Rare | All Joints | Urgent Reduction | High AVN Risk
- Total talar dislocation = talus completely dislocated from all articulations (ankle, subtalar, talonavicular) - extremely rare, urgent reduction required
- Urgent reduction required - Skin tension causes necrosis, neurovascular compromise, high AVN risk. Reduce within hours, do not delay
- High AVN risk (50-100%) - Complete disruption of blood supply, prolonged dislocation increases risk. Monitor with serial imaging
- Often open injury - Skin disruption common due to high-energy mechanism. Urgent debridement required
- ORIF if fractures present - After reduction, address talar fractures with ORIF. Restore joint congruity
- “Rare but serious, urgent reduction required
- “High AVN risk (50-100%)
- “Often open injury
- “ORIF if fractures present
Urgent reduction required - Skin tension causes necrosis within hours, neurovascular compromise, high AVN risk. Reduce within hours, do not delay for imaging. Document neurovascular status before and after reduction.
High AVN risk (50-100%) - Complete disruption of blood supply to talus. Prolonged dislocation increases risk. Monitor with serial imaging (Hawkins sign at 6-8 weeks). May require talectomy or fusion if AVN develops.
Often open injury - Skin disruption common due to high-energy mechanism. Urgent debridement required. Higher infection risk. Worse outcomes than closed injuries.
ORIF if fractures present - After reduction, address talar fractures with ORIF. Restore joint congruity. Success rate 50-70% due to high AVN risk."
- Frequency
- Rare, no fractures
- Treatment
- Urgent reduction
- Outcome
- 50-70% good results
- Frequency
- Common, talar fractures
- Treatment
- Urgent reduction, ORIF
- Outcome
- 40-60% good results
- Frequency
- Common, skin disrupted
- Treatment
- Urgent reduction, debridement
- Outcome
- 30-50% good results
TOTALTotal Talar Dislocation Features
Hook:TOTAL: Total dislocation, Open often, Talus dislocated, AVN high risk, Lateral most common!
AVNAVN Risk
Hook:AVN: AVN high risk, Vascular disruption, Necrosis monitoring!
Overview and Epidemiology
Total talar dislocation is an extremely rare but serious injury where the talus is completely dislocated from all its articulations (ankle, subtalar, talonavicular). This injury requires urgent reduction and has a high risk of AVN.
Definition
Total talar dislocation: Complete dislocation of talus from all articulations, which:
- Joints involved: Ankle (tibiotalar), subtalar (talocalcaneal), talonavicular
- Mechanism: High-energy trauma
- Treatment: Urgent reduction, then ORIF if fractures
- Outcome: Poor due to high AVN risk
Types:
- Pure: No fractures, rare
- With fractures: Talar fractures, common
- Open: Skin disrupted, common
Epidemiology
- Incidence: Extremely rare (less than 0.1% of dislocations)
- Age: Peak 20-40 years (trauma population)
- Gender: No clear predominance
- Mechanism: High-energy trauma (MVA, falls from height)
- Associated injuries: Talar fractures, open injuries
Urgent reduction required - Skin tension causes necrosis within hours, neurovascular compromise, high AVN risk. Reduce within hours, do not delay for imaging. Document neurovascular status before and after reduction.
Anatomy and Pathophysiology
Talar Anatomy
Articulations:
- Ankle (tibiotalar): Tibia and fibula
- Subtalar (talocalcaneal): Calcaneus
- Talonavicular: Navicular
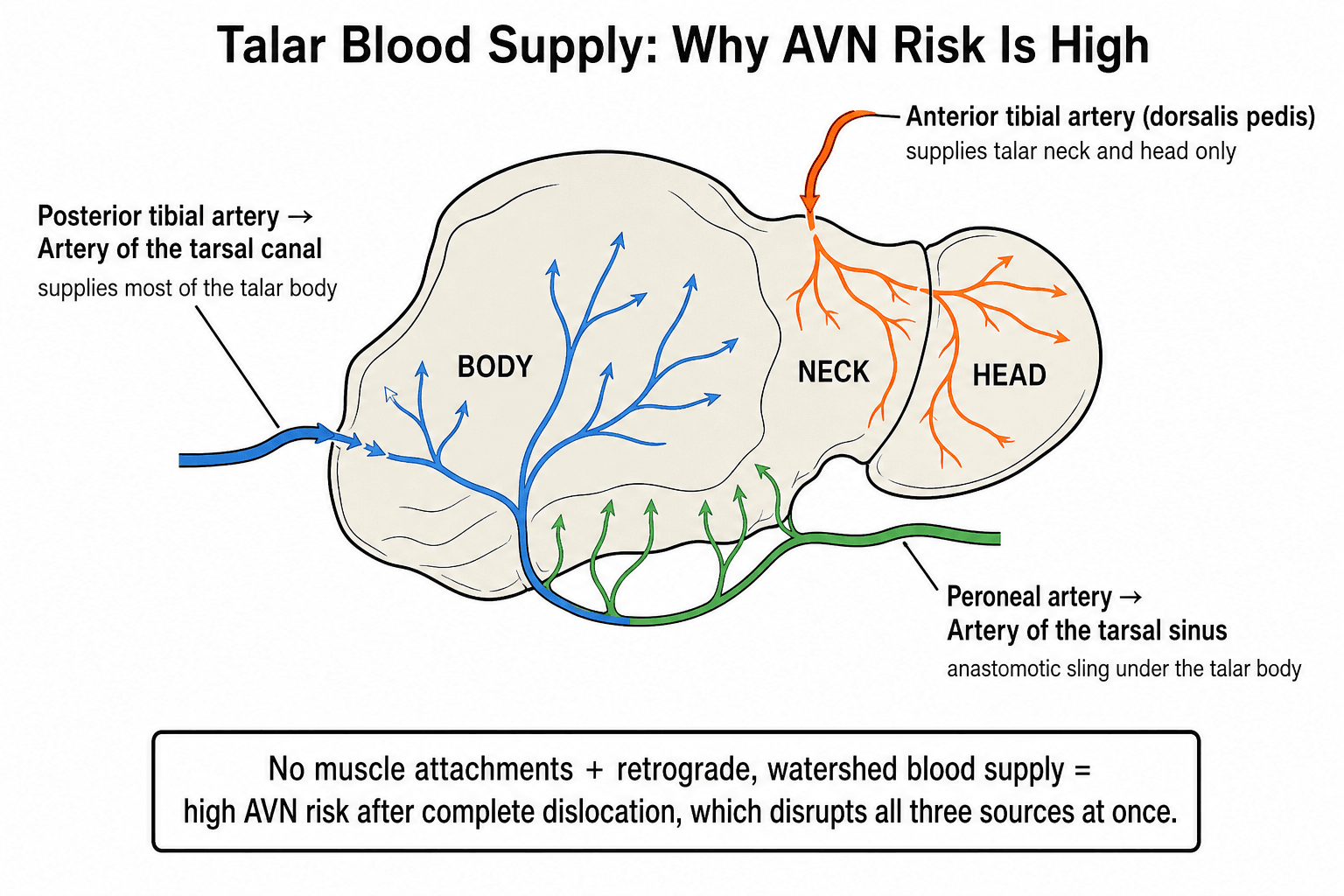
Blood supply:
- Posterior tibial artery: Artery of tarsal canal
- Anterior tibial artery: Talar neck and head
- Peroneal artery: Artery of tarsal sinus
- Tenuous: 60% articular cartilage, no muscle attachments
Pathophysiology
Injury mechanism:
- High-energy trauma: MVA, falls from height
- Forces: Extreme rotation, translation, axial loading
- Complete disruption: All ligaments and capsules
Why urgent reduction:
- Skin tension: Causes necrosis within hours
- Neurovascular compromise: Risk of ischemia
- AVN risk: Prolonged dislocation increases AVN risk
Why high AVN risk:
- Complete disruption: All blood supply disrupted
- Tenuous supply: Talus has tenuous blood supply
- Prolonged dislocation: Increases AVN risk
Classification Systems
Pattern-Based Classification
Pure dislocation:
- No fractures
- Rare
- Treatment: Urgent reduction
With fractures:
- Talar fractures
- Common
- Treatment: Urgent reduction, ORIF
Open injury:
- Skin disrupted
- Common
- Treatment: Urgent reduction, debridement
Pattern guides treatment approach.
Clinical Assessment
History
Symptoms:
- Ankle/foot pain: Severe pain
- Deformity: Obvious deformity
- Inability to weight bear: Cannot bear weight
- Mechanism: High-energy trauma
Risk factors:
- High-energy trauma
- MVA, falls from height
- Sports injuries
Physical Examination
Inspection:
- Obvious deformity
- Swelling
- Skin tenting (urgent reduction)
- Open wound (if open)
Palpation:
- Tenderness over ankle/foot
- Crepitus (if fractures)
- Deformity
Neurovascular:
- Document before reduction: Critical
- Pulses: Dorsalis pedis, posterior tibial
- Sensation: Dorsal and plantar foot
- Motor: Ankle dorsiflexion, plantarflexion
Range of Motion:
- Ankle/foot ROM limited and painful
- Cannot test due to pain
Document neurovascular status before reduction - Critical for medicolegal and clinical reasons. Check pulses (dorsalis pedis, posterior tibial), sensation (dorsal and plantar foot), and motor function (ankle dorsiflexion, plantarflexion). Repeat after reduction.
Investigations
Standard X-ray Protocol
AP view:
- Shows dislocation
- Assess talus position
- Check for fractures
Lateral view:
- Shows dislocation direction
- Assess talus position
- Check for fractures
Mortise view:
- Shows mortise alignment
- Assess talus position
Key point: Do not delay reduction for imaging if skin compromised.
Differential Diagnosis
The key exam discriminator is distinguishing total (pan-talar) dislocation from the more common partial peritalar injuries. The talus has three articulations; defining how many are dislocated and whether the talus retains a tibiotalar relationship guides both terminology and treatment.
- Joints Dislocated
- Tibiotalar + subtalar + talonavicular
- Key Radiographic Feature
- Talus extruded from all articulations, empty mortise
- Distinguishing Point
- Talus separated from tibia, calcaneus AND navicular
- Joints Dislocated
- Subtalar + talonavicular (talus stays in mortise)
- Key Radiographic Feature
- Talus normal in mortise, foot displaced beneath it
- Distinguishing Point
- Tibiotalar joint intact - talus stays with tibia
- Joints Dislocated
- Subtalar and/or tibiotalar via fracture plane
- Key Radiographic Feature
- Fracture line through neck, body displaced
- Distinguishing Point
- Talar body fractured, not whole-bone extrusion
- Joints Dislocated
- Tibiotalar only
- Key Radiographic Feature
- Malleolar fractures, talar shift in mortise
- Distinguishing Point
- Subtalar and talonavicular remain congruent
- Joints Dislocated
- Talonavicular + calcaneocuboid
- Key Radiographic Feature
- Disruption at midtarsal line
- Distinguishing Point
- Talus stays in mortise and on calcaneus
The single most testable distinction: in subtalar dislocation the talus stays in the mortise and the foot dislocates beneath it, whereas in total talar dislocation the talus itself is extruded from all three articulations (tibiotalar, subtalar and talonavicular). Count the joints.
Management Algorithm
Management Pathway
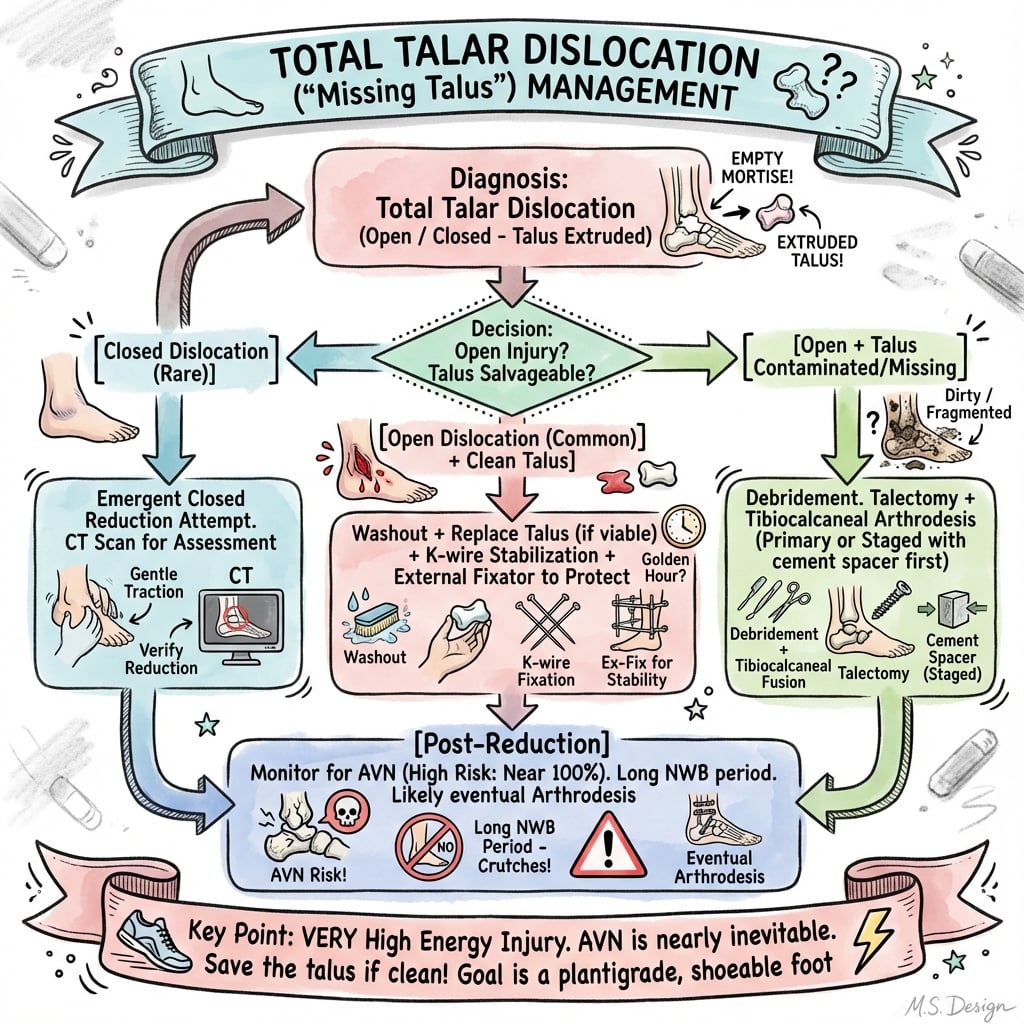
Total Talar Dislocation Management
Diagnose total talar dislocation clinically and radiographically. Document neurovascular status before reduction. Do not delay reduction for imaging if skin compromised. Urgent reduction required within hours.
Closed reduction under sedation or general anesthesia - Flex knee to relax gastrocnemius, traction, then reverse deformity based on direction. Document neurovascular status after reduction. Success rate 60-70% for closed reduction.
CT scan after reduction to assess talar fractures - 60-80% have associated talar fractures. Assess displacement and plan ORIF if indicated.
ORIF if fractures present and displaced - Talar fractures require ORIF if displaced. Restore joint congruity. Success rate 50-70% due to high AVN risk.
Surgical Technique
ORIF Talar Fractures
Indications:
- Displaced talar fractures
- Associated with dislocation
- Unstable after reduction
Approach:
- Anterior approach for talar neck
- Medial or lateral approach for talar body
- Dual incisions if needed
Technique:
- Exposure: Approach based on fracture location, expose fracture, protect neurovascular structures
- Reduction: Anatomic reduction of fracture to restore joint congruity
- Fixation: Screws (3.5-4.5mm) or plate
- Verification: Confirm reduction and hardware position fluoroscopically, verify joint congruity restored
Advantages:
- Restores joint congruity
- Prevents arthritis
- Allows early motion
ORIF restores joint congruity.
Why Closed Reduction Often Fails and the Direction-Specific Technique
The topic's decision tree quotes a closed-reduction success rate around 60 to 70 percent, yet its own controversy panel notes that closed reduction is frequently impossible. Reconciling these two statements is a common viva trap, and the reason matters for how you plan the reduction.
Why the talus buttonholes
In a total (pan-talar) dislocation the extruded talus commonly buttonholes through a rent in the surrounding capsule, retinaculum or skin, and tendons and the neurovascular bundle can become interposed around its neck. Once the bone has herniated through a soft-tissue defect, longitudinal traction alone tends to tighten the noose of soft tissue around it rather than allow it to slip back, which is why forced closed manipulation so often fails and why many published series ultimately required open reduction.
A single gentle attempt, then open reduction
- Optimise conditions first: adequate analgesia with procedural sedation or general anaesthesia and full muscle relaxation; flex the knee to relax the gastrocnemius so the ankle can be dorsiflexed and the mortise opened.
- One controlled attempt: apply longitudinal traction to re-establish length, then reverse the displacement based on the direction of the dislocation while an assistant provides counter-traction and, where relevant, direct thumb pressure over the prominent talus.
- Do not repeat forceful attempts: each additional forceful manipulation risks further stripping the already tenuous blood supply and worsening the soft-tissue and skin injury. If a single gentle attempt fails, proceed promptly to open reduction, extending the traumatic wound in open injuries or using a standard anteromedial/anterolateral exposure, releasing the interposed structures under direct vision.
If asked why the reduction is difficult, say the talus has buttonholed through the soft-tissue envelope with interposed tendons and neurovascular structures. Attempt one gentle closed reduction under full relaxation, but abandon repeated forceful attempts in favour of prompt open reduction to protect the residual blood supply and the skin.
REDUCEReduction Technique
Hook:REDUCE: Reduction urgent, Emergency within hours, Document neurovascular, Urgent do not delay, CT after reduction, Examine fractures!
Managing the Extruded Talus in the Open Injury
Several of this topic's evidence cards (Karampinas, Veselý) and its reimplant-versus-talectomy controversy hinge on what you physically do with a talus that has been fully extruded from the wound, yet the management sections never operationalise it. The modern principle is clear: do not discard the extruded talus.
Retrieve, clean, reimplant
- Keep the bone: even a grossly contaminated, fully extruded talus should be retained. Discarding it commits the patient to a large bone-stock deficit; retaining it preserves length and bone stock for reimplantation and for any later arthrodesis, and published series report acceptable function after reimplantation with low rates of deep infection when debridement is thorough.
- Aggressive debridement and irrigation: meticulous excision of contaminated and devitalised tissue with copious pulsatile lavage of both the wound and the extruded bone; send tissue for culture; give IV antibiotics on the open-fracture pathway (early broad-spectrum cover, tetanus prophylaxis) with combined orthoplastic planning.
- Immediate reimplantation and stabilisation: replace the talus in its bed and stabilise it. Reported constructs use Kirschner wires or Steinmann pins passed through the calcaneus into the talus and tibia, protected by a spanning calcaneo-tibial external fixator, which holds alignment while the soft-tissue envelope recovers and avoids extensive internal dissection that would further devascularise the bone.
- Then follow the AVN pathway: counsel that infection and osteonecrosis remain difficult to predict at presentation despite optimal care, and that even if AVN later supervenes the retained talus still provides bone stock for salvage arthrodesis.
The single highest-yield operative point in the open injury: reimplant the extruded talus rather than perform primary talectomy. Debride and lavage it thoroughly, culture, replace it, and stabilise with K-wires/Steinmann pins plus a spanning external fixator. Primary talectomy is reserved for the catastrophically contaminated or unreconstructable bone.
Complications
- Incidence
- 50-100%
- Risk Factors
- Prolonged dislocation, complete disruption
- Prevention/Management
- Early reduction, anatomic fixation
- Incidence
- 60-80%
- Risk Factors
- AVN, joint damage
- Prevention/Management
- Anatomic reduction, adequate fixation
- Incidence
- 10-20%
- Risk Factors
- Displacement, inadequate fixation
- Prevention/Management
- Rigid fixation
- Incidence
- 10-20%
- Risk Factors
- Open injury, delayed treatment
- Prevention/Management
- Urgent debridement, antibiotics
AVN
50-100% incidence:
- Cause: Complete disruption of blood supply, prolonged dislocation
- Prevention: Early reduction, anatomic fixation
- Management: Monitor with serial imaging, fusion if collapse
Post-Traumatic Arthritis
60-80% incidence:
- Cause: AVN, joint damage, inadequate reduction
- Prevention: Anatomic reduction, adequate fixation
- Management: Ankle fusion or arthroplasty if severe
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (8-12 weeks)
- ROM: Ankle ROM after cast removal
- PT: Ankle ROM and strengthening
Rehabilitation Protocol
Weeks 0-8:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 8-12:
- CT to confirm healing
- Check for Hawkins sign (AVN assessment)
- Cast removal if healing
- Transition to walking boot
- Progressive weight bearing
Weeks 12-16:
- Full weight bearing
- Progressive activity
- Monitor for AVN
Outcomes and Prognosis
Overall Outcomes
Closed reduction (pure dislocation):
- Success rate: 50-70% (stability, pain relief)
- Functional outcomes: 40-60% return to pre-injury level
- AVN: 50-70% develop AVN
ORIF (with fractures):
- Success rate: 50-70% (union, pain relief)
- Functional outcomes: 40-60% return to pre-injury level
- AVN: 60-80% develop AVN
Open injuries:
- Success rate: 30-50% (union, pain relief)
- Functional outcomes: 30-50% return to pre-injury level
- AVN: 70-90% develop AVN
Long-Term Prognosis
AVN progression:
- With proper treatment: 50-100% develop AVN
- Without treatment: Near 100% develop AVN
- Risk factors: Prolonged dislocation, complete disruption, open injury
Guidelines, Registries & Global Practice
There are no condition-specific society guidelines for total talar dislocation given its rarity; management is extrapolated from talar fracture-dislocation principles and open-fracture guidance. Below is the global picture and how core principles are framed across societies.
Global Epidemiology
- Rarity: Total (pan-talar) dislocation accounts for roughly 3.4% of major talar injuries and is itself a small fraction of all foot/ankle trauma (Johnson et al, 2011).
- Open predominance: A high proportion present open (historically quoted around 70% in case reviews), reflecting the high-energy mechanism.
- Demographics: Predominantly young adults (20-40 years) after motor-vehicle trauma, falls from height or high-energy sport.
- Pooled outcome trend: Across small series, AVN affects a substantial minority to majority of patients; open and prolonged-dislocation injuries do consistently worse.
Guidance Framed by Society / System
- Relevant Principle
- Talar neck fracture timing; urgent reduction of dislocation
- Application to Total Talar Dislocation
- Reduce the dislocation urgently; definitive fixation can be staged once soft tissues allow
- Relevant Principle
- Open-fracture pathway: early IV antibiotics, combined ortho-plastic care, definitive fixation with soft-tissue cover
- Application to Total Talar Dislocation
- Apply directly to open extrusions - antibiotics within 1 hour, joint ortho-plastic planning
- Relevant Principle
- Preserve talar blood supply; avoid tarsal canal/sinus tarsi stripping
- Application to Total Talar Dislocation
- Limit dissection; reduce promptly and stabilise (K-wires + external fixator commonly used)
- Relevant Principle
- Joint-preserving salvage; reimplant rather than discard extruded talus
- Application to Total Talar Dislocation
- Reimplant the talus to retain bone stock even if later fusion is needed
Registry Notes
No arthroplasty or implant registry (NJR, AJRR, AOANJRR, SHAR) tracks this injury, as treatment is reduction and fixation rather than joint replacement. Emerging custom total talar prostheses for talar collapse are reported chiefly from Japanese centres and are not yet captured by mainstream registries; cadaveric data flag anterior instability and dislocation of downsized implants (Sato et al, 2021).
High- vs Limited-Resource Practice
- Well-resourced settings: Immediate ortho-plastic care, external fixation, CT planning, MRI for AVN surveillance, and access to delayed reconstruction/arthrodesis or custom prostheses.
- Limited-resource settings: Emphasis on prompt reduction, K-wire stabilisation and external fixation, vigilant infection control, and arthrodesis as the principal salvage; advanced reconstruction may be unavailable.
Total talar dislocation is a rare but important viva topic. Know that urgent reduction required (within hours, skin necrosis risk), high AVN risk (50-100%), often open injury, ORIF if fractures displaced (50-70% good results), and document neurovascular status before and after reduction. Be prepared to discuss the reduction technique and management of AVN.
Controversies and Areas of Uncertainty
Because the injury is rare and the evidence is limited to small retrospective series, several management questions remain genuinely unsettled.
Older teaching favoured discarding a fully extruded, contaminated talus. Contemporary series (Karampinas, Veselý) show that immediate reimplantation can achieve good function and preserves bone stock for later fusion. Most authors now favour reimplantation even when AVN later supervenes, reserving talectomy for catastrophic contamination or failed salvage.
Closed reduction is often impossible because of buttonholing through soft tissue and interposed structures, and many series report needing open reduction. Repeated forceful closed attempts may worsen soft-tissue and vascular injury, so a single gentle attempt followed by prompt open reduction is widely advocated.
For talar neck fracture-dislocations, evidence (Clare and Maloney) indicates initial displacement - not the timing of definitive fixation - drives osteonecrosis. The dislocation itself should still be reduced urgently to relieve skin and vascular compromise, but definitive bony fixation can be staged once soft tissues recover.
Custom total talar replacement is emerging (predominantly Japanese centres) as a salvage option for talar AVN/collapse, but cadaveric data show anterior instability concerns and downsized implants dislocate. Its role after total dislocation is experimental and not established.
Frequently quoted complication figures (for example "AVN 50-100%") derive from heterogeneous small series with wide confidence intervals and selection bias toward published cases. Quote them as estimates, emphasise the trend (open and prolonged-dislocation injuries do worse), and avoid presenting any single percentage as established fact.
MCQ Practice Points
Q: Why is urgent reduction required for total talar dislocation? A: Skin tension causes necrosis within hours, neurovascular compromise, high AVN risk - Reduce within hours, do not delay for imaging if skin compromised. Document neurovascular status before and after reduction.
Q: What is the AVN risk for total talar dislocation? A: High AVN risk (50-100%) - Complete disruption of blood supply to talus. Prolonged dislocation increases risk. Monitor with serial imaging (Hawkins sign at 6-8 weeks). May require talectomy or fusion if AVN develops.
Q: Are total talar dislocations often open injuries? A: Yes, often open injury - Skin disruption common due to high-energy mechanism. Urgent debridement required. Higher infection risk. Worse outcomes than closed injuries (30-50% good results vs 50-70%).
Q: What is the treatment for total talar dislocation? A: Urgent closed reduction, then ORIF if fractures present - Reduce within hours, document neurovascular status, CT after reduction to assess fractures, ORIF if displaced. Success rate 50-70% with proper treatment.
Q: What are the complications of total talar dislocation? A: AVN (50-100%), post-traumatic arthritis (60-80%), nonunion (10-20%), infection (10-20% in open injuries) - Prevent with early reduction and adequate fixation. Success rate 50-70% with proper treatment.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old patient presents with total talar dislocation after high-energy trauma. Talus is completely dislocated from ankle, subtalar, and talonavicular joints. Skin is tented but intact.”
“A 35-year-old patient has an open total talar dislocation with exposed talus. The examiner asks you to explain your management approach.”
“A trauma radiograph is shown. The examiner asks how you would distinguish a total talar dislocation from a subtalar dislocation, and how you would monitor for avascular necrosis afterwards.”
Key Concepts
- Extremely rare injury (less than 0.1% of dislocations)
- Talus completely dislocated from all articulations
- Urgent reduction required within hours (skin necrosis risk)
- High AVN risk (50-100%)
Classification
- Pure: No fractures, rare - urgent reduction (50-70% good results)
- With fractures: Talar fractures, common - urgent reduction, ORIF (50-70% good results)
- Open: Skin disrupted, common - urgent reduction, debridement (30-50% good results)
- Direction: Lateral (common), Medial (less common), Anterior (rare)
Treatment
- Urgent closed reduction: Within hours, document neurovascular status
- CT after reduction: Assess talar fractures (60-80% have fractures)
- ORIF if fractures displaced: Restore joint congruity (50-70% good results)
- Pure dislocation: Conservative if stable (50-70% good results)
Surgical Technique
- Reduction: Flex knee, traction, reverse deformity
- ORIF talus: Anterior, medial, or lateral approach
- Salvage: Tibiotalar or tibiocalcaneal fusion if AVN
- Verify reduction fluoroscopically
Complications
- AVN: 50-100% (prevent with early reduction, monitor with serial imaging)
- Post-traumatic arthritis: 60-80% (prevent with anatomic reduction)
- Nonunion: 10-20% (prevent with rigid fixation)
- Infection: 10-20% in open injuries (prevent with urgent debridement)
Evidence Base
All evidence below is verified against PubMed. Total talar dislocation is a rare injury, so the literature is dominated by small retrospective series and case reports — no randomised data exist, and stated complication rates carry wide confidence intervals.
Rapid open reduction outperforms talectomy
- 5 patients, all reduced openly, mean follow-up 4.5 years
- AVN in 2 of 5 (40%); no talectomy required
- 3 good and 2 fair clinical results
- Preserve the talus - avoid primary talectomy
Total dislocation is 3.4% of major talar injuries
- Total dislocation = 3.4% of major talar injuries
- Dominant complications: osteomyelitis and AVN
- Evidence base limited to small series and case reports
- Tenuous blood supply underlies the high AVN rate
Immediate reimplantation of the extruded talus
- 9 open extrusions, immediate reimplantation + external fixation
- Mean AOFAS 82.5; 6 of 9 complication-free
- Infection in 2, AVN in 1, arthrodesis in 2
- Reimplantation preserves bone stock even if salvage later needed
Open extrusion: reimplantation with external fixation
- 6 open dislocations, reimplantation + external fixation
- Infection in 2, AVN in 1
- Salvage (arthrodesis/talectomy) required in 2
- Infection and AVN are unpredictable at the time of injury
Initial displacement, not surgical timing, predicts osteonecrosis
- Initial displacement is the strongest predictor of AVN
- Timing of DEFINITIVE fixation does not change AVN risk
- Urgently reduce the dislocation; definitive surgery can be staged
- Avoid tarsal canal/sinus tarsi dissection to spare blood supply
Closed dislocation: early closed reduction can preserve vascularity
- Closed dislocation, no fracture - early closed reduction
- 8 weeks non-weight-bearing, MRI confirmed no AVN
- Return to sport at 18 months with minor symptoms
- Confirm absence of AVN before progressing weight-bearing