candidacy
- Conservative management
- Radiographic Findings
- Definite osteophytes, possible JSN
- Clinical Correlation
- Mild-moderate symptoms
- Surgical Candidacy
- Conservative, possibly UKA
- Radiographic Findings
- Moderate osteophytes, definite JSN, sclerosis
- Clinical Correlation
- Moderate symptoms
- Surgical Candidacy
- Consider TKA if failed conservative
- Radiographic Findings
- Large osteophytes, severe JSN, bone-on-bone
- Clinical Correlation
- Severe symptoms
- Surgical Candidacy
- TKA candidate
The Kellgren-Lawrence classification provides standardized grading for radiographic osteoarthritis severity.
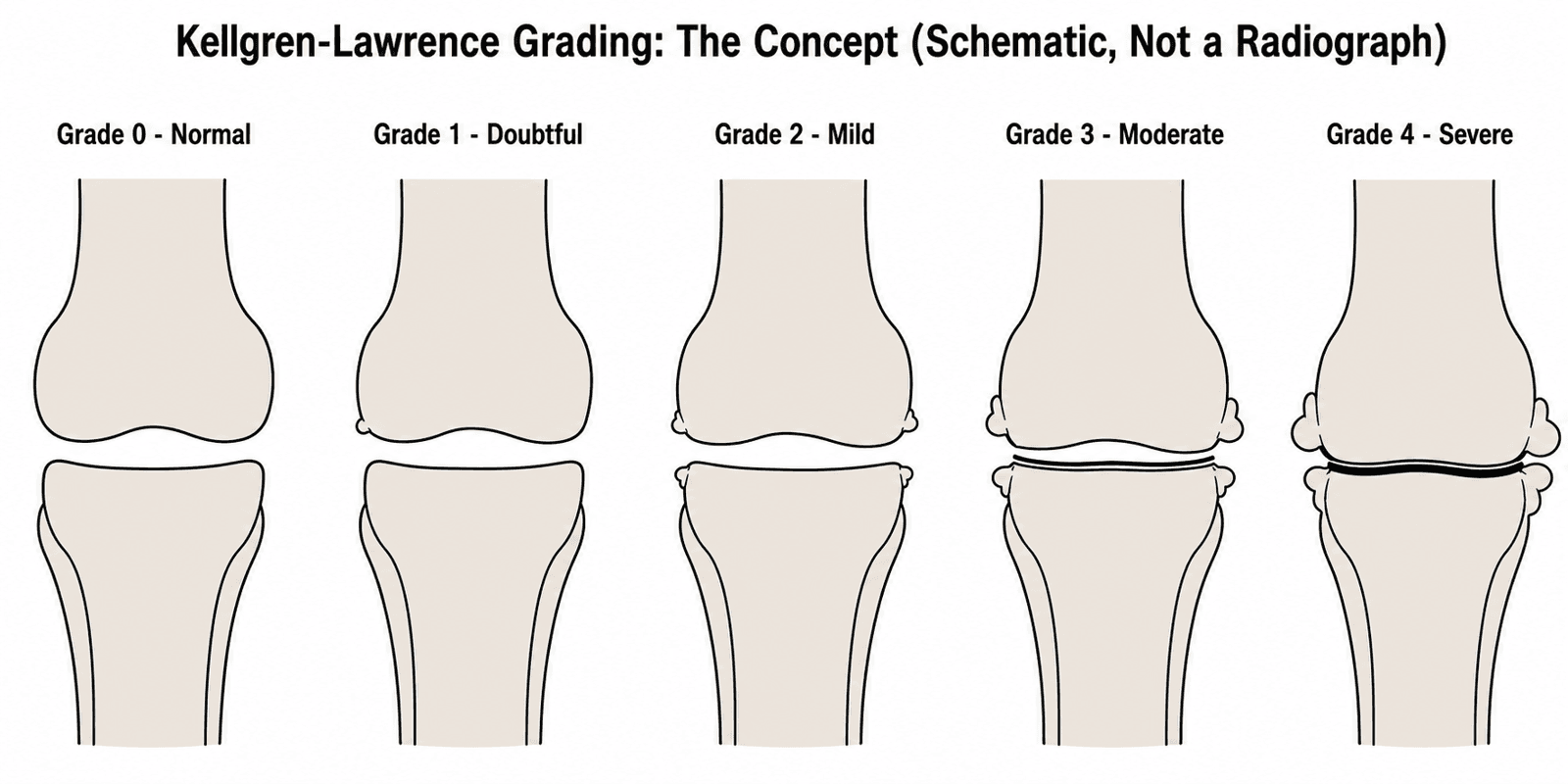
TKA does not require bone-on-bone contact. KL Grade 3 with failed conservative management and significant symptoms is an appropriate indication. However, milder grades should exhaust conservative options and may be suitable for osteotomy or UKA.
Investigations
Preoperative Workup
- Weight-bearing AP, lateral, skyline radiographs
- Long-leg alignment films (if deformity)
- MRI rarely needed (unless diagnostic uncertainty)
- FBC, UEC, LFTs, coagulation
- HbA1c (diabetics, target less than 8%)
- CRP/ESR (rule out infection if suspected)
- Purpose
- Glycemic control
- Target
- Less than 8%
- Purpose
- Bone health
- Target
- Greater than 75 nmol/L
- Purpose
- Nutritional status
- Target
- Greater than 35 g/L
- Purpose
- Cardiac assessment
- Target
- No acute changes
Differential Diagnosis of the Painful Knee
Before attributing pain to arthritis and proceeding to TKA, exclude mimics and confirm clinical–radiographic correlation. A painful knee in an older adult is not always intra-articular OA, and referred or extra-articular pain will not improve after arthroplasty.
- Distinguishing Features
- Activity-related and night/rest pain, stiffness, deformity, crepitus
- Key Investigation
- Weight-bearing radiograph (KL 3-4)
- Why It Matters for TKA
- The correct indication when conservative care fails
- Distinguishing Features
- Groin/thigh pain, pain on hip rotation, antalgic gait
- Key Investigation
- Hip radiograph, examine hip
- Why It Matters for TKA
- TKA will not relieve hip-referred pain
- Distinguishing Features
- Radiating pain, dermatomal sensory change, neuro signs
- Key Investigation
- Lumbar exam, MRI spine if indicated
- Why It Matters for TKA
- Spinal origin not addressed by TKA
- Distinguishing Features
- Hot swollen joint, fever, raised CRP/ESR
- Key Investigation
- Aspiration: cell count, culture
- Why It Matters for TKA
- Absolute contraindication to implant
- Distinguishing Features
- Acute flares, chondrocalcinosis, raised urate
- Key Investigation
- Aspiration for crystals
- Why It Matters for TKA
- Treat flare; may coexist with OA
- Distinguishing Features
- Polyarticular, morning stiffness, raised inflammatory markers
- Key Investigation
- RF/anti-CCP, ESR/CRP
- Why It Matters for TKA
- Valid indication but plan DMARD and timing
- Distinguishing Features
- Anterior pain on stairs/rising, skyline changes only
- Key Investigation
- Skyline radiograph
- Why It Matters for TKA
- Consider PFA rather than TKA
- Distinguishing Features
- Localised medial tenderness below joint line
- Key Investigation
- Clinical exam
- Why It Matters for TKA
- Extra-articular; TKA inappropriate
Conservative Management Trial

- Evidence Level
- Level I
- Expected Benefit
- Significant pain reduction per 5kg lost
- Duration/Dose
- 5-10% body weight target
- Evidence Level
- Level I
- Expected Benefit
- Strength, proprioception, function
- Duration/Dose
- 6-12 weeks supervised program
- Evidence Level
- Level I
- Expected Benefit
- Mild pain relief, safe long-term
- Duration/Dose
- 1g QID maximum 4g daily
- Evidence Level
- Level I
- Expected Benefit
- Moderate pain relief
- Duration/Dose
- Lowest effective dose, GI protection
- Evidence Level
- Level I
- Expected Benefit
- Short-term relief 4-8 weeks
- Duration/Dose
- Maximum 3-4 per year
- Evidence Level
- Level II
- Expected Benefit
- Controversial, modest benefit
- Duration/Dose
- 3-5 weekly injections
- Evidence Level
- Level II
- Expected Benefit
- Unloading affected compartment
- Duration/Dose
- Continuous use during activity
When Conservative Fails
Conservative management is considered failed when adequate trials of multiple modalities over 3-6 months fail to provide sufficient pain relief or functional improvement. Night pain and rest pain are particularly indicative of advanced disease requiring surgery.
Management Algorithm
Decision Making
Step 1: Confirm Diagnosis
- Radiographic OA with symptom correlation
- Exclude other causes (infection, referred pain)
Step 2: Conservative Trial
- Minimum 3-6 months
- Weight loss, physiotherapy, analgesia, injections
Step 3: Patient Selection
- Assess contraindications
- Optimize modifiable risk factors
- Action
- Conservative management
- Duration
- 3-6 months
- Action
- Risk factor modification
- Duration
- Variable
- Action
- TKA if failed conservative
- Duration
- When optimized
Complications
Potential Complications
- Surgical site infection (1-2%)
- DVT/PE (1-2% symptomatic)
- Stiffness (5-10%)
- Wound problems (2-5%)
- Aseptic loosening (1% per year)
- Periprosthetic fracture (1-2%)
- Late infection (0.5% per year)
- Polyethylene wear
- Incidence
- 1-2%
- Prevention
- Optimization, prophylaxis
- Incidence
- 1-2% symptomatic
- Prevention
- Chemoprophylaxis
- Incidence
- 5-10%
- Prevention
- Early mobilization, PT
- Incidence
- 5% at 10 years
- Prevention
- Technique, alignment
Postoperative Care
Recovery Protocol
- Full weight-bearing with walker/crutches
- DVT prophylaxis (2-6 weeks)
- Physiotherapy for ROM and strength
- Wound care
- Progress to independent walking
- Return to sedentary activities
- Continue physiotherapy
- Activity
- Protected walking
- Goals
- ROM 0-90°
- Activity
- Independent ambulation
- Goals
- Full extension
- Activity
- Light activities
- Goals
- ROM 0-120°
Outcomes
Expected Results
- 95% at 10 years
- 90% at 15 years
- 85% at 20 years
- 85% satisfied overall
- 15-20% have residual dissatisfaction
- Expectations predict satisfaction
- Result
- ~95%
- Comment
- Pooled registry data
- Result
- 85%
- Comment
- Patient selection critical
- Result
- Variable
- Comment
- Low-impact only
- Result
- 90%+
- Comment
- Most reliable outcome
Clinical Relevance and Patient Selection
Absolute Indications
The primary indication for TKA is end-stage knee arthritis with failed conservative management characterized by:
- Significant pain affecting quality of life
- Functional limitation (walking distance, stairs, ADLs)
- Night pain and rest pain
- Radiographic changes correlating with symptoms
- Failure of at least 3-6 months conservative care
Specific Conditions
Primary osteoarthritis accounts for approximately 95% of TKAs. Other indications include rheumatoid arthritis, post-traumatic arthritis, osteonecrosis, and crystalline arthropathy. Each requires individualized assessment.
This comprehensive evaluation ensures appropriate patient selection.
Guidelines, Registries & Global Practice
Global Epidemiology
Knee OA affects an estimated 250 million people worldwide and is among the leading global causes of years lived with disability. Primary OA accounts for around 95% of TKAs across all major registries. Procedure volumes are rising fastest in ageing, higher-income populations, driven by demographics and obesity.
Side-by-Side Guideline Comparison
- Conservative trial
- Required: exercise, weight management, education
- BMI / age cut-offs
- No arbitrary BMI/age refusal
- Emphasis
- Shared decision-making, symptoms over imaging
- Conservative trial
- Non-operative first-line (exercise, NSAIDs, weight loss)
- BMI / age cut-offs
- Optimise modifiable risks; no absolute BMI bar
- Emphasis
- Evidence-based non-operative ladder before TKA
- Conservative trial
- Failed appropriate non-operative care
- BMI / age cut-offs
- Optimise, do not ration on BMI alone
- Emphasis
- Surgical thresholds and informed consent
- Conservative trial
- Structured non-surgical care trial
- BMI / age cut-offs
- Risk optimisation, individualised
- Emphasis
- Registry-informed practice, prehabilitation
Registry Evidence
National joint registries (NJR for England/Wales, AJRR in the US, AOANJRR in Australia, SHAR/Swedish, Norwegian, NZJR) consistently show 10-year primary TKA revision of around 4-6% and pooled 25-year survival around 82% (Evans, Lancet 2019). Younger age and male sex are reproducible revision risk factors. Registries also benchmark implant and fixation performance and flag outlier devices.
High- vs Limited-Resource Practice Variation
- High-resource settings: prehabilitation clinics, dedicated arthroplasty pathways, enhanced recovery, robotic/PSI options, day-case TKA in selected patients, and registry surveillance.
- Limited-resource settings: longer waiting times allow disease to progress to severe deformity; implant and revision capacity is constrained, so case selection is more conservative and durable, lower-cost cemented implants are favoured. Access and affordability, not indication, are the dominant limiting factors.
Special Populations
Young Patients (Under 55)
Younger patients have higher activity demands and longer life expectancy, resulting in:
- Higher revision rates (15-20% at 15 years vs 5-10% in older patients)
- Need for realistic expectations about activity limitations
- Consideration of alternative procedures (osteotomy, UKA)
- Discussion of future revision surgery likelihood
Elderly Patients (Over 80)
Older patients have higher perioperative medical risks but excellent pain relief outcomes. Considerations include:
- Medical optimization essential
- Higher cardiac and pulmonary complication rates
- Excellent functional improvement despite comorbidities
- Single-stage bilateral TKA generally avoided
Morbid Obesity
BMI greater than 40 increases surgical complications:
- Surgical site infection increased 2-3 fold
- DVT and PE risk elevated
- Implant loosening rates higher
- Weight loss programs beneficial but surgery not contraindicated
Assessing and Managing Patient Expectations
The Bourne cross-sectional study of 1703 primary TKAs found that unmet expectations were by far the strongest predictor of dissatisfaction (about a tenfold increase in risk) — a larger effect than pain, function scores or complications. Yet expectation assessment is often informal and rushed. Because roughly one in five patients remain dissatisfied despite technically sound surgery, structured expectation work is a core part of appropriate patient selection, not an afterthought.
Eliciting Expectations
- Ask specifically what the patient hopes to achieve — pain relief, walking distance, stairs, return to work, sport, or kneeling — rather than accepting a vague "get back to normal".
- Validated instruments exist to structure this, such as the Hospital for Special Surgery Knee Replacement Expectations Survey (HSS-KRES), which quantifies the number and type of expectations a patient holds.
- Satisfaction depends on whether expectations are met (fulfilment), not on the absolute outcome score — two patients with identical objective results can differ in satisfaction according to what they expected.
Common Unrealistic Expectations to Correct
- Complete elimination of all pain and a "forgotten", entirely normal knee — TKA reliably reduces pain and improves function but is a resurfacing procedure, not restoration of a native joint.
- Return to high-impact sport or heavy manual labour without restriction.
- Comfortable kneeling, which remains difficult or uncomfortable for a large proportion of patients long-term and should be explicitly discussed.
- Rapid recovery — meaningful functional gains and pain plateau typically continue to evolve over the first postoperative year.
Aligning Expectations
Use structured preoperative education, decision aids and shared decision-making to correct misconceptions, then document the agreed, realistic goals. Screen for the psychological and pain-sensitisation drivers of poor outcome (owned by the knee-osteoarthritis topic) and involve them in counselling. Managing expectations is the single most powerful modifiable lever on postoperative satisfaction.
Unmet expectations are the strongest predictor of dissatisfaction after TKA (Bourne 2010). Elicit specific goals, correct unrealistic ones (a "normal" knee, unrestricted sport, comfortable kneeling), and document a realistic shared plan. Kneeling difficulty in particular must be discussed explicitly before surgery.
Bilateral TKA: Simultaneous versus Staged
Many candidates for TKA have symptomatic bilateral disease, forcing a distinct selection decision that the topic flags but does not resolve: should both knees be replaced under one anaesthetic (simultaneous) or as two separate operations (staged)?
The Trade-off
- Simultaneous bilateral TKA offers a single anaesthetic, one hospital admission, one rehabilitation episode, faster overall recovery of both limbs, and lower total cost. However, it carries a higher risk of cardiopulmonary complications and blood transfusion, and several studies report increased perioperative mortality compared with staged surgery.
- Staged bilateral TKA spreads the physiological insult across two events, allowing recovery and reassessment between operations, at the cost of a second anaesthetic, a second admission and a longer total treatment course.
Patient Selection
Because the added risk falls on the cardiopulmonary system, simultaneous surgery is generally reserved for younger, fitter patients (typically ASA grade one or two) without significant cardiac or pulmonary disease, with careful shared decision-making and informed consent about the higher perioperative risk. Older patients and those with meaningful comorbidity are better served by a staged approach or by treating the more symptomatic knee first. When knees are staged, the interval is individualised to allow adequate recovery before the second procedure.
Reserve simultaneous bilateral TKA for young, fit, low-comorbidity patients (ASA one to two). The benefit is a single anaesthetic, admission and rehabilitation; the price is higher cardiopulmonary complication, transfusion and, in several series, mortality risk. Comorbid or elderly patients should be staged.
Controversies and Areas of Uncertainty
- BMI thresholds: Many units historically applied a hard BMI cut-off (often 40) for elective TKA. The evidence (Dowsey 2010) shows higher complications and smaller functional gains in the morbidly obese, but absolute benefit remains substantial, and guidelines (NICE) explicitly reject refusing surgery on BMI alone. The debate is optimisation and shared decision-making versus rationing.
- Timing — too early vs too late: The MEDIC RCT (Skou 2015) shows structured non-surgical care helps many "surgery-eligible" patients, supporting a genuine conservative trial; yet excessive delay risks fixed deformity, muscle wasting and worse outcomes. There is no universally agreed minimum trial duration; 3-6 months is pragmatic, not evidence-mandated.
- The persistently dissatisfied 15-20%: Roughly one in five patients are dissatisfied despite technically sound surgery (Bourne 2010), driven largely by unmet expectations and central pain sensitisation rather than implant or technique. Selecting and counselling these patients remains unsolved.
- Age limits: Younger patients gain function but face higher lifetime revision risk; older patients carry higher perioperative medical risk but excellent pain relief. Chronological age alone is a poor selection criterion.
- Bilateral simultaneous vs staged TKA: Simultaneous bilateral reduces total hospital time and a second anaesthetic but carries higher cardiopulmonary and transfusion risk; patient selection is debated.
- Robotic and patient-specific instrumentation: Improve alignment precision but have not yet shown consistent long-term survivorship or satisfaction benefit to justify routine use everywhere — a cost-versus-value question, especially in limited-resource settings.
MCQ Practice Points
Q: What is the most common indication for total knee arthroplasty? A: Primary osteoarthritis accounts for approximately 95% of TKA procedures. The key requirement is end-stage arthritis with failed conservative management over 3-6 months, not radiographic severity alone.
Q: What are the absolute contraindications to TKA? A: Remember STING: Sepsis/active infection (local or remote), Tuberculosis or remote infection, Ischemic limb (severe PVD), Neuropathic joint (Charcot), Generally unfit for surgery. Active infection is the most critical - never proceed with untreated UTI, dental abscess, or skin infection.
Q: Is Kellgren-Lawrence Grade 4 required for TKA? A: No. KL Grade 3 with significant symptoms and failed conservative management is an appropriate indication. The indication is symptomatic arthritis with failed conservative care, not radiographic severity alone. Some patients with KL4 have minimal symptoms and don't need surgery.
Q: What HbA1c threshold should be achieved before elective TKA? A: Target HbA1c less than 8%, ideally less than 7.5%. Perioperative glucose should be maintained below 10 mmol/L. Poor glycemic control increases surgical site infection risk threefold.
At a Glance
Total knee arthroplasty (TKA) is indicated for end-stage knee arthritis with pain and functional limitation refractory to conservative management (minimum 3-6 months trial). Primary osteoarthritis accounts for 95% of TKAs, with Kellgren-Lawrence Grade 3-4 radiographic changes that correlate with clinical symptoms. Absolute contraindications include active infection and severe peripheral vascular disease; relative contraindications include morbid obesity (BMI over 40), poorly controlled diabetes (HbA1c over 8), and unrealistic expectations. Optimal candidates are over 55 years, non-obese, motivated, and have realistic expectations. TKA achieves 95% 10-year survivorship and 85% patient satisfaction when patient selection is appropriate. Night pain and rest pain suggest advanced disease warranting surgical consideration.
ARTHRITISTKA Indication Checklist
Hook:ARTHRITIS criteria must be met before TKA!
STINGAbsolute Contraindications
Hook:STING means no TKA until resolved!
OBESERelative Contraindications
Hook:OBESE patients need optimization before TKA!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman presents with bilateral knee pain worse on the right for 5 years. She has tried physiotherapy, NSAIDs, and two cortisone injections without lasting relief. X-rays show KL Grade 4 changes on the right. What are your thoughts on surgical management?”
“A 52-year-old builder presents with severe right knee pain limiting his ability to work. He has post-traumatic OA following tibial plateau fracture 15 years ago. Failed all conservative measures. What are your considerations?”
“A 72-year-old diabetic man with BMI 42 and recurrent UTIs requests TKA for severe OA. His HbA1c is 9.2% and he is an active smoker. How do you approach this case?”
Key Indications
- End-stage OA (KL Grade 3-4) with symptoms
- Failed 3-6 months conservative management
- Significant functional limitation and pain
- Night pain and rest pain suggest advanced disease
Absolute Contraindications (STING)
- Sepsis/active infection
- TB or remote infection
- Ischemic limb (severe PVD)
- Neuropathic joint (Charcot)
- Generally unfit for surgery
Relative Contraindications (OBESE)
- Obesity morbid (BMI greater than 40)
- Blood sugar uncontrolled (HbA1c greater than 8%)
- Expectations unrealistic
- Smoking active
- Extreme youth (under 50)
Preop Optimization
- HbA1c less than 8% (ideally under 7.5%)
- Smoking cessation 4 plus weeks
- Weight loss encouraged if obese
- Dental clearance, treat infections
Evidence Base
- 100 patients with moderate-to-severe knee OA eligible for TKR, randomised to TKR plus non-surgical care vs non-surgical care alone
- TKR group had greater 12-month KOOS4 improvement (32.5 vs 16.0; adjusted mean difference 15.8, 95% CI 10.0 to 21.5)
- More serious adverse events in the TKR group (24 vs 6, P=0.005)
- Only 26% of the non-surgical group crossed over to TKR within 12 months
- Cross-sectional study of 1703 primary TKAs in Ontario, Canada
- Approximately 1 in 5 patients (19%) were not satisfied with the outcome
- Strongest predictor of dissatisfaction was unmet expectations (10.7x risk)
- Other predictors: low 1-year WOMAC, preoperative rest pain, complication requiring readmission
- Systematic review and meta-analysis of case series and national registries with 15+ years follow-up
- Pooled registry 25-year all-cause survival of primary TKR was 82.3% (95% CI 81.3 to 83.2)
- Pooled 25-year survival for UKR was 69.8%
- Based on roughly 300,000 TKRs from 14 registries
- Retrospective study of 462 diabetic patients (714 TKAs)
- Preoperative HbA1c greater than or equal to 8% was associated with superficial SSI (OR 6.1, 95% CI 1.6 to 23.4)
- Fasting glucose greater than or equal to 200 mg/dL also predicted SSI (OR 9.2)
- Supports glycaemic optimisation before elective TKA
- Prospective study of 529 consecutive primary TKAs stratified by BMI
- Adverse events rose with BMI: 14.2% non-obese, 22.6% obese, 35.1% morbidly obese (P=0.001)
- Functional (Knee Society) gains were smaller in obese and morbidly obese groups
- Most obese patients did not lose clinically significant weight after surgery
- Original description of the radiographic grading system for osteoarthritis
- Grades 0-4 based on osteophytes, joint space narrowing, sclerosis and bone contour
- Remains the most widely used radiographic OA classification worldwide
- Grade 3-4 changes correspond to moderate-to-severe radiographic disease
- Offer joint replacement when conservative measures no longer control symptoms or affect quality of life
- Do not use age, sex, BMI or comorbidities alone to refuse referral for surgery
- Emphasise shared decision-making and realistic expectations
- Core non-surgical care: exercise, weight management and education for all