Low Transverse Fracture of Distal Humerus | Intra-capsular | High Nonunion Rate
- Definition: A fracture across the condyles of the distal humerus, passing through the olecranon fossa and coronoid fossa.
- Distinction: Unlike supracondylar fractures (extra-capsular), transcondylar fractures are intra-capsular.
- Challenge: The distal fragment is very small ('wafer thin'), making screw purchase difficult.
- Treatment: Primary Total Elbow Arthroplasty (TEA) is favored in independent elderly patients due to high failure rate of ORIF.
- “Transcondylar fractures are intra-capsular (hemarthrosis). Supracondylar are extra-capsular.
- “Dual plating (90-90 or Parallel) is required if ORIF is attempted.
- “Ulnar nerve transposition is controversial but often done during ORIF to prevent tardy palsy.
The distal articular block is often extremely thin, providing poor bone stock for screws. This leads to high pull-out rates with ORIF in osteoporotic bone.
In elderly (greater than 65) low-demand patients, Total Elbow Arthroplasty allows immediate motion and avoids nonunion. "Bag of Bones" (non-op) is reserved for sedentary/demented.
Always document status pre-op. In ORIF, identify and protect. In TEA, transposition is routine.
Supracondylar (the classic paediatric distal-humerus fracture, above the fossae) is extra-capsular. Transcondylar (adult, low, through the fossae) is intra-capsular / intra-articular - the key distinction.
- Bone Quality
- Good
- Treatment
- **ORIF**
- Reason
- Preserve joint, high load tolerance
- Bone Quality
- Osteoporotic
- Treatment
- **TEA (Total Elbow)**
- Reason
- Immediate ROM, avoids ORIF failure
- Bone Quality
- Poor
- Treatment
- **Cast ('Bag of Bones')**
- Reason
- Functional ROM achievable, low complication risk
TRIColumns
Hook:Restoring the Triangle is key.
Overview and Epidemiology
Transcondylar fractures are fractures of the distal humerus occurring at the level of the condyles, passing transversely through the olecranon and coronoid fossae. They are essentially distinct from supracondylar fractures because they are lower and intra-capsular.
- Typically unexpected in adults (unless high energy).
- Bimodal distribution:
- Young males (High energy trauma).
- Elderly females (Osteoporotic falls) - much more common.
- The "Silver Tsunami": Incidence of fragility distal humerus fractures is rising.
Anatomy
The distal humerus is a triangle composed of two columns (Medial and Lateral) supporting the articular block (Trochlea and Capitellum). The columns diverge distally to form the supracondylar ridges. This structure is analogous to a suspension bridge or a tie-beam construct.
- Medial Column: Diverges at an angle of 45 degrees. Terminates in the medial epicondyle. It is easier to plate because it has a broad crest ("Medial Crest").
- Lateral Column: Diverges at an angle of 20 degrees. Terminates in the lateral epicondyle. It is flat posteriorly, accommodating a posterior plate.
- Transcondylar Pattern: Both columns are separated from the articular block at the lowest level, passing through the fossae. This is the thinnest part of the distal humerus ("The Wafer"), often measuring only a few millimeters in AP dimension.
The trochlea and capitellum form a spool-shaped articular surface.
- Trochlea: Covered by hyaline cartilage over 300 degrees of its surface. Acts as a tie-beam connecting the two columns. It has a sulcus that articulates with the ulnar ridge.
- Capitellum: Spheroidal structure articulating with the radial head. It projects anteriorly.
- Olecranon Fossa: Posterior fossa accomodating the olecranon tip in extension.
- Coronoid Fossa: Anterior fossa accomodating the coronoid process in flexion.
- Radial Fossa: Anterolateral fossa accommodating the radial head in flexion.
- Triceps: Inserts on the Olecranon. Pulls the proximal ulna proximally. If the fracture is very low (Transcondylar), the triceps does not de-rotate the distal fragment, but if the fracture involves the epicondyles, the extensors/flexors rotate them.
- Brachialis: Inserts on the Coronoid. Pulls the forearm distally.
- Common Flexor Origin: Medial Epicondyle. Flexes and pronates the medial fragment.
- Common Extensor Origin: Lateral Epicondyle. Extends and supinates the lateral fragment.
- MCL (Ulnar Collateral Ligament): Anterior bundle attaches to the inferior aspect of the medial epicondyle. Essential valgus stabilizer.
- LCL (Lateral Collateral Ligament): Component of the LCL complex (LUCL) attaches to the lateral epicondyle. Essential varus/rotatory stabilizer.
- Capsule: The anterior and posterior capsule is thin but reinforced by the brachialis and triceps respectively.
- Ulnar Nerve: Runs in the cubital tunnel posterior to the medial epicondyle. It is at high risk during fixation of the medial column.
- Radial Nerve: Runs in the spiral groove and pierces the lateral intermuscular septum 10cm proximal to the joint line to enter the anterior compartment.
- Median Nerve: Runs medial to the brachial artery, well protected by the brachialis muscle anteriorly.
- Vascularity: The trochlea is supplied by terminal branches of the ulnar and collateral arteries. The capitellum has a precarious retrograde supply. Transcondylar fractures are intra-capsular and disrupt this intra-osseous supply, relying on capsular vessels for healing.
Why 'Intra-Capsular' Is the Defining Feature (and What It Costs)
The one fact this topic repeats — the transcondylar fracture is intra-capsular, unlike the extra-capsular supracondylar fracture — is not just a labelling point; it drives the diagnosis and the high nonunion rate.
- Hemarthrosis and the fat-pad sign. Because the fracture is inside the capsule, bleeding fills the joint (hemarthrosis) and lifts the fat pads. A posterior fat-pad sign in an adult is pathological and means an intra-articular/intra-capsular fracture until proven otherwise — often the only clue to a minimally displaced transcondylar fracture on plain films.
- A synovial-fluid environment impairs healing. The fracture surfaces bathe in synovial fluid, which dilutes the fracture haematoma and the fibrin scaffold that ordinary (extra-capsular) fractures rely on — a major reason the transcondylar/A3 pattern has a higher nonunion rate than the extra-capsular supracondylar fracture.
- A precarious blood supply to a tiny fragment. The short distal "wafer" fragment has a largely intra-osseous and capsular blood supply that the fracture disrupts, adding poor biology to poor mechanics (thin bone, weak screw purchase).
- The contrast to hold onto. Supracondylar (extra-capsular) — larger fragment, better bone for fixation, better healing; transcondylar (intra-capsular) — thin wafer, hemarthrosis and fat-pad sign, synovial-fluid-impaired healing and a higher nonunion rate. This is why fixation is hard and why primary TEA is attractive in the osteoporotic elderly.
Q: Why does it matter that a transcondylar fracture is intra-capsular rather than extra-capsular like a supracondylar fracture? A: Being inside the capsule means bleeding causes a hemarthrosis (the adult posterior fat-pad sign may be the only clue to an occult fracture), the fracture bathes in synovial fluid that impairs haematoma-driven healing, and the tiny distal fragment has a precarious capsular/intra-osseous blood supply — together explaining the higher nonunion rate and the appeal of primary TEA in poor bone.
Classification Systems
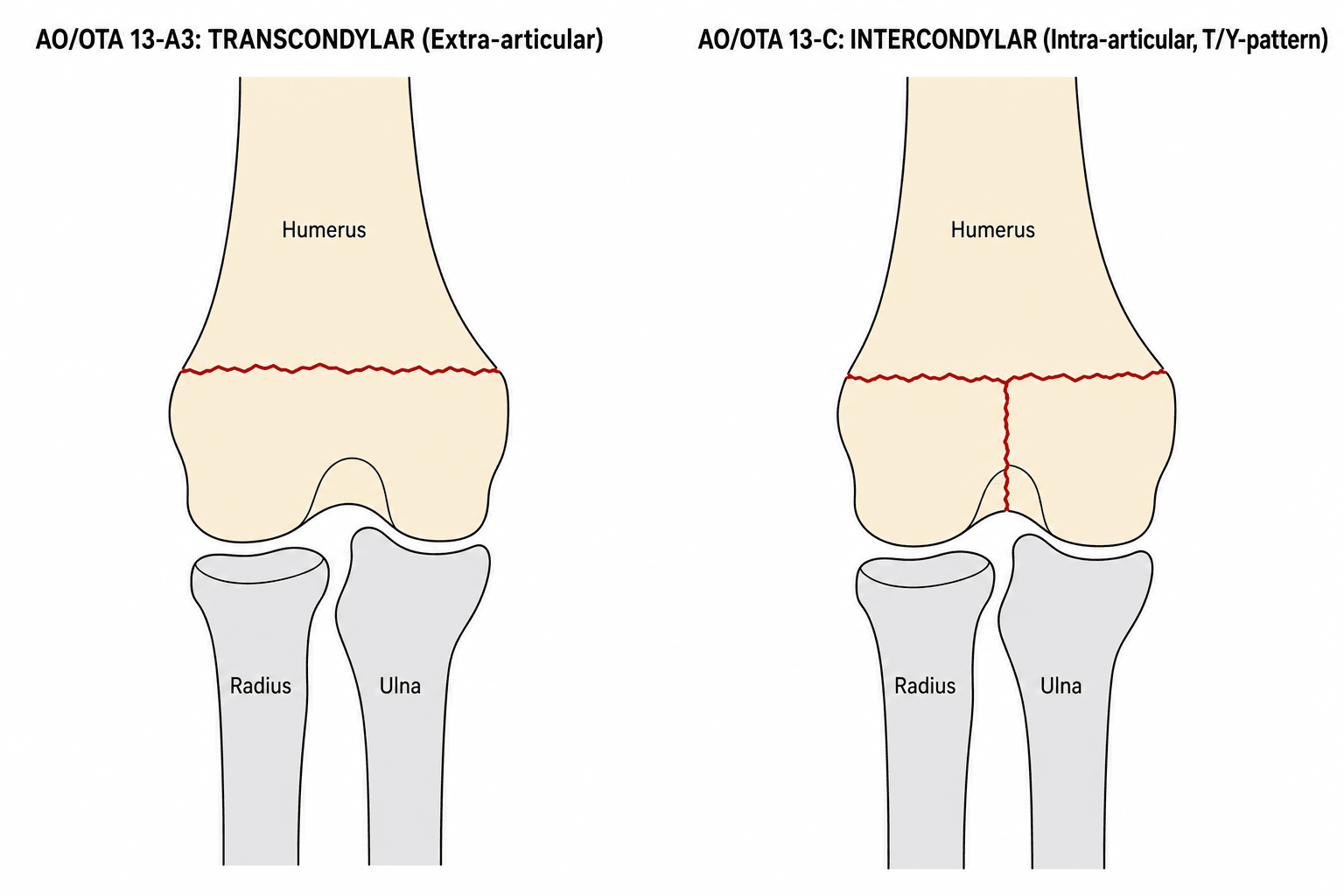
- 13-A: Extra-articular.
- 13-A3: Transcondylar unifocal fracture. (Basically the distal fragment includes the articular surface but the surface itself is not split).
- 13-C: Complete Articular (Intercondylar split). (C3 is Multi-fragmentary).
Type C is intra-articular.
Clinical Assessment
- Fall on outstretched hand (FOOSH) or direct blow.
- Immediate pain, swelling, inability to move.
- Deformity: Gross instability ("floppy elbow").
- Skin: Check for open wounds (posteriorly especially).
- Nerves:
- Ulnar Nerve: Most commonly injured (contusion/stretch). Check intrinsic strength and sensation (little finger).
- Radial Nerve: Check wrist extension/thumb extension.
- AIN: Check "OK sign" (FPL/FDP).
Investigations
- Views: AP and Lateral views of the elbow are standard. Hand and Shoulder views if indicated.
- Signs:
- Fracture Line: Transverse line at the supracondylar level but passing through the fossae.
- Fat Pad Sign: The posterior fat pad is always pathological in adults. If visible, there is a fracture until proven otherwise. The anterior fat pad ("Sail Sign") may be elevated.
- Alignment: Check for varus/valgus Angulation and Rotational Malalignment.
- Drop Sign: Increase in the distance between the ulna and humerus (distraction) may indicate gross instability or ligament injury.
- Traction View:
- Technique: Performed by the surgeon in the ED or under anaesthesia.
- Value: Neutralizes the deforming forces of the triceps/brachialis. Allows better assessment of the comminution and whether the articular block is one piece (Simple A3) or split (C-type).
- Role: Essential for almost all adult distal humerus fractures. Defines the "personality" of the fracture.
- 2D Views:
- Coronal: Shows the "Tie Beam" integrity (trochlea calcified arch).
- Sagittal: Shows the capitellum ("Headless Ghost" due to osteopenia).
- Axial: Best for assessing rotation of the columns.
- 3D Reconstruction:
- Subtract Humerus: Remove the shaft to see the articular surface from above ("Bird's eye view").
- Subtract Ulna/Radius: Remove the forearm to see the Articular surface from below.
- Bone Stock Assessment:
- Look for the "Wafer" - the thin shell of bone between the fracture line and the joint. If this is less than 5mm or very osteopenic, screw purchase is unlikely to be sufficient for ORIF, pushing the decision towards TEA.
- Rarely indicated for acute fractures unless ligament injury (LCL/MCL) is suspected in a simple dislocation masking as a fracture-dislocation.
- May be used for late assessment of Ulnar collateral ligament in high-demand athletes (unlikely in this demographic).
The Functional Arc of Elbow Motion (Why a Stiff Elbow Can Still Work)
The management logic — accepting a "bag of bones" functional nonunion, tolerating lost terminal extension, and aiming to restore motion — rests on Morrey's functional arc.
- Morrey's functional arc. Most activities of daily living are performed within a 100-degree flexion-extension arc (about 30 to 130 degrees) and a 100-degree forearm-rotation arc (about 50 degrees pronation to 50 degrees supination). Motion outside this arc contributes relatively little to everyday function.
- Why this justifies the "bag of bones". A non-operatively treated transcondylar fracture often heals as a functional (fibrous) nonunion or malunion with a reduced but still functional arc — acceptable in a frail, low-demand patient because ADLs live inside that 30-to-130-degree window.
- Why lost terminal extension is tolerated. Losing the last ~30 degrees of extension keeps the patient within the functional arc, whereas losing flexion (needed to reach the face and head) is far more disabling — so rehabilitation and any later release prioritise restoring flexion over a cosmetically full range.
- The surgical corollary. ORIF and TEA both aim to restore this functional arc through early motion — the "Rigid fixation enables early Motion" (ARM) rationale is precisely to keep the elbow moving within, and ideally beyond, Morrey's arc before it stiffens.
Q: What is the functional arc of elbow motion, and why does it justify accepting some stiffness after a transcondylar fracture? A: Morrey's functional arc is roughly 30-130 degrees of flexion-extension and 50-50 degrees of pronation-supination — most ADLs happen within it. A "bag of bones" or a stiff post-ORIF elbow can therefore still be functional if it keeps this arc, which is why losing terminal extension is tolerated but losing flexion is not, and why early motion is the priority.
Differential Diagnosis
The "low transverse distal humerus fracture" in an elderly patient can mimic or coexist with several other injuries. Distinguishing them changes the operative plan.
- Key Distinguishing Feature
- Transverse line through both fossae, intact articular block
- Capsule
- Intra-capsular
- Implication
- Thin distal 'wafer'; ORIF vs TEA decision
- Key Distinguishing Feature
- Line above the fossae, larger distal fragment
- Capsule
- Extra-capsular
- Implication
- More bone for fixation; rare in adults
- Key Distinguishing Feature
- Articular split into the joint (Y/T pattern on CT)
- Capsule
- Intra-capsular
- Implication
- Needs articular reconstruction before column fixation
- Key Distinguishing Feature
- Coronal-plane articular fragment, 'double-arc' sign
- Capsule
- Intra-capsular
- Implication
- Headless screws from front; CT essential
- Key Distinguishing Feature
- Ulnohumeral incongruity, terrible-triad pattern
- Capsule
- Capsuloligamentous
- Implication
- Assess LCL/MCL and coronoid; stability focus
Management Algorithm
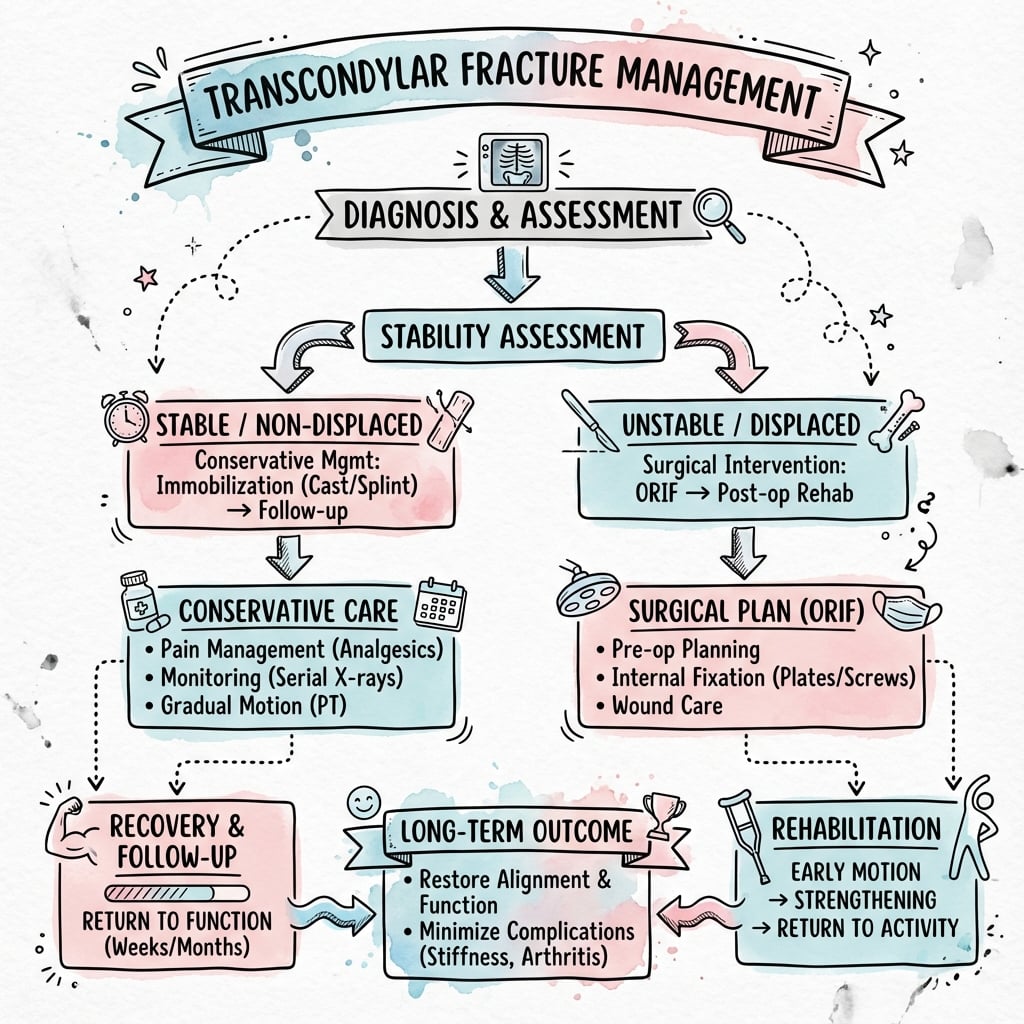
Indication: Undisplaced (rare), or Frail elderly ("Bag of Bones"). Technique: Collar and Cuff aimed at 110 degrees flexion (gravity reduction) for 2 weeks, then gentle mobilization. Outcome: Usually creates a functional nonunion with decent ROM but weak extension. Acceptable for low demand.
Surgical Techniques
Principle: The goal is to convert the complex articular fracture into a simple supracondylar fracture, then fix it to the shaft. This requires perfect articular reduction.
-
Positioning:
- Lateral Decubitus: Arm over a bolster. Allows easy access to the posterior elbow and iliac crest (for graft).
- Prone: Good for visualization but airway access is harder.
- Tourniquet: Sterile tourniquet high on the arm.
-
Approach:
- Posterior Midline: Incision 5cm proximal to olecranon to 5cm distal. Curve around the lateral or medial side of the olecranon tip to avoid scar over the bony prominence.
- Full Thickness Flaps: Raise skin and fascia together to protect cutaneous nerves.
-
Ulnar Nerve Management:
- Identify the nerve in the cubital tunnel before any other dissection.
- Release the cubital tunnel retinaculum (Osborne's ligament).
- Protect with a vessel loop. Do not forcefully retract.
- If the nerve is subluxating or the hardware will be prominent medially, plan for transposition.
-
Deep Exposure (The Window):
- Olecranon Osteotomy (Chevron):
- Technique: Pre-drill the proximal ulna for tension band or screw. Use an oscillating saw to cut 3/4 of the way through the olecranon intra-articularly (at the "bare area" of the sigmoid notch). Complete the cut with an osteotome to create an interdigitating surface ("Chevron").
- Advantage: Best view of the trochlea and capitellum.
- Paratricipital (Triceps-Sparing):
- Technique: Identify the medial and lateral borders of the triceps. Lift the muscle off the posterior humerus.
- Advantage: Preserves extensor mechanism (faster rehab). Good for A-type and simple C-type.
- Olecranon Osteotomy (Chevron):
-
Articular Reduction:
- This is the critical step. You cannot fix the shaft until the block is rebuilt.
- Clear the fracture site of clot and interposed tissue.
- Reassemble the capitellum and trochlea fragments. Use a large reduction clamp.
- Fixation: Use K-wires (temporary) or 3.0/3.5mm headless compression screws (Herbert/Acutrak) or separate cannulated screws. Ensure they are buried in the cartilage.
- Verification: Visually inspect joint congruency.
-
Shaft Fixation (Parallel Plating):
- Construct: 90-90 plating (one posterior, one medial) is biomechanically inferior to Parallel Plating (one medial, one lateral) for varus/valgus stability.
- Medial Plate: Place on the medial crest. It must wrap around the epicondyle.
- Lateral Plate: Place on the posterior aspect of the lateral column (or directly lateral).
- Tying the Arch: Convert the columns back to the shaft.
- Interdigitation: The distal screws from the medial and lateral sides must interdigitate like a zipper within the distal fragment to create a fixed-angle arch.
- Compression: Use the oval hole to compress the articular block to the shaft.
-
Closure:
- Osteotomy Repair: Reduce the olecranon. Fix with a heavy tension band wire (1.2mm wire, 1.6mm K-wires) or a 6.5mm cancellous screw with a washer.
- Nerve: Decide on transposition (subcutaneous). If left in situ, ensure no impingement by the medial plate.
- Drain: Usually placed deep to muscle.
ARMSurgical Goals
Hook:The elbow needs to ARM for movement.
Complications
- Ulnar Neuropathy (15-20%):
- Causes: Contusion at injury, stretch during reduction, hardware irritation (medial plate), scar tissue formation.
- Management: Release in situ or Anterior Transposition.
- Wound Dehiscence:
- Posterior skin is thin. Hematoma can cause tension.
- Prevention: Full thickness flaps, sub-muscular drains, careful closure, prevent flexion greater than 90 degrees if skin under tension.
- Infection (2-6%):
- Higher in revision cases or TEA.
- Management: Debridement. If stable, retain hardware. If unstable/loose, remove and place antibiotic spacer (Spacer to Stage 2 TEA).
-
Stiffness (Arthofibrosis):
- Most common complaint. Loss of terminal extension (30 degrees) is tolerated functionally.
- Prevention: Early Active Motion (The "Motion" in ARM).
- Treatment: Static progressive splinting (Turnbuckle) to Surgical release (capsulectomy).
-
Heterotopic Ossification (HO):
- Risk Factors: Head injury, delayed surgery, forceful passive stretching.
- Prophylaxis: Indomethacin (75mg sustained release daily for 6 weeks) or Radiation (700 cGy single dose).
-
Nonunion (2-10%):
- Risk: Higher in Transcondylar (A3) due to lack of extensive soft tissue attachment to distal fragment.
- Treatment: Revision ORIF with bone graft + Plate augmentation (90-90 or quad plating) OR Conversion to TEA in elderly.
-
Hardware Failure:
- Screw pullout from distal fragment.
- Plate breakage (fatigue failure) due to nonunion.
-
TEA Complications:
- Loosening: Aseptic loosening of stems (10-15% at 10 years).
- Bushing Wear: The polyethylene bushing wears out, causing metal-on-metal contact and osteolysis.
- Triceps Insufficiency: Failure of triceps repair leads to inability to extend against gravity.
SUNComplications
Hook:Don't let the SUN set on a bad elbow.
Postoperative Care
-
Phase 1: Protection (Weeks 0-2):
- Splint: Posterior splint in 60-90 degrees of flexion (to offload triceps repair).
- Edema Control: High elevation ("Hand above heart").
- Motion: Active finger, wrist, and shoulder ROM immediately.
- Imaging: X-ray at 2 weeks to check alignment.
-
Phase 2: Mobilization (Weeks 2-6):
- Wound: Sutures removed.
- Motion: Start Active Assisted ROM (AAROM).
- Gravity Assisted: Supine overhead flexion, Seated gravity extension.
- Turnbuckle Splinting: Consider if stiff at 6 weeks.
- Precaution: NO passive stretching (increases HO risk). NO lifting greater than coffee cup.
-
Phase 3: Strengthening (Weeks 6-12):
- Bone Healing: When callus is visible.
- Motion: Aim for functional arc (30-130).
- Strength: Isometric triceps strengthening. Progressive resistive exercises.
- Bag of Bones: Collar and cuff for comfort, move as tolerated. Ignore the X-ray, treat the patient.
Outcomes/Prognosis
- ORIF: Good to Excellent in 75-80% of young patients. Stiffness is main complaint.
- TEA: 90% 10-year survival. Happiness rate high in elderly.
- Non-Union: 5-10% in ORIF group.
Guidelines, Registries & Global Practice
Global Epidemiology
- Distal humeral fractures account for roughly 2 to 3% of all adult fractures and around one-third of all elbow fractures.
- Distribution is bimodal: high-energy injuries in young men and low-energy fragility fractures in older women. The fragility-fracture share is rising with population ageing ("the silver tsunami").
- Transcondylar (low transverse, OTA 13-A3) patterns are over-represented in the osteoporotic elderly because the fracture follows the thinnest, weakest distal bone.
Side-by-Side Society Positions
- Emphasis
- Column theory and the parallel-plate ("principle-based") construct; restore the triangular distal humerus and enable early motion.
- Emphasis
- Early senior-led decision-making, CT for intra-articular patterns, orthogeriatric co-management of fragility fractures, and timely definitive surgery.
- Emphasis
- No fracture-specific clinical practice guideline; recommendations follow general fragility-fracture and bone-health (secondary prevention) guidance.
- Emphasis
- Endorses primary TEA for the comminuted elderly elbow not amenable to stable fixation, citing the McKee RCT.
Registry & Outcome Signals
- National joint registries that capture elbow arthroplasty (e.g. the Australian, UK and Nordic registries) consistently show that a large share of TEAs are now performed for acute trauma or fracture sequelae rather than inflammatory arthritis.
- Registry and cohort data show higher revision burden in younger, more active recipients and in men — reinforcing TEA as a procedure for low-demand patients.
High- vs Limited-Resource Practice Variation
- Well-resourced settings: CT-based planning, pre-contoured locking plates, headless compression screws, and ready availability of TEA implants and fellowship-trained elbow surgeons.
- Limited-resource settings: Reliance on plain films and traction views, conventional reconstruction/recon plates, and a lower threshold for non-operative ("bag of bones") management where arthroplasty implants, cement or revision capacity are scarce. Orthogeriatric co-management and falls/bone-health pathways may be unavailable.
Controversies & Areas of Uncertainty
- ORIF vs primary TEA threshold: The McKee RCT supports TEA in the comminuted elderly elbow, but the "right" age/activity cut-off is not evidence-defined. Many surgeons now push the boundary upward, attempting fixation in fitter 65 to 75-year-olds because TEA imposes a permanent lifting restriction and revision is difficult.
- Distal humeral hemiarthroplasty (DHH): Proposed for low fractures with an intact or reconstructable column and competent collateral ligaments, avoiding the TEA lifting limit. Evidence remains low-level and implant availability is limited; long-term wear of the native ulna/radial head is unknown.
- Olecranon osteotomy vs triceps-sparing exposure: The osteotomy gives the best articular view but adds an osteotomy non-union/hardware risk (5 to 10% reoperation for hardware). Paratricipital and triceps-reflecting approaches avoid this but limit articular access — choice is fracture- and surgeon-dependent.
- Ulnar nerve: transpose or leave in situ? Vazquez et al found transposition was not protective and may add risk; routine transposition during ORIF is therefore contested. In TEA most surgeons still handle/transpose the nerve to avoid traction.
- Parallel vs perpendicular (90-90) plating: Parallel plating is biomechanically and clinically favoured for comminuted articular patterns, but high-quality comparative clinical trials are lacking, and 90-90 remains acceptable for simpler patterns.
- HO prophylaxis: Routine indomethacin or radiotherapy is not supported for all cases; reserve for high-risk elbows (head injury, delayed/repeat surgery) given GI and union concerns.
MCQ Practice Points
Q: What is the primary contraindication to Total Elbow Arthroplasty for fracture? A: Active Infection or High Physical Demand (heavy laborer). TEA cannot withstand heavy lifting (greater than 1-2kg).
Q: Which nerve is most frequently injured iatrogenically during distal humerus ORIF? A: Ulnar Nerve. Usually due to entrapment or retraction neurapraxia.
Q: Which plating configuration provides the greatest stability for distal humerus fractures? A: Parallel Plating (Medial and Lateral columns).
Q: What is the preferred osteotomy technique for surgical exposure of the distal humerus articular surface? A: Chevron olecranon osteotomy - provides the best visualization of the trochlea and capitellum. Pre-drill before cutting.
Q: What did the McKee multicentre RCT (JSES 2008) conclude about ORIF vs TEA in elderly patients with distal humerus fractures? A: TEA had better 2-year Mayo Elbow Performance Scores and shorter operative time; about 24% of patients randomised to ORIF could not be stably fixed and were converted to TEA intra-operatively.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 78-year-old active lady presents with a comminuted distal humerus fracture (Transcondylar). CT shows 'osteopenia' and 'comminuted articular block'.”
“You decide to perform ORIF on a younger patient. Describe your fixation strategy.”
“An 80-year-old falls and has a swollen elbow. AP and lateral radiographs show a low transverse line with a posterior fat pad sign but the articular detail is unclear.”
Key Features
- Intra-capsular low fracture
- Small distal fragment (wafer)
- Elderly osteoporotic females
- High nonunion rate with ORIF
Treatment Matrix
- Young to ORIF (Parallel Plates)
- Elderly Active to TEA (Total Elbow)
- Elderly Demented to Bag of Bones
- Consider patient function/compliance for TEA vs ORIF
- TEA has a lifelong lifting restriction (~2 kg repetitive, a 'cup of tea')
Surgical Tips
- Olecranon osteotomy for exposure
- Identify Ulnar nerve immediately
- Interdigitate distal screws
- Avoid varus malreduction
Complications
- Stiffness (HO)
- Ulnar neuropathy
- Nonunion / Hardware failure
- Implant loosening (TEA)
Evidence
ORIF vs TEA in Elderly — Landmark RCT
- Multicentre RCT: 42 patients over 65 with displaced intra-articular (OTA 13C) distal humerus fractures randomised to ORIF vs semiconstrained TEA.
- 5 of 21 (24%) randomised to ORIF were converted to TEA intra-operatively because stable fixation could not be achieved.
- TEA had significantly better Mayo Elbow Performance Scores at 2 years (86 vs 73, P=0.015) and 32 minutes shorter operative time.
- Reoperation rates (TEA 12% vs ORIF 27%) did not reach significance.
ORIF vs Primary TEA — Supporting Cohort
- Retrospective comparison of ORIF vs TEA in 24 women over 65 with OTA 13.C2/C3 fractures (12 per group).
- TEA: 11 excellent, 1 good Mayo scores; no revisions. ORIF: 4 excellent, 4 good, 1 fair, 3 poor.
- 3 of 12 ORIF cases (25%) required conversion to TEA.
- Benefit of TEA most pronounced with rheumatoid arthritis, osteoporosis or steroid use.
Parallel-Plate Biomechanics
- Cadaveric biomechanical comparison of double-plate fixation methods for complex distal humeral fractures.
- A medial-and-lateral plate-and-bolt construct gave increased strength and stability in the most unstable fracture pattern.
- Tested compressive stiffness before and after fatigue cycling, then load to failure.
Principle-Based Parallel Plating — Clinical Outcomes
- 34 complex distal humeral fractures (26 AO type C3, 14 open) fixed with two parallel sagittal-plane plates.
- No hardware failure or fracture displacement; primary union in 31 of 32 followed fractures.
- Mean flexion-extension arc 99 degrees, mean Mayo Elbow Performance Score 85.
- Two principles: maximise distal-fragment fixation and make distal screws contribute to supracondylar stability.
The 'Bag of Bones' — Non-Operative Outcomes
- 19 low-demand, medically unwell or older patients (mean age 77) managed non-operatively, mean follow-up 27 months.
- 68% (13 of 19) reported good-to-excellent subjective outcomes; mean Mayo Elbow Performance Index 90.
- Radiographic union in 81% (22 of 27); only one patient was salvaged with later TEA.
- Flexion and extension were modestly worse than the uninjured side but functionally acceptable.
Ulnar Nerve After ORIF
- Retrospective cohort of 69 patients (OTA 13A and 13C) without pre-operative ulnar dysfunction.
- Ulnar nerve dysfunction in 10% immediately post-op and 16% at final follow-up.
- No demographic, injury or treatment factor (including transposition) predicted dysfunction.
- Anterior transposition was NOT protective in this analysis.
TEA for Fracture — 10-Year Survivorship
- 44 TEAs after distal humeral fracture, minimum 10-year follow-up.
- 10-year implant survival 92% (no rheumatoid arthritis) and 76% (rheumatoid arthritis).
- Mean Mayo Elbow Performance Score 90.5; deep infection in 11%, revision or resection in 18%.
- Male sex was the strongest risk factor for revision (HR 12.6).