Most Common Cause of Hip Pain in Children | Self-Limiting | Must Exclude Septic Arthritis | Kocher Criteria Critical
- Most common cause of hip pain in children aged 3-8 years - self-limiting condition
- Kocher criteria differentiate from septic arthritis: fever over 38.5°C, non-weight bearing, ESR over 40, WCC over 12,000
- 0-1 criteria = 3% septic risk (observe), 4 criteria = 99% septic risk (urgent I&D)
- Hip aspiration is gold standard if doubt - WCC under 50,000 with under 75% PMN suggests transient synovitis
- Self-limiting - resolves in 7-10 days with rest and NSAIDs, no long-term sequelae
- “Always exclude septic arthritis first - it's an orthopaedic emergency
- “Kocher criteria are high-yield exam content - know all 4 criteria and probability for each
- “Hip aspiration: Septic arthritis typically over 50,000 WCC with over 75% PMN
- “Transient synovitis: WCC 5,000-15,000 with 40-50% PMN, culture negative
- “Post-viral history common in transient synovitis but not diagnostic
Clinical Imaging
Imaging Atlas



Septic arthritis is orthopaedic emergency - must be excluded in every case. Use Kocher criteria: fever over 38.5°C, non-weight bearing, ESR over 40, WCC over 12,000. 4 criteria = 99% probability septic = urgent I&D. Never miss septic arthritis.
Know all 4 criteria and probabilities: 0-1 = 3% (observe), 2 = 40% (consider aspiration), 3 = 93% (likely I&D), 4 = 99% (urgent I&D). CRP over 20 may be added as 5th criterion in some studies.
If doubt exists, aspirate. Septic: over 50,000 WCC, over 75% PMN, culture positive. Transient: 5,000-15,000 WCC, 40-50% PMN, culture negative. Low WCC does not completely exclude infection - clinical picture matters.
Transient synovitis resolves in 7-10 days with rest and NSAIDs. No long-term sequelae. No need for antibiotics if diagnosis confirmed. Reassurance and symptomatic treatment sufficient.
| Feature | Transient Synovitis | Septic Arthritis |
|---|---|---|
| Age | 3-8 years (peak) | Any age, often younger |
| Fever | Low-grade or absent | High fever over 38.5°C |
| Weight bearing | May weight bear with limp | Refuses all weight bearing |
| ESR | Normal or mildly elevated | Over 40mm/hr |
| WCC | Normal or mildly elevated | Over 12,000 |
| Aspiration WCC | 5,000-15,000 | Over 50,000 |
| Aspiration PMN | 40-50% | Over 75% |
| Treatment | Rest, NSAIDs, observe | Urgent I&D, IV antibiotics |
| Outcome | Resolves 7-10 days, no sequelae | Urgent treatment prevents joint destruction |
FENWKocher Criteria for Septic Arthritis
Hook:FENW - Four criteria, if all present = 99% septic arthritis!
TRANSIENTTransient Synovitis Features
Hook:TRANSIENT - it's temporary, resolves on its own!
SEPTICSeptic Arthritis Aspiration
Hook:SEPTIC - high WCC, high PMN, positive culture, urgent treatment!
Overview and Epidemiology
Differentiation is Key. The exam focus is almost entirely on distinguishing this benign condition from septic arthritis. You must demonstrate a safe, logical approach using Kocher criteria. Missing septic arthritis is a critical fail.
- Peak age: 3-8 years (most common 4-6 years)
- Gender: Slight male predominance (1.5:1)
- Incidence: Most common cause of hip pain in children
- Seasonal: May follow viral illness (winter/spring)
- Recurrence: 5-15% may have recurrent episodes
- Self-limiting: Resolves spontaneously in 7-10 days
- No long-term sequelae: No increased risk of Perthes or other hip pathology
- Recurrence: May recur but each episode resolves
- Prognosis: Excellent - complete resolution expected
Pathophysiology and Mechanisms
Pathogenesis of Transient Synovitis
Mechanism: Benign, self-limiting inflammation of the hip synovium (synovitis).
Etiology: Exact cause unknown, but widely accepted as:
- Post-viral: Often follows upper respiratory tract infection (1-2 weeks prior).
- Post-infectious: Immune-mediated response to recent infection.
- Non-bacterial: Joint fluid is sterile.
Process: Synovial inflammation leads to Joint effusion leads to Capsular distension leads to Pain and limitation of movement (especially internal rotation/abduction).
Classification Systems
Validated Prediction Rule
There is no classification for transient synovitis itself. The relevant "classification" is the Risk Stratification for Septic Arthritis using Kocher Criteria.
| Criteria Count | Septic Arthritis Probability | Recommended Action |
|---|---|---|
| 0 criteria | less than 0.2% | Observe |
| 1 criterion | 3% | Observe / Symptomatic treatment |
| 2 criteria | 40% | Make clinical judgment / Aspirate |
| 3 criteria | 93% | Urgent Aspiration |
| 4 criteria | 99% | Urgent Aspiration & I&D |
The 4 Criteria:
- Fever over 38.5°C
- Non-weight bearing on affected side
- ESR over 40 mm/hr
- WCC over 12,000 cells/mm³
Clinical Assessment
- Onset: Acute or subacute (hours to days)
- Pain: Hip/groin pain, may refer to thigh or knee
- Limp: Refusal to walk or antalgic limp
- Recent illness: URI common 1-2 weeks prior
- Systemic: Child usually appears well
- Vital signs: Usually afebrile or low-grade (under 38.5°C)
- Gait: Antalgic limp (short stance phase)
- ROM: Restriction in Internal Rotation and Abduction.
- Log roll: May be irritable but less severe than septic.
- Tenderness: Anterior joint line tenderness.
Referred Pain: Hip pathology in children frequently presents as knee pain (via obturator nerve). ALWAYS examine the hip in any child presenting with knee or thigh pain. A normal knee exam with an irritable hip suggests hip pathology.
Investigations
Essential Bloods
FBC: WCC usually normal or mildly elevated (under 12,000). Over 12,000 is a Kocher criterion. ESR: Usually normal or mild (under 40). Over 40 is a Kocher criterion. CRP: Usually normal (under 20).
Blood Culture: Not routine if low suspicion. Essential if febrile or septic concern.
Management Algorithm
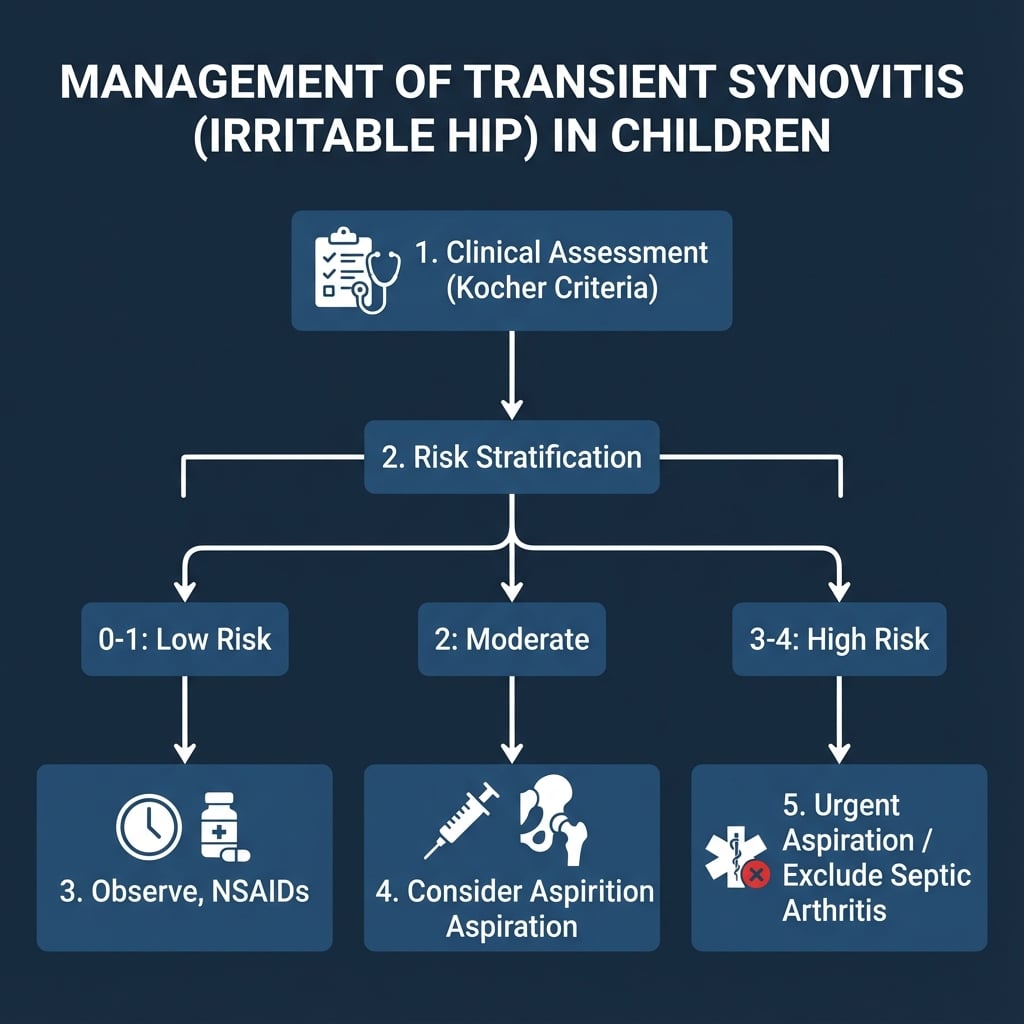
Step-by-Step Management
- Calculate Kocher Score: Assess fever, weight-bearing, WCC, ESR.
- Low Risk (0-1): OBSERVE. Prescribe NSAIDs. Rest. Review in 48 hours.
- Moderate Risk (2): CONSIDER ASPIRATION. Or close observation if clinical picture benign.
- High Risk (3-4): URGENT ASPIRATION. If pus leads to Surgery. If unsure leads to Surgery.
Aspiration Thresholds:
- Transient Synovitis: WCC under 50,000, PMN under 75%, Gram stain negative.
- Septic Arthritis: WCC over 50,000, PMN over 75%, Gram stain positive.
Clinical judgment is required when results are equivocal. Aspiration is the only way to definitively rule out sepsis in high-risk cases.
Detailed Differential Diagnosis
Differentiating Perthes Disease
Perthes disease (Legg-Calvé-Perthes) is the main differential for a limping child in this age group (4-8 years).
| Feature | Transient Synovitis | Perthes Disease |
|---|---|---|
| Onset | Acute (days) | Insidious (weeks/months) |
| Pain | Constant, antalgic | Activity-related, often mild |
| ROM | Restricted in acute phase only | Chronic restriction (Abduction/IR) |
| X-ray | Normal / Effusion | Sclerosis / Fragmentation / Flattening |
| Systemic | Post-viral history | Well child, small stature |
Clinical Pearl: If symptoms persist beyond 2 weeks, it is NOT transient synovitis. Repeat X-ray to look for early Perthes changes (crescent sign).
Surgical Technique
No Surgical Role
Transient Synovitis is a medical condition. There is no role for surgery in the treatment of confirmed transient synovitis.
Role of Surgery is Diagnostic:
- Hip Aspiration: Used to exclude septic arthritis.
- Arthrotomy: Only if septic arthritis is confirmed or strongly suspected (pus on aspiration).
Surgery is otherwise not part of the management algorithm for this self-limiting condition.
Complications
Complications and Pitfalls
| Complication | Risk | Mitigation |
|---|---|---|
| Missed Septic Arthritis | Critical | Apply Kocher criteria strictly |
| Recurrence | 5-15% | Parent education, reassure it's benign |
| Perthes Disease | Unrelated | Follow-up X-ray if symptoms persist over 2 weeks |
| Coxa Magna | Rare | Usually resolves (overgrowth from hyperemia) |
Coxa Magna: Mild enlargement of the femoral head can occur due to increased blood flow (hyperemia) from synovitis. It is asymptomatic and usually resolves or persists without consequence. It is NOT Perthes disease.
Follow-Up Protocol
Transient Synovitis Follow-Up
Exclude septic arthritis. Start NSAIDs and rest.
Phone or clinical review. Child should be improving. If worse leads to Red Flag (Re-evaluate for Sepsis/Perthes).
Symptoms should largely resolve. Return to activity as tolerated.
Only needed if symptoms recur or persist. Consider X-ray to exclude Perthes (rare presentation).
Outcomes and Prognosis
Long-Term Outlook
Function: Excellent. 100% return to sports and activities.
Bone Health: No increased risk of osteoarthritis or avascular necrosis (differentiates from Perthes).
Recurrence: Can happen, usually milder. Treat same way (exclude sepsis, NSAIDs).
Evidence Base
Kocher Criteria — Original Prediction Algorithm
- Retrospective review of an acutely irritable hip cohort at a tertiary children's hospital (1979-1996)
- Four independent multivariate predictors: history of fever, non-weight-bearing, ESR at least 40 mm/hr, serum WCC over 12,000/mm³
- Predicted probability of septic arthritis: under 0.2% (0 predictors), 3.0% (1), 40.0% (2), 93.1% (3), 99.6% (4)
- Excellent ROC performance for combined predictors despite overlap of individual variables
External Validation of Kocher Criteria
- 165 hips (1992-2000) — applied the original Kocher algorithm at an independent institution
- With all 4 predictors present, probability of septic arthritis was only 59% (vs 99.6% in Kocher's cohort)
- Best local model used 3 variables (fever, WCC over 12,000, previous health-care visit) — 71% probability when all present
- Neither the original nor the local algorithm performed reliably outside its derivation centre
C-Reactive Protein as a Predictor (Prospective)
- Prospective study of 53 children undergoing hip aspiration for suspected septic arthritis
- CRP was the only factor strongly and independently associated with septic arthritis on multivariate analysis
- Fever (oral temperature over 38.5°C) was the single best predictor; CRP over 20 mg/L a strong independent risk factor
- Probability of septic arthritis: 83% (3 factors), 93% (4 factors), 98% (5 factors)
Transient Synovitis — Long-Term Characterisation
- 30-year retrospective review: 497 episodes in 475 children
- Femoral head measurements at 6-month follow-up showed no significant dimensional change
- Legg-Calvé-Perthes disease developed in 3 children (2.5%); recurrent synovitis (benign course) in 19
- Authors recommend radiographic assessment at 6 months after the initial episode
Ultrasound Cannot Differentiate Septic from Transient
- 154 children (81 septic arthritis, 73 transient synovitis); ultrasound correlated with final diagnosis in 127
- Ultrasound sensitivity 86.4%, specificity 89.7%, PPV 87.9% for septic hip
- Ultrasound detects minimal effusion but cannot safely distinguish septic arthritis from transient synovitis
- Worse outcomes with treatment delayed over 4 days and with false-negative scans
Kingella kingae as a Leading Cause of Osteoarticular Infection
- Prospective study; specific real-time PCR applied to culture-negative osteoarticular specimens in young children
- Culture alone identified a pathogen in 45%; adding PCR raised documentation to 66%
- Kingella kingae was the leading pathogen (45%), ahead of Staphylococcus aureus (29%)
- Standard cultures substantially under-detect K. kingae
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 4-year-old boy presents with a limp. He had a viral URTI last week. He is afebrile and happy. Examination shows restricted internal rotation. What is your approach?”
“A 3-year-old girl presents refusing to walk. Temp 38.6. CRP 40. WCC 16. Ultrasound shows effusion. How do you manage this patient?”
“A 6-year-old boy returns 4 weeks after a diagnosis of 'transient synovitis'. He is still limping intermittently. He is afebrile. What is your differential?”
“A 7-year-old boy presents with a 4-week history of mild groin pain. He has been treated as 'transient synovitis' by his GP but is not improving. X-ray shows 'mild flattening' of the femoral head. Discuss.”
MCQ Practice Points
Q: A child has 3 out of 4 Kocher criteria. What is the predicted probability of septic arthritis? A: 93%.
- 0 criteria: less than 0.2%
- 1 criterion: 3%
- 2 criteria: 40%
- 3 criteria: 93%
- 4 criteria: 99%
Q: You aspirate a hip. The WCC is 8,000 with 45% PMNs. What is the diagnosis? A: Transient Synovitis. Septic arthritis typically has WCC over 50,000 and over 75% PMNs.
Q: What is the most common organism causing septic arthritis in the 3-8 year age group? A: Staphylococcus aureus. (Kingella kingae is increasing, especially in younger children under 4 years).
Q: What is Waldenstrom's sign? A: Widening of the medial joint space (over 2mm asymmetry) on plain X-ray. It indicates hip effusion (synovitis or septic).
Q: Does transient synovitis increase the risk of Perthes disease? A: No. Evidence suggests no link. However, Perthes can initially present similar to transient synovitis.
Guidelines, Registries & Global Practice
- Most common cause of atraumatic hip pain and limp in children worldwide
- Annual incidence estimated at roughly 0.2% of children; lifetime risk up to 3%
- Peak age 3-8 years (commonly 4-6); male predominance approximately 1.5-2:1
- Preceding viral illness (often URTI) reported in a substantial minority
- Recurrence in roughly 4-15% of children across series
- No single registry exists (non-implant, self-limiting condition)
- Kocher / Caird prediction tools are referenced internationally (AAOS, BOA, European centres)
- Universal principle: septic arthritis must be actively excluded before labelling a hip "transient synovitis"
- Antibiotic stewardship: narrow-spectrum agents (e.g. flucloxacillin / first-generation cephalosporin) reserved for proven or strongly suspected infection
| Source / Region | Risk Stratification | Imaging Emphasis | Notable Point |
|---|---|---|---|
| AAOS / North America | Kocher + CRP (Caird) | Ultrasound to confirm effusion, guide aspiration | Low threshold for aspiration when 3-4 predictors |
| BOA / UK practice | Clinical + inflammatory markers | Ultrasound first-line for effusion | MRI if osteomyelitis or pyomyositis suspected |
| European centres | CRP-weighted models | Ultrasound; PCR for Kingella in young children | Strong emphasis on K. kingae molecular detection |
| Limited-resource settings | Clinical + basic bloods | X-ray; ultrasound where available | Aspiration and empirical cover prioritised when sepsis cannot be excluded |
Where ultrasound and rapid inflammatory markers are unavailable, the safe default shifts toward aspiration and exclusion of sepsis rather than observation, because the cost of a missed septic hip is joint destruction. Conversely, in well-resourced settings serial examination, ultrasound and CRP allow more confident observation of low-risk children.
Kingella kingae is fastidious and frequently missed on standard culture. In a young child (under 4 years) with a septic-appearing but culture-negative hip, request K. kingae PCR (or inoculate aspirate into blood-culture bottles). Molecular methods have repositioned it as the leading osteoarticular pathogen in this age group.
Controversies & Areas of Uncertainty
The Kocher probabilities (under 0.2% to 99.6%) were not reproduced on external validation (Luhmann: 59% for 4/4). The tools stratify risk but should never override clinical judgment or replace aspiration when suspicion is high.
Caird's prospective data suggest CRP may be the single strongest individual predictor, yet the original four-variable rule remains the most quoted. Whether CRP should replace or supplement ESR/WCC is unsettled.
Routine early radiographs in a classic, rapidly settling case have low yield. There is no consensus on universal first-visit X-ray; most reserve it for atypical, persistent (over 2 weeks) or recurrent presentations to exclude Perthes.
A causal link between transient synovitis and later Perthes is not established; historical series report a small (around 2-3%) subsequent Perthes rate, likely reflecting early Perthes initially mislabelled rather than true progression.
Exam Cheat Sheet
Diagnosis
- Age 3-8 years, acute limp
- Diagnosis of Exclusion
- Must exclude Septic Arthritis
- Exclude Perthes (X-ray)
Kocher Criteria
- Fever over 38.5
- Non-Weight Bearing
- ESR over 40
- WCC over 12
- 4/4 = 99% Septic
Management
- Rest + NSAIDs
- Observe if Low Risk
- Aspirate if High Risk
- NO Antibiotics
Aspiration
- Septic: WCC over 50k, PMN over 75%
- Transient: WCC under 15k
- Culture is definitive
Prognosis
- Self-limiting (7-10 days)
- Recurrence 5-15%
- No long term sequelae
- Does NOT cause Perthes