Reversible Lysine Analogue | Reduces Blood Loss | Safe VTE Profile | Cost-Effective
- Mechanism: Reversible competitive inhibitor of plasminogen activation, preventing fibrin degradation
- Evidence: Level I evidence in TKA, THA, trauma, spine surgery for reducing blood loss
- Safety: No increased VTE risk in surgical meta-analyses at therapeutic doses
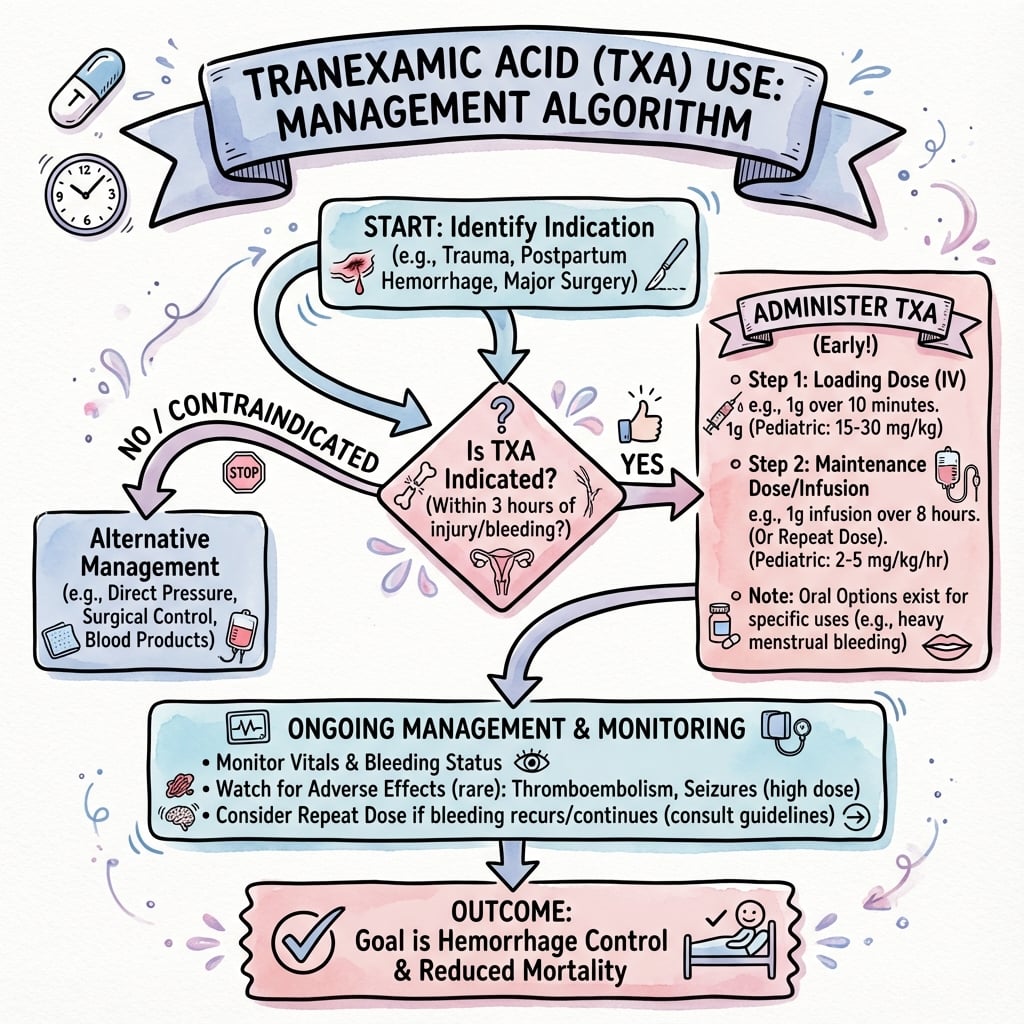
- Timing: Most effective when given pre-incision (15-20mg/kg IV bolus); in trauma within 3h of injury
- Cost-effectiveness: Reduces transfusion rates and hospital costs significantly
- “TXA binds reversibly to plasminogen, blocking lysine-binding sites
- “CRASH-2 trial established use in trauma (1g bolus within 3h, then 1g over 8h)
- “No clinically significant difference between IV, topical, or combined routes in TJA
- “Contraindications: active thromboembolic disease, renal impairment (adjust dose), seizure history
TXA is a synthetic lysine analogue that competitively and reversibly inhibits plasminogen activation. This prevents conversion of plasminogen to plasmin, the enzyme responsible for fibrin degradation. The result is stabilization of formed clots.
No increased VTE risk demonstrated in surgical meta-analyses and the CRASH-2 trauma trial (over 20,000 patients) at therapeutic doses. In the POISE-3 noncardiac surgery trial, the cardiovascular composite was similar but formal noninferiority was not met, so standard VTE prophylaxis is always continued.
Maximum efficacy when given pre-incision or within 3 hours of injury (CRASH-2). Surgical fibrinolysis peaks during and immediately after surgery. Late administration (after 3h post-trauma) may increase mortality.
IV, topical, and combined routes show similar efficacy in TJA. Choose based on patient factors and surgeon preference. Topical reduces systemic exposure in patients with relative contraindications to IV use.
At a Glance
Tranexamic acid (TXA) is a synthetic lysine analogue that competitively inhibits plasminogen activation, stabilizing formed clots and reducing blood loss by 30-50% in joint arthroplasty. Standard dosing is 15-20 mg/kg IV pre-incision or 2-3g topical intra-articular. The CRASH-2 trial (20,211 trauma patients) established efficacy in trauma (1g bolus within 3 hours, then 1g over 8 hours) with no increased VTE risk. Surgical meta-analyses confirm no clear increase in DVT/PE at therapeutic doses. IV, topical, and combined routes show similar efficacy in TJA. Contraindications include active thromboembolic disease, renal impairment (dose adjustment needed), and seizure history. Timing is critical, as administration after 3 hours post-trauma may increase mortality.
CLOTCLOT - Mechanism and Effect
Hook:TXA helps blood CLOT by stabilizing fibrin meshwork
SAFESAFE - Safety Profile Points
Hook:TXA is SAFE when used appropriately with attention to contraindications
ROUTESROUTES - Administration Options
Hook:Multiple ROUTES available - choose based on patient and procedure
BENEFITSBENEFITS - Clinical Outcomes
Hook:The BENEFITS of TXA are multiple and well-established
Pharmacology and Mechanism
Tranexamic acid (TXA) is a synthetic derivative of the amino acid lysine that acts as a competitive inhibitor of fibrinolysis. Its mechanism and pharmacokinetics make it ideal for perioperative blood conservation.
Chemical structure:
- Molecular formula: C8H15NO2
- Systematic name: trans-4-(aminomethyl)cyclohexanecarboxylic acid
- Lysine analogue: Structurally similar to lysine, allowing competitive binding
Mechanism of action:
-
Competitive inhibition of plasminogen activation:
- TXA binds reversibly to lysine-binding sites on plasminogen
- Prevents plasminogen binding to fibrin
- Blocks conversion of plasminogen to plasmin by tissue plasminogen activator (tPA)
-
Direct plasmin inhibition:
- At higher concentrations, TXA also inhibits plasmin directly
- Prevents degradation of fibrin clot into fibrin degradation products (FDPs)
-
Stabilization of fibrin meshwork:
- Formed clots are protected from premature breakdown
- Surgical hemostasis is more effective and durable
Surgical trauma activates fibrinolysis through tissue damage releasing tPA and contact with artificial surfaces (especially cardiopulmonary bypass). This physiologic response can be excessive, leading to microvascular oozing. TXA counteracts this by stabilizing clots at the surgical site.
Pharmacokinetics:
- Absorption: Rapid after IV administration, oral bioavailability approximately 45%
- Distribution: Low protein binding (3%), distributes into extravascular space including joint fluid
- Peak plasma concentration: 1 hour after oral dose, immediate after IV bolus
- Half-life: 2-3 hours (prolonged in renal impairment)
- Excretion: 90% excreted unchanged in urine by glomerular filtration
- Effective concentration: 10-15 micrograms/mL for antifibrinolytic effect
- Duration: Antifibrinolytic effect lasts 3-6 hours after single dose
Low-moderate doses (10-25mg/kg): Effective antifibrinolytic action without significant adverse effects.
High doses (over 100mg/kg): Risk of seizures increases, especially in cardiac surgery or with renal impairment. No additional hemostatic benefit.
Optimal dosing: 15-20mg/kg IV bolus or 1-2g flat dose provides therapeutic levels for typical orthopaedic procedures.
Investigations
Preoperative Assessment for TXA Use
Before TXA administration:
- Renal function (eGFR) - dose adjustment if impaired
- History of thromboembolic disease (DVT, PE, stroke, MI)
- Current anticoagulation or antiplatelet therapy
- Seizure disorder history
- Pregnancy/breastfeeding status
No routine coagulation testing required for standard use.
Evaluate risk-benefit:
- Active VTE or recent thromboembolic event (within 6 months)
- Severe renal impairment (eGFR less than 30)
- History of seizures or intracranial hemorrhage
- Known hypersensitivity to TXA
- Subarachnoid hemorrhage (controversial)
Most orthopaedic patients are candidates for TXA use.
Preoperative Laboratory Assessment
Laboratory Testing Before TXA
Renal Function and Dose Adjustment
- Dose Adjustment
- Full dose (15-20mg/kg)
- Rationale
- Normal clearance
- Dose Adjustment
- Consider reduced dose (10-15mg/kg)
- Rationale
- Moderately prolonged half-life
- Dose Adjustment
- Reduce dose by 50% (7.5-10mg/kg)
- Rationale
- Significantly prolonged half-life
- Dose Adjustment
- Avoid or single reduced dose
- Rationale
- Accumulation risk, seizure risk
For routine TXA use in TKA/THA:
- No special investigations required beyond standard preoperative workup
- eGFR is the key value to check for dose adjustment
- Routine coagulation testing NOT needed unless on anticoagulation
- TXA does NOT require monitoring of coagulation parameters postoperatively
Management
TXA Dosing Protocols by Procedure
Standard TXA Dosing Protocols in Orthopaedic Surgery
Route Selection
Advantages:
- Systemic effect (effective for all surgical sites)
- Predictable plasma levels
- Standard approach in most institutions
- Evidence-based with extensive RCT data
Dose: 15-20mg/kg bolus or 1-2g flat dose
Timing: Ideally 10-15 minutes before incision
Advantages:
- Minimal systemic absorption
- High local concentration at surgical site
- Preferred if relative contraindication to systemic use
- No clear difference in efficacy from IV in TKA/THA
Dose: 2-3g in 50-100mL saline
Technique: Intra-articular with 5-10 min dwell time
Decision Algorithm for TXA Administration
Confirm eligibility: check renal function (eGFR), review contraindications (active VTE, seizure history), complete standard preoperative workup, and document the TXA plan.
Choose route:
- Standard patient: IV or topical (equivalent efficacy)
- Renal impairment: Topical preferred, or reduced IV dose
- Seizure history: Topical preferred
- Patient preference: Either route acceptable
Optimise timing:
- IV bolus: 10-15 minutes before skin incision
- Topical: applied at end of procedure before closure
- Combined: IV pre-incision + topical at closure (no clear added benefit in most studies)
Consider repeat dose if: procedure over 3 hours (half-life 2-3 hours), ongoing significant blood loss, or revision/complex reconstruction. Dose: half the initial dose, or full dose at 3 hours; do not exceed about 3g total IV.
Surgical meta-analyses and the CRASH-2 trial show no clear increase in VTE with TXA. Continue standard VTE prophylaxis: mechanical (IPC, TED stockings), chemical (LMWH, rivaroxaban, aspirin per protocol), and early mobilisation.
For exams, remember:
- Standard dose: 15-20mg/kg IV or 1-2g flat dose
- Timing: pre-incision for IV, at closure for topical
- No clear difference between IV and topical efficacy in TJA
- No clear increase in VTE risk - continue standard prophylaxis
- Consider repeat dose if procedure greater than 3 hours
Surgical Technique
TXA Administration Techniques
Standard protocol:
- Confirm patient eligibility (no contraindications) during the WHO checklist
- Prepare TXA: 15-20mg/kg or 1-2g in 100mL saline
- Administer as slow IV infusion over 10 minutes
- Complete 10-15 minutes before skin incision
- Document dose, timing and route in the anaesthetic/operative record
Important: Slow infusion reduces hypotension risk.
Standard protocol:
- Prepare solution: 2-3g TXA in 50-100mL normal saline
- Achieve mechanical surgical haemostasis first
- Instill into joint cavity or wound, ensuring contact with bleeding surfaces
- Maintain a dwell time of 5-10 minutes
- If a drain is used, clamp during the dwell period then release
Timing: at end of procedure before closure.
Procedure-Specific Considerations
TXA Technique by Procedure
For exams:
- IV route: slow infusion over 10 min, 10-15 min pre-incision
- Topical: 2-3g in 50-100mL saline, 5-10 min dwell time
- Achieve surgical haemostasis BEFORE topical application
- Document dose, timing, route in anaesthetic/operative records
- Either route is acceptable - no clear difference in efficacy in TJA
Complications and Safety
Overview of TXA Safety
Key evidence:
- Over 10,000 surgical patients in the Ker meta-analysis; over 20,000 in CRASH-2
- No clear increase in VTE at therapeutic doses
- Rare serious adverse events at orthopaedic doses
TXA is among the safest perioperative medications when used appropriately.
Most are minor or rare:
- Nausea/vomiting/diarrhoea (especially rapid IV or oral)
- Hypotension (with rapid IV administration)
- Seizures (high doses, renal impairment)
- Visual disturbance (extremely rare, retinal toxicity with prolonged use)
Risk increases with dose and renal impairment.
Thromboembolic Safety
TXA does not clearly increase VTE risk at therapeutic doses.
- CRASH-2 (20,211 patients): no increase in vascular occlusive events (DVT, PE, stroke, MI)
- Ker BMJ surgical meta-analysis (129 trials): no clear increase in DVT, PE, MI or stroke
- POISE-3 noncardiac surgery: cardiovascular composite similar (14.2% vs 13.9%), but formal noninferiority was NOT met, so vigilance and standard prophylaxis remain essential
Mechanism of safety: TXA inhibits fibrinolysis, not coagulation initiation. It protects formed clots rather than promoting new clot formation. Continue standard VTE prophylaxis.
Seizure Risk
Seizure Risk with TXA
Mechanism: at high plasma concentrations (over about 80-100 micrograms/mL) TXA acts as a GABA-A receptor antagonist, lowering seizure threshold. Orthopaedic doses rarely reach these levels. If a TXA-related seizure occurs: stop the infusion, protect the airway, give a benzodiazepine, check glucose, document, and avoid future TXA use.
For exams:
- TXA does NOT clearly increase VTE risk (CRASH-2, Ker meta-analysis)
- Seizure risk increased with high doses (over 100mg/kg) or renal failure
- Standard orthopaedic doses (15-20mg/kg) have an excellent safety profile
- Slow IV infusion prevents hypotension
- Continue standard VTE prophylaxis - TXA is not a contraindication
Postoperative Care
Postoperative Monitoring After TXA
Standard postoperative care:
- No additional monitoring required for TXA specifically
- Standard wound observation
- Hemoglobin check Day 1 (routine)
- VTE prophylaxis as per protocol
TXA does not require special postoperative care.
If a surgical drain is used:
- If topical TXA instilled, clamp for 5-10 min (or up to 1-2 hours per protocol)
- Unclamp and allow free drainage; monitor output as usual
- Remove drain per standard protocol (typically 24-48 hours)
Drain management is not significantly altered by TXA.
Transfusion and VTE Prophylaxis
Continue standard VTE prophylaxis (mechanical plus chemical, with extended chemical prophylaxis for TKA/THA) and standard restrictive transfusion thresholds (Hb less than 70 g/L for most patients; 70-80 g/L if symptomatic or cardiac disease). TXA reduces but does not eliminate transfusion need (transfusion rate roughly 2-5% with TXA versus 15-25% without).
Wound Care and Rehabilitation
Standard wound care applies; TXA typically reduces wound haematoma. Rehabilitation and mobilisation are unchanged, with early mobilisation Day 0 or Day 1. If excessive drainage or haematoma develops, the TXA effect has usually worn off (half-life 2-3 hours) and the priority is to assess for surgical bleeding rather than routinely re-dose.
For exams:
- TXA does not require additional postoperative monitoring
- Continue standard VTE prophylaxis (no clear increase in VTE risk)
- Same restrictive transfusion thresholds apply (Hb greater than 70 g/L)
- Rehabilitation and mobilisation unchanged
- Drain management: if topical used, clamp for dwell time then standard care
Outcomes and Cost-Effectiveness
Primary Outcomes
Consistent across studies:
- TKA: 30-50% reduction in total blood loss
- THA: 30-40% reduction in total blood loss
- Absolute reduction: approximately 300-500 mL per procedure
Clinical significance: reduces anaemia, transfusion need and associated complications.
Dramatic effect:
- Transfusion rate without TXA: 15-25%
- Transfusion rate with TXA: 2-5%
- The Ker surgical meta-analysis reported transfusion reduced by about one third (RR 0.62)
Cost impact: significant savings from reduced transfusion.
Key Outcome Metrics
TXA Outcomes in Total Joint Arthroplasty
Cost-Effectiveness
TXA is one of the most cost-effective interventions in orthopaedic surgery and is generally cost-saving (a dominant strategy that both saves money and improves outcomes):
- TXA cost: very low, of the order of a few units of currency per gram (roughly 10-30 per patient)
- Transfusion cost: a single unit costs hundreds (including testing, administration and monitoring), plus the cost of transfusion-related complications
- Net effect: reduced transfusion of the order of 15-20% absolute, NNT roughly 5-10 to prevent one transfusion, with net savings of several hundred per patient
- Indirect benefits: shorter length of stay, fewer transfusion-related complications, reduced blood-bank burden
For exams, remember:
- Blood loss reduction: 30-50% in TKA/THA
- Transfusion reduction: roughly one third to two thirds (from 15-25% to 2-5%)
- VTE risk: no clear increase (CRASH-2 and surgical meta-analyses)
- Cost: very low per dose, saves several hundred per patient
- Safety: excellent, seizure risk only at high doses
Evidence Base Across Orthopaedic Subspecialties
Total Knee Arthroplasty (TKA)
- Network meta-analysis and multiple RCTs demonstrate consistent 30-50% reduction in blood loss and a fall in transfusion from roughly 20% to under 5%
- No clear increase in symptomatic VTE
- Routes: IV (15-20mg/kg pre-incision), topical (2-3g in 50-100mL saline, 5-10 min dwell), combined (no clear added benefit), oral (1-2g pre-op, emerging) - none clearly superior
- Outcomes: mean blood-loss reduction 300-500mL; no difference in infection, wound complications or thrombosis
No clinically significant difference between topical and IV TXA in RCTs and network meta-analyses. Choose IV for systemic effect and convenience, or topical if the patient has a relative contraindication to systemic use (e.g. seizure disorder).
Total Hip Arthroplasty (THA)
- 30-40% blood-loss reduction across approaches (posterior, lateral, anterior); transfusion reduced from 15-25%
- Safe in cemented and uncemented techniques; effective in revision with higher doses considered
- Dosing: 1.5-2g IV bolus or 15-20mg/kg; topical 2-3g into acetabulum/femoral canal before final component insertion; consider repeat for prolonged procedures
Key Evidence Summary
CRASH-2 Trial - Trauma
- All-cause mortality reduced 16.0% to 14.5% (RR 0.91)
- Death from bleeding reduced 5.7% to 4.9% (RR 0.85)
- No increase in vascular occlusive events
- Benefit only when given within 3 hours of injury
TXA Safety and Efficacy in Surgery - Ker Meta-Analysis
- Transfusion reduced by about one third (RR 0.62)
- No clear increase in DVT (RR 0.86) or PE (RR 0.61)
- No clear increase in MI (RR 0.68) or stroke (RR 1.14)
- Thromboembolic effect estimates have wide confidence intervals
Route Comparison in TKA - Fillingham Network Meta-Analysis
- 67 studies, primary TKA
- Topical, IV and oral all superior to placebo
- No formulation, dose or timing clearly superior
- Moderate evidence favours pre-incision IV
Route Comparison in THA - Fillingham Network Meta-Analysis
- 34 studies, primary THA
- All routes superior to placebo
- No route clearly superior
- Higher/repeat dosing no clear benefit
POISE-3 - TXA in Noncardiac Surgery
- 9535 noncardiac surgery patients
- Composite bleeding 9.1% vs 11.7% (HR 0.76)
- Cardiovascular composite 14.2% vs 13.9% (HR 1.02)
- Formal cardiovascular noninferiority not established
CRASH-3 - TXA in Traumatic Brain Injury
- 12,737 TBI patients
- Head-injury death 18.5% vs 19.8% (RR 0.94)
- Benefit in mild-to-moderate TBI (RR 0.78)
- No increase in seizures or vascular occlusive events
Society Guideline - TXA in Primary Total Joint Arthroplasty
- Strong recommendation for TXA in primary TJA
- No route/dose/timing clearly superior
- Concordant with NICE and WHO guidance
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 75-year-old woman with eGFR of 25 mL/min/1.73m2 is scheduled for TKA. How do you manage TXA in this patient?”
“A 65-year-old woman is scheduled for bilateral TKA under single anesthetic. How would you manage TXA dosing for this patient?”
“Describe your technique for administering tranexamic acid during total knee arthroplasty.”
“A colleague expresses concern about using TXA in patients undergoing TKA, citing thromboembolic risk. How do you address this concern?”
“You are called to the ward on the evening of surgery. Your patient who had TKA with TXA has 600mL in the drain over 4 hours and is complaining of knee pain and swelling. How do you manage this?”
“What is the evidence for using tranexamic acid in total knee arthroplasty, and should it be standard of care?”
MCQ Practice Points
Q: What is the mechanism of action of tranexamic acid (TXA) in reducing surgical blood loss?
A: TXA competitively inhibits plasminogen activation by binding to lysine-binding sites on plasminogen. This prevents plasmin from degrading fibrin clots (antifibrinolytic). TXA stabilizes formed clots rather than promoting new clot formation. It does NOT clearly increase thrombogenicity or VTE risk in orthopaedic surgery populations based on large trials (CRASH-2) and surgical meta-analyses.
Q: What is the recommended dosing regimen for TXA in primary total knee arthroplasty?
A: IV TXA 1-2g (or 15-20mg/kg) given before tourniquet inflation or skin incision, with an optional repeat dose at closure or 3 hours later. Topical TXA (2-3g in 50-100mL saline) applied before closure is an alternative with equivalent efficacy and lower systemic absorption. Network meta-analyses show no route, dose or timing is clearly superior. Avoid exceeding about 3g total IV.
Q: What is the expected reduction in blood loss and transfusion risk with TXA use in total joint arthroplasty?
A: TXA reduces calculated blood loss by 30-50% (approximately 300-500mL) and transfusion risk substantially (the Ker meta-analysis reported transfusion reduced by about one third overall). Hemoglobin drop is reduced by approximately 1 g/dL. Hospital length of stay may be shortened. No clear increase in DVT/PE with appropriate thromboprophylaxis.
Q: What are the absolute and relative contraindications to TXA use in orthopaedic surgery?
A: Absolute: active thromboembolic disease (acute DVT, PE, stroke), subarachnoid haemorrhage, hypersensitivity. Relative: history of VTE (requires thromboprophylaxis), renal impairment (reduce dose by 50% if eGFR 10-30, avoid if under 10), seizure disorder (TXA lowers seizure threshold at high plasma levels), coronary stents. Previous treated VTE with adequate prophylaxis is NOT an absolute contraindication.
Q: What is the evidence for TXA in trauma and noncardiac surgery beyond arthroplasty?
A: CRASH-2 (20,211 trauma patients) reduced mortality when given within 3 hours of injury, and CRASH-3 reduced head-injury death in mild-to-moderate TBI. POISE-3 (9535 noncardiac surgery patients) significantly reduced the composite bleeding outcome (HR 0.76) but did NOT formally establish cardiovascular noninferiority, so standard VTE/cardiovascular care continues. In trauma, give as early as possible and avoid administration more than 3 hours post-injury.
Guidelines, Registries & Global Practice
Global epidemiology and rationale
Perioperative bleeding and allogeneic transfusion are common across orthopaedic surgery worldwide. Untreated, transfusion rates reach 15-25% in primary TKA/THA and are higher in revision, bilateral and trauma cases. TXA is on the WHO Model List of Essential Medicines, reflecting its global relevance and low cost, and is a cornerstone of patient blood management (PBM) programmes internationally.
Major society guidance (side by side)
| Organization / Region | Setting | Recommendation | Key Points |
|---|---|---|---|
| AAOS / AAHKS / Hip & Knee Society / ASRA (US) | Primary TJA | Strong | Routine use; no route/dose/timing clearly superior |
| NICE / BOA (UK) | Elective hip/knee replacement | Recommended | Cost-effective; considered standard of care |
| WHO | Trauma bleeding | Essential Medicine | CRASH-2 protocol, within 3h of injury |
| European trauma guidance (e.g. EuSEM/ESAIC consensus) | Trauma and major surgery | Recommended | Early administration; part of blood management |
Registry and blood-management context
National joint registries (NJR-UK, AJRR-US, AOANJRR-Australia, Swedish/Norwegian registries) do not all capture TXA use directly, but transfusion rates following primary TKA/THA have fallen markedly over the past decade in regions where TXA and PBM programmes have been adopted (e.g. TKA transfusion rates declining from roughly 20% to under 10% nationally in several registries). This temporal correlation supports TXA as a key driver of reduced perioperative transfusion. No registry-level signal of increased VTE or revision has emerged.
Patient blood management (PBM) - three pillars
- Optimise erythropoiesis preoperatively - treat anaemia (iron, erythropoietin if indicated), manage anticoagulation
- Minimise perioperative blood loss - TXA as the key pharmacological intervention, cell salvage, meticulous haemostasis, hypotensive anaesthesia where safe
- Harness tolerance of anaemia - restrictive transfusion thresholds (Hb less than 70-80 g/L unless symptomatic), continued iron supplementation
High- vs limited-resource variation
- High-resource settings: TXA is often embedded in pre-printed order sets and surgical checklists for TJA and trauma, with pharmacy-driven automatic dispensing; cell salvage and restrictive transfusion are routinely available
- Limited-resource settings: TXA is especially valuable because it is cheap, stable and easy to administer, reducing dependence on a constrained donor blood supply; CRASH-2 deliberately recruited across 40 countries to establish global applicability
Barriers and strategies for adoption
Despite strong evidence, uptake varies due to knowledge gaps, outdated VTE-risk concerns and protocol inertia. Effective strategies include institutional protocols, default order sets, education for surgeons/anaesthetists/nurses, and audit-and-feedback on transfusion and TXA utilisation.
TXA is a WHO Essential Medicine and a cornerstone of patient blood management worldwide. Major society guidelines (AAOS, NICE/BOA, WHO, European trauma consensus) converge on routine use in primary TJA and early use in trauma, with no single route or dosing schedule shown to be clearly superior in arthroplasty.
Mechanism
- Synthetic lysine analogue - competitively inhibits plasminogen
- Binds lysine-binding sites, prevents plasmin formation
- Antifibrinolytic - stabilizes clots, does not promote formation
- Half-life 2-3h, 90% renal excretion unchanged
Evidence Base
- TKA/THA: 30-50% reduction in blood loss, substantial transfusion reduction (Level I)
- CRASH-2: 20,211 trauma patients, mortality reduced 16.0% to 14.5% (RR 0.91)
- CRASH-3: benefit in mild-moderate TBI within 3h, no increase in seizures/VTE
- POISE-3: bleeding reduced (HR 0.76) but cardiovascular noninferiority not met
- Ker BMJ meta-analysis: transfusion down ~one third, no clear VTE increase
Dosing Protocols
- TKA/THA: 15-20mg/kg or 1-2g IV bolus pre-incision
- Topical: 2-3g in 50-100mL saline, 5-10 min dwell
- Trauma (CRASH-2): 1g over 10 min, then 1g over 8h within 3h injury
- Spine: Loading 10-15mg/kg, then 1-2mg/kg/h infusion
- Renal impairment: 50% dose if eGFR 10-30, avoid if under 10
Safety Profile
- VTE risk: no clear increase at therapeutic doses (CRASH-2, Ker meta-analysis)
- Mechanism of safety: antifibrinolytic, not procoagulant
- Seizure risk: rare, dose-dependent (over 100mg/kg), risk if renal impairment
- Safe with aspirin, antiplatelet agents, and warfarin
Contraindications
- Absolute: active VTE (acute DVT/PE), subarachnoid hemorrhage, allergy
- Relative: seizure disorder (consider topical), renal impairment (dose adjust)
- Previous treated VTE: relative, ensure adequate prophylaxis
- Trauma timing: DO NOT give if over 3h post-injury (CRASH-2 harm signal)
Routes Comparison
- IV bolus: rapid, systemic, standard for most procedures
- Topical: equivalent to IV in TJA, lower systemic exposure
- IV infusion: for prolonged surgery (spine, complex revision)
- Combined IV+topical: no clear additional benefit over either alone
- Oral: 45% bioavailability, emerging evidence but less studied
Guidelines
- AAOS/AAHKS/ASRA: strong recommendation for TXA in primary TJA
- NICE/BOA: recommended for elective hip/knee replacement
- WHO: Essential Medicine for trauma bleeding (CRASH-2 protocol)
- Standard of care: routine in TJA, trauma, major spine
Cost-Effectiveness
- TXA is inexpensive per gram (a few units per dose)
- A single transfusion costs many times more, plus risks
- NNT roughly 5-10 to prevent one transfusion
- Generally cost-saving (dominant): saves money and improves outcomes
Key Exam Points
- State mechanism clearly: reversible competitive inhibition of plasminogen
- Know CRASH-2: 20,211 patients, reduced mortality, within 3h only
- Safety: no clear VTE increase; acknowledge POISE-3 noninferiority not met
- Dosing: 15-20mg/kg or 1-2g IV for TJA, CRASH-2 protocol for trauma
- Routes equivalent in TJA: IV and topical same efficacy
- Contraindications: absolute vs relative, most patients eligible
- Cost-effective: strong economic argument, should be routine
Common Viva Questions
- Q: Does TXA increase VTE risk? A: No clear increase in surgical meta-analyses
- Q: Mechanism? A: Lysine analogue, reversibly inhibits plasminogen activation
- Q: Dosing in TKA? A: 15-20mg/kg or 1-2g IV pre-incision, or 2-3g topical
- Q: CRASH-2 protocol? A: 1g over 10 min, then 1g over 8h, within 3h injury
- Q: Contraindications? A: Absolute - active VTE, SAH, allergy. Relative - seizure, renal
- Q: IV vs topical? A: Equivalent efficacy in TJA, choose based on patient factors