Radial Distal Row | Body vs Ridge Pattern | CMC Joint Implications
- Two distinct patterns: Body fractures (articular) vs ridge fractures (extra-articular)
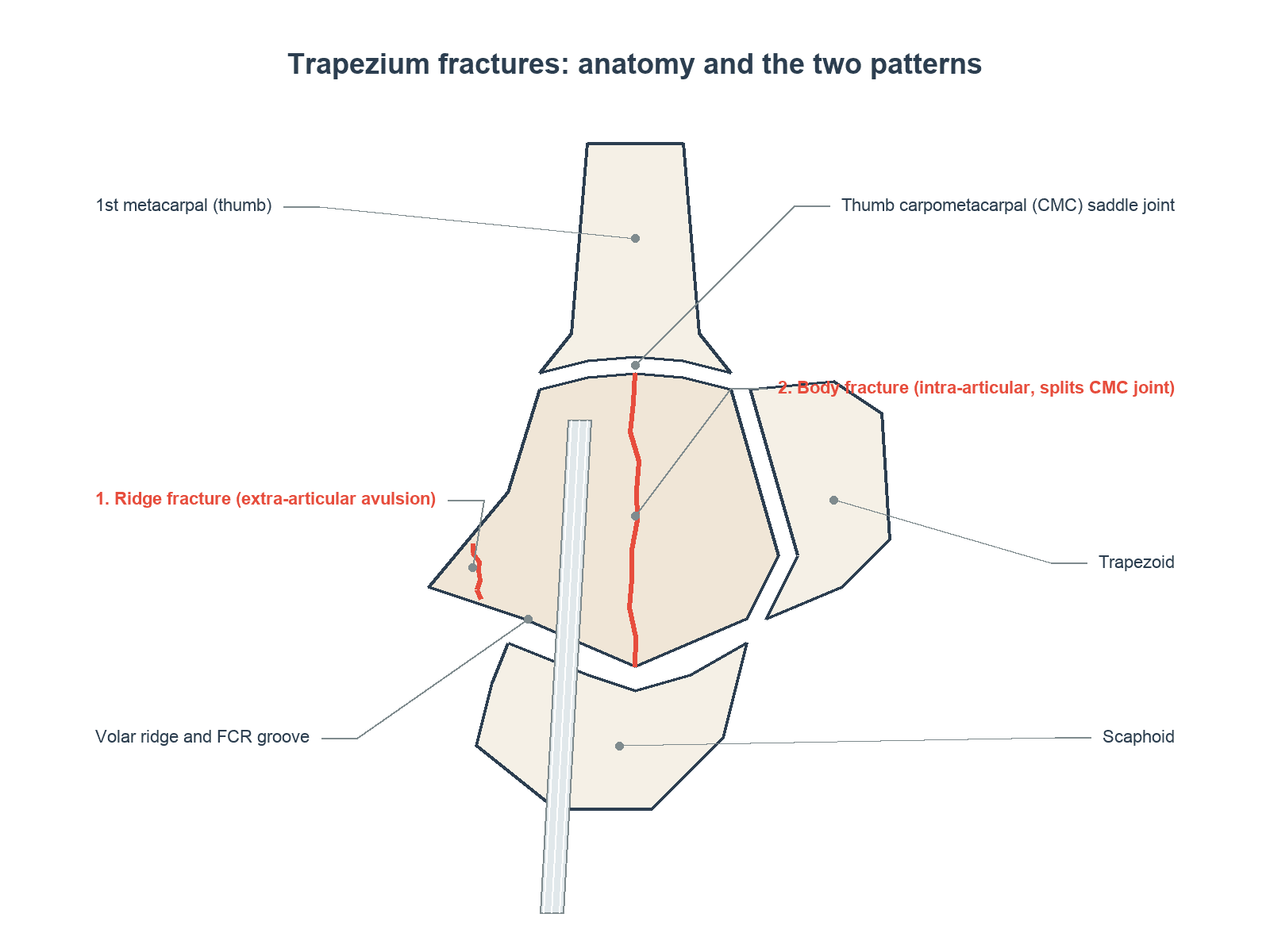
- Body fractures involve thumb CMC joint - articular reduction critical
- Ridge fractures are FCR insertion avulsions - usually conservative
- Bennett's variant: Trapezium body fracture may resemble Bennett's mechanism
- CT essential for body fracture surgical planning
- “Ridge fractures most common - in FCR groove, usually conservative
- “Body fractures involve CMC joint - need anatomic reduction
- “Carpal tunnel view shows ridge fractures best
- “High rate of FCR tendon irritation with ridge fractures
Body fractures are intra-articular, involving the thumb CMC joint - require anatomic reduction. Ridge fractures are extra-articular avulsions in the FCR groove - usually heal with conservative treatment.
The carpal tunnel (Roberts) view is essential for visualizing ridge fractures. Standard PA and lateral views may miss this pattern. Ask for this view specifically if ridge fracture is suspected.
Body fractures affect the thumb CMC joint - the most important joint for hand function. Malreduction leads to early arthritis. Consider these as similar in importance to Bennett's fractures.
The FCR tendon passes through the volar trapezial ridge groove. Ridge fractures can cause FCR tenosynovitis or rupture. Symptomatic non-union may require fragment excision.
- Location
- Volar ridge (FCR groove)
- Management
- Cast 4-6 weeks
- Key Consideration
- Symptomatic non-union: excise
- Location
- Through body
- Management
- Thumb spica cast 6 weeks
- Key Consideration
- Monitor for displacement
- Location
- Through body
- Management
- ORIF with screws/K-wires
- Key Consideration
- CMC articular reduction critical
- Location
- Sagittal through CMC
- Management
- ORIF - restore CMC congruity
- Key Consideration
- Similar to Bennett's
- Location
- Entire trapezium
- Management
- Complex reconstruction or fusion
- Key Consideration
- High energy, poor prognosis
TRAPTRAP - Trapezium Fracture Features
Hook:TRAP - Two patterns, Ridge in FCR groove, Articular body, Pronated view needed
BODYBODY - Body Fracture Priorities
Hook:BODY fractures involve CMC joint - ORIF for Displaced patterns
Overview and Epidemiology
Definition
Trapezium fractures are fractures of the trapezium carpal bone, located on the radial side of the distal carpal row. They include body fractures (involving the thumb CMC articular surface) and ridge fractures (extra-articular avulsions of the volar ridge).
Epidemiology
- Incidence: 3-5% of all carpal fractures
- Ranking: Second most common distal row fracture (after hamate)
- Age distribution: Young to middle-aged adults
- Gender: Male predominance
- Mechanism: Axial load through thumb or direct trauma
Fracture Patterns
Ridge Fractures (More Common)
- Avulsion of volar trapezial ridge
- FCR tendon attachment
- Extra-articular
- Usually conservative treatment
Body Fractures (Less Common but More Significant)
- Through trapezium body
- Involves CMC articular surface
- Requires anatomic reduction
- Higher complication rate
Clinical Significance
The trapezium's position makes it critical for thumb function:
- Articulates with thumb metacarpal (CMC joint)
- Allows opposition, flexion, extension, abduction
- CMC joint is the most mobile and important thumb joint
- Injury affects grip and pinch strength
Understanding the two distinct fracture patterns is essential for appropriate management.
Anatomy/Biomechanics
Osseous Anatomy
Shape and Configuration
- Saddle-shaped: Allows multiplanar thumb motion
- Volar ridge: Prominent projection on palmar surface
- Body: Main bone mass with articular surfaces
Articular Surfaces
- Distal (CMC): Saddle joint with 1st metacarpal
- Medial: Articulates with trapezoid
- Proximal: Articulates with scaphoid
Volar Ridge
- Location: Palmar trapezium surface
- FCR groove: Ridge forms radial border of groove
- Attachments: Transverse carpal ligament, FCR sheath
Blood Supply
Vascular Pattern
- Multiple small vessels
- No single dominant vessel
- Lower AVN risk than scaphoid or lunate
- Good healing potential
Entry Points
- Dorsal and volar surfaces
- Non-articular areas
- Adequate anastomoses
Biomechanics
CMC Joint Function
- Saddle joint: Biaxial motion
- Allows opposition, circumduction
- Critical for grip and pinch
- Most functionally important thumb joint
Load Transmission
- Forces from thumb concentrate here
- High stress during pinch and grip
- Predisposed to arthritic changes
FCR Relationship
- FCR passes through volar groove
- Ridge fractures affect FCR glide
- Chronic irritation causes tenosynovitis
The FCR tendon passes through a groove bounded by the volar ridge. Ridge fractures can cause FCR irritation, tenosynovitis, or even rupture. Always assess FCR function and consider this in management.
Understanding anatomy guides surgical approach and management priorities.
Classification Systems
Anatomical Classification
Based on fracture location:
Type I - Vertical Body Fracture
- Sagittal split through body
- Involves CMC articular surface
- Similar mechanism to Bennett's fracture
- Treatment: ORIF if displaced
Type II - Horizontal Body Fracture
- Coronal split through body
- May involve scaphotrapeziotrapezial joint
- Less common than vertical
- Treatment: ORIF if displaced
Type III - Dorsal Ridge Fracture
- Small dorsal avulsion
- Ligament attachment site
- Usually small fragment
- Treatment: Conservative
Type IV - Volar Ridge Fracture
- Most common pattern overall
- FCR groove avulsion
- Extra-articular
- Treatment: Conservative, excision if symptomatic
Type V - Comminuted Body
- Multiple fragments
- High-energy mechanism
- Articular involvement
- Treatment: Complex reconstruction or fusion
Location and articular involvement guide treatment.
- Location
- Volar/dorsal ridge
- Articular
- No
- Treatment
- Conservative, excision if needed
- Location
- Sagittal through CMC
- Articular
- Yes
- Treatment
- ORIF
- Location
- Coronal
- Articular
- Variable
- Treatment
- ORIF if displaced
- Location
- Entire body
- Articular
- Yes
- Treatment
- Complex reconstruction/fusion
Trapezial ridge fractures have their own named scheme (Palmer, 1981) that predicts healing and explains the heal-versus-excise behaviour. Type I is a fracture at the base of the ridge (where it joins the trapezial body) — better vascularised, it generally unites with cast immobilisation. Type II is an avulsion of the tip of the ridge — distal, poorly vascularised and pulled by the transverse carpal ligament, so it is prone to non-union and, if symptomatic, is best treated by fragment excision rather than prolonged immobilisation. Both can irritate the adjacent FCR, but the Type II tip avulsion is the classic cause of the symptomatic non-union that comes to excision.
Classification determines treatment approach and expected outcomes.
Clinical Assessment
History
Mechanism of Injury
- FOOSH: Fall with thumb abducted
- Direct trauma: Blow to thenar eminence
- Axial load: Punch or fall onto thumb
- Avulsion: Forceful wrist flexion (ridge fractures)
Key History Points
- Exact mechanism and thumb position
- Energy of injury
- Immediate symptoms
- Hand dominance and occupation
- Prior thumb/wrist pathology
Physical Examination
Inspection
- Swelling over thenar eminence
- Bruising at thumb base
- Compare to contralateral hand
Palpation
- Anatomic snuffbox: May be tender (overlaps with scaphoid)
- Thenar eminence: Direct trapezium tenderness
- Volar wrist crease: Ridge tenderness
- FCR tendon: Assess for tenosynovitis
Range of Motion
- Thumb CMC motion limited by pain
- Opposition particularly affected
- Compare to contralateral
Stability Assessment
- CMC joint stability
- Stress testing after adequate analgesia
- Compare to opposite side
Neurovascular Assessment
- Usually preserved
- Median nerve (thenar branch) may be at risk
- Document baseline
Special Tests
Grind Test
- Axial load with rotation at CMC
- Pain suggests CMC pathology
- May be positive with both fracture and arthritis
FCR Provocation
- Resisted wrist flexion
- Pain suggests FCR involvement
- Important for ridge fractures
Thumb Pinch Strength
- Markedly reduced with trapezium injury
- Compare to contralateral
- Baseline for recovery assessment
Clinical examination helps differentiate ridge from body fractures.
Differential Diagnosis
Radial-sided wrist and thumb-base pain after trauma has several mimics. The trapezium sits at the crossroads of the scaphoid, the thumb metacarpal base, the scaphotrapeziotrapezoid (STT) joint, and the FCR tunnel, so each must be actively excluded.
- Distinguishing features
- Snuffbox and scaphoid tubercle tenderness, FOOSH mechanism
- Key test / discriminator
- Scaphoid-series radiographs; MRI/CT if occult
- Distinguishing features
- Pain and deformity at the metacarpal base, not the trapezium
- Key test / discriminator
- PA/lateral thumb views show metacarpal base fracture-subluxation
- Distinguishing features
- Gross instability of thumb base; may coexist with body fracture
- Key test / discriminator
- Stress views; reduce and reassess stability (see Roger et al.)
- Distinguishing features
- Older patient, chronic pain, positive grind test, no acute trauma
- Key test / discriminator
- Radiographs show joint-space loss/osteophytes, not a fracture line
- Distinguishing features
- Volar pain with resisted wrist flexion, no fracture
- Key test / discriminator
- Tenderness along FCR; ultrasound; may follow ridge malunion
- Distinguishing features
- Pain just distal to scaphoid, insidious onset
- Key test / discriminator
- Radiographs show STT joint degeneration
- Distinguishing features
- Volar ridge tenderness (extra-articular) vs dorsal CMC tenderness (intra-articular)
- Key test / discriminator
- Carpal tunnel (Roberts) view for ridge; CT for body
Investigations
Plain Radiographs
Standard Views
- PA view: May show body fractures
- Lateral view: Assess displacement
- Oblique view: Additional perspective
Carpal Tunnel (Roberts) View
- Essential for ridge fractures
- Wrist hyperextended, beam angled 25 degrees
- Shows volar ridge clearly
- Ridge fractures easily missed without this view
Betts View (Hyperpronation)
- Isolates trapezium from overlapping bones
- Good for body fracture assessment
- Complement to carpal tunnel view
Signs to Look For
- Ridge fragment on carpal tunnel view
- Body fracture line on PA/oblique
- CMC joint congruity
- Associated thumb metacarpal injury
CT Scanning
Indications
- Body fracture surgical planning
- Assessment of CMC articular surface
- Comminution evaluation
- Occult fracture detection
Key CT Findings
- Fracture orientation (vertical vs horizontal)
- Articular step-off or gap
- Fragment size and displacement
- Associated injuries
MRI
Indications
- Soft tissue assessment
- FCR tendon evaluation
- Occult fracture detection
- Ligament injury assessment
Findings
- Bone marrow edema
- FCR tenosynovitis
- Ligament integrity
Investigations summary is provided below.
- Primary Role
- Body fractures
- Advantage
- Available, quick
- Limitation
- May miss ridge fractures
- Primary Role
- Ridge fractures
- Advantage
- Essential for ridge
- Limitation
- Specific technique needed
- Primary Role
- Surgical planning
- Advantage
- Articular detail
- Limitation
- Essential for ORIF
- Primary Role
- Soft tissue, FCR
- Advantage
- FCR tendon status
- Limitation
- Rarely needed acutely
The carpal tunnel view is essential and must be specifically requested for ridge fracture evaluation.
Management Algorithm

Ridge Fracture Management
Initial Treatment
Ridge fractures are extra-articular and generally have excellent prognosis with conservative treatment.
Immobilization
- Thumb spica splint or cast
- Thumb in functional position
- Duration: 4-6 weeks
- May use removable splint if compliant
Follow-Up
- Week 2: Clinical review
- Week 4-6: Assess tenderness, mobility
- If non-tender, begin mobilization
Symptomatic Non-Union
Occurs in minority of cases:
Presentation
- Persistent thenar pain
- FCR tenosynovitis symptoms
- Pain with wrist flexion/extension
- Tender over volar ridge
Management
- Trial of splinting and anti-inflammatories
- Steroid injection may provide temporary relief
- Fragment excision if persistent symptoms
Excision Technique
- Volar approach through FCR sheath
- Excise fragment, smooth bed
- Protect FCR tendon
- Good outcomes expected
Ridge fractures have excellent prognosis with appropriate management.
Treatment depends on fracture type - ridge vs body.
RIDGERIDGE - Ridge Fracture Management
Hook:RIDGE fractures: Roberts view, Immobilize, may need Delayed excision, Good prognosis
Surgical Technique
ORIF for Trapezium Body Fracture
Preoperative Planning
- CT scan for fracture characterization
- Plan approach based on fracture pattern
- Identify fragment size for fixation choice
Patient Setup
- Supine, arm table
- Tourniquet applied
- Fluoroscopy available
Dorsal Approach
Skin Incision
- Longitudinal over dorsal CMC joint
- Start at 1st metacarpal base
- Extend proximally 3-4 cm
Deep Dissection
- Identify radial sensory nerve branches (protect)
- Retract EPB and EPL appropriately
- Incise CMC capsule longitudinally
- Expose trapezium and articular surface
Fracture Reduction
Visualization
- Direct view of articular surface
- Assess fracture pattern
- Identify all fragments
Reduction Technique
- Use dental pick or small elevator
- Manipulate fragments to anatomic position
- Assess reduction visually and with fluoroscopy
- Provisional K-wire fixation
Definitive Fixation
Screw Technique
- 2.0-2.4mm headless compression screw
- Drill, measure, tap if needed
- Insert screw perpendicular to fracture line
- Countersink below cartilage
- Check with fluoroscopy
K-Wire Technique
- Multiple 1.1-1.25mm K-wires
- Cross fracture in different planes
- May span CMC joint if needed
- Plan for removal at 6 weeks
Closure
- Repair CMC capsule
- Close subcutaneous layer
- Skin closure
- Thumb spica splint
Anatomic reduction of the CMC surface is essential for good outcomes.
Surgical technique varies based on fracture pattern.
Complications
Ridge Fracture Complications
FCR Tenosynovitis
- Common with symptomatic non-union
- Fragment irritates tendon
- Treatment: Excision with debridement
FCR Rupture (Rare)
- Chronic irritation from fragment
- Usually in untreated symptomatic cases
- Treatment: Fragment excision, tendon repair if possible
Symptomatic Non-Union
- Occurs in 10-20% of ridge fractures
- May be asymptomatic
- Treatment: Excision if symptomatic
Body Fracture Complications
Malunion
- CMC articular incongruity
- Leads to early arthritis
- Prevention: Anatomic reduction
- Treatment: May need osteotomy or fusion
Post-Traumatic CMC Arthritis
- Most significant long-term complication
- Related to residual step-off
- Progressive thumb base pain
- Treatment: CMC arthroplasty or fusion
Nonunion
- Uncommon with proper treatment
- May require bone grafting
- Consider internal fixation
Stiffness
- CMC joint may become stiff
- Prevention: Early mobilization when stable
- Treatment: Hand therapy, patience
Surgical Complications
Radial Sensory Nerve Injury
- Dorsal approach at risk
- Prevention: Careful identification
- Treatment: Usually recovers, may need neurolysis
Screw/Hardware Problems
- Joint penetration
- Prominent hardware
- Treatment: Removal when healed
Infection
- Rare
- Standard treatment principles
- Fracture Type
- Ridge
- Prevention
- Early treatment
- Management
- Fragment excision
- Fracture Type
- Body
- Prevention
- Anatomic reduction
- Management
- Arthroplasty or fusion
- Fracture Type
- Either
- Prevention
- Adequate immobilization/fixation
- Management
- Bone graft, fixation
- Fracture Type
- Body
- Prevention
- Early mobilization
- Management
- Hand therapy
Post-traumatic trapeziometacarpal (CMC) arthritis is the feared long-term consequence of a malreduced body fracture, and the salvage options mirror those for primary thumb-base osteoarthritis, with the choice driven by age and demand. Trapeziectomy, with or without ligament reconstruction and tendon interposition (LRTI) — typically using an FCR or APL slip — is the workhorse for older, lower-demand patients: it reliably relieves pain and preserves mobility at the cost of some pinch strength and metacarpal subsidence. CMC arthrodesis (fusion) is preferred for the young, high-demand manual worker because it preserves pinch and grip strength and durability, accepting loss of thumb-base mobility plus a risk of nonunion and adjacent scaphotrapeziotrapezoid (STT) arthritis. Implant/prosthetic arthroplasty is used selectively. Localised trapeziometacarpal arthritis can be addressed in isolation, whereas pan-trapezial (including STT) degeneration favours trapeziectomy over fusion.
CMC arthritis is the main concern with body fractures; FCR problems with ridge fractures.
Postoperative Care
Conservative Treatment Protocol
Ridge Fractures
Week 0-4
- Thumb spica splint or cast
- Finger motion encouraged
- Ice and elevation for swelling
Week 4-6
- Assess tenderness
- If non-tender, begin mobilization
- Wean from splint
Week 6+
- Progressive ROM and strengthening
- Return to activities as tolerated
- Monitor for late FCR symptoms
Undisplaced Body Fractures
Week 0-6
- Thumb spica cast
- Serial radiographs at week 2 and 4
- Finger exercises throughout
Week 6-8
- If healed, transition to splint
- Begin gentle thumb ROM
- Progressive activity
Surgical Treatment Protocol
ORIF for Body Fractures
Immediate (0-2 Weeks)
- Thumb spica splint
- Elevate and ice
- Finger motion
Week 2-6
- Thumb spica cast
- Monitor wound
- Continue finger ROM
Week 6
- Radiographs to assess healing
- K-wire removal if used
- Transition to removable splint
- Begin gentle thumb ROM
Week 6-12
- Progressive ROM
- Light strengthening
- Hand therapy guidance
Week 12+
- Full activities as tolerated
- Progressive grip strengthening
- Sport at 3-4 months
Ridge Excision
Week 0-2
- Light splint for comfort
- Suture removal at 10-14 days
- Begin ROM
Week 2-6
- Progressive activities
- Usually fully recovered
- Return to work/sport
Follow-Up Schedule
- Week 2
- Clinical
- Week 6
- If symptomatic
- Week 12
- As needed
- Month 6
- -
- Week 2
- X-ray
- Week 6
- X-ray, ROM
- Week 12
- Function
- Month 6
- As needed
- Week 2
- Wound
- Week 6
- X-ray, K-wire removal
- Week 12
- Function
- Month 6
- Final
- Week 2
- Sutures
- Week 6
- Final
- Week 12
- -
- Month 6
- -
Rehabilitation is tailored to fracture type and treatment method.
Outcomes and Prognosis
Ridge Fractures
Conservative Treatment Outcomes
- Union rate: Over 90% heal with casting
- Function: Excellent in most cases
- Symptomatic non-union: 10-20%
After Fragment Excision
- Pain relief: Over 95% satisfied
- Function: Return to previous activities
- FCR problems: Resolved with excision
Body Fractures
Conservative Treatment (Undisplaced)
- Good outcomes when truly undisplaced
- Risk of secondary displacement
- Close monitoring essential
Surgical Treatment (ORIF)
- Articular reduction determines outcome
- Step-off under 1mm: Good outcomes
- Step-off over 2mm: Higher arthritis rate
- ROM recovery: 80-90% of contralateral
Long-Term CMC Joint Health
- Anatomic reduction: Lower arthritis rate
- Malreduction: Progressive CMC OA
- May require later CMC arthroplasty
Prognostic Factors
Favorable
- Ridge fracture pattern
- Undisplaced body fracture
- Early treatment
- Anatomic reduction achieved
- Compliant patient
Unfavorable
- Displaced body fracture
- Comminuted pattern
- Delayed treatment
- Articular incongruity
- Associated injuries
Return to Activity
Ridge Fractures
- Desk work: 2-4 weeks
- Light manual: 4-6 weeks
- Heavy manual: 6-8 weeks
- Sports: 6-8 weeks
Body Fractures
- Desk work: 4-6 weeks
- Light manual: 8-12 weeks
- Heavy manual: 12-16 weeks
- Contact sports: 4-6 months
Prognosis depends on fracture type and treatment adequacy.
Guidelines, Registries & Global Practice
Global Epidemiology
Trapezium fractures are uncommon, comprising roughly 3-5% of carpal fractures, and non-scaphoid carpal fractures as a whole are rare. In the population-based Australian Geelong/Barwon cohort, the incidence of non-scaphoid carpal fractures was 15.9 per 100,000 person-years in males and 4.5 per 100,000 person-years in females, with a male predominance, a peak in young adulthood (20-29 years), and most fractures resulting from a fall (Holloway et al., Arch Osteoporos 2015, PMID 25910867). Contemporary hand-surgery reviews emphasise that these injuries are frequently associated with other carpal or metacarpal injuries and are easily missed on standard radiographs (Suh, Ek, Wolfe, J Hand Surg Am 2014, PMID 24679911).
- Figure
- approximately 3-5%
- Source
- Carpal fracture reviews
- Figure
- 15.9 / 100,000 / year
- Source
- Holloway 2015 (Australia)
- Figure
- 4.5 / 100,000 / year
- Source
- Holloway 2015 (Australia)
- Figure
- Fall (greater than 87% of carpal fractures)
- Source
- Holloway 2015 (Australia)
- Figure
- Male predominance, peak 20-29 years
- Source
- Holloway 2015 (Australia)
Guideline & Society Positions
No fracture-specific society guideline (AAOS, NICE, BOA/BSSH, AO, EFORT) is dedicated to the trapezium given its rarity; practice is driven by general carpal-fracture principles and hand-surgery consensus. The table below summarises the converging guidance and its evidence basis.
- Position relevant to trapezium fractures
- Undisplaced fractures: cast immobilisation; displaced intra-articular body fractures: anatomic ORIF (screws/K-wires) to restore CMC congruity
- Evidence level
- Expert consensus
- Position relevant to trapezium fractures
- Image beyond standard views when clinically suspected; treat extra-articular ridge fractures conservatively, refer displaced articular fractures
- Evidence level
- Expert consensus / low
- Position relevant to trapezium fractures
- No trapezium-specific recommendation; supports specialist referral for intra-articular hand/wrist fractures and shared decision-making
- Evidence level
- Guideline (indirect)
- Position relevant to trapezium fractures
- No dedicated guideline; texts endorse conservative care for ridge fractures and ORIF for displaced body fractures with CMC involvement
- Evidence level
- Expert consensus
- Position relevant to trapezium fractures
- Aligns with AO principles; emphasises CT for articular planning and FCR assessment for ridge fractures
- Evidence level
- Expert consensus
Registry Evidence
No national fracture registry tracks trapezium fractures specifically. Indirect registry-adjacent signals come from arthroplasty literature: trapezium fracture is a recognised complication of certain CMC implants (for example, implant subsidence into the trapezium), reinforcing that the bone is mechanically loaded and that articular integrity matters. The Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) does not separately report trapezium fracture but documents thumb-base arthroplasty activity, the downstream burden that post-traumatic CMC arthritis can contribute to.
Practice Variation
- Imaging access: dedicated carpal tunnel (Roberts) views and early CT are routine in well-resourced systems but variably available elsewhere, driving differences in detection of ridge and occult body fractures.
- Fixation choice: headless compression screws are preferred where fragment size permits; K-wires remain widely used for small fragments or in lower-resource settings.
- Rehabilitation: structured hand-therapy pathways (well established in high-income settings such as Australia, the UK, and North America) shorten time to return of function; access varies internationally.
- Imaging request practices: dedicated carpal tunnel (Roberts) views must be specifically requested; targeted education of emergency and primary-care clinicians reduces missed ridge fractures.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old man presents after falling during boxing with pain over the thenar eminence. Standard PA and lateral radiographs are reported as normal. What do you do next?”
“CT confirms a vertical body fracture of the trapezium with 3mm of articular step-off at the CMC joint. How do you manage this injury?”
“A patient presents 4 months after a trapezium ridge fracture. Despite casting, they have persistent volar wrist pain that worsens with gripping. X-rays confirm non-union. How do you manage this?”
MCQ Practice Points
Q: What is the most common trapezium fracture pattern? A: Volar ridge fractures are the most common pattern, occurring in the FCR groove. Body fractures involving the CMC joint are less common but more clinically significant.
Q: Which radiographic view is essential for diagnosing trapezium ridge fractures? A: The carpal tunnel (Roberts) view is essential. Obtained with wrist hyperextended and beam angled 25 degrees, it demonstrates the volar ridge that is obscured on standard PA and lateral views.
Q: Why is the FCR tendon at risk with trapezium ridge fractures? A: The FCR tendon passes through a groove bounded by the volar ridge. Ridge fractures can cause FCR tenosynovitis or rupture, and this relationship must be considered in management.
Q: What articular step-off threshold indicates ORIF for trapezium body fractures? A: Articular step-off greater than 2mm is the threshold for surgical intervention. Malreduction predicts post-traumatic CMC arthritis.
Q: What percentage of trapezium ridge fractures develop symptomatic non-union? A: Approximately 10-20% develop symptomatic non-union. These are effectively treated with fragment excision.
Q: What is the definitive treatment for symptomatic trapezium ridge non-union? A: Fragment excision through a volar approach. This is a straightforward procedure with excellent outcomes in over 95% of cases.
Understanding these key concepts will help with exam success.
Key Concepts
- 3-5% of all carpal fractures
- Two patterns: Ridge (common) vs Body (CMC involved)
- Ridge = extra-articular, FCR groove
- Body = intra-articular, CMC joint
- Carpal tunnel view essential for ridge
Ridge Fracture Management
- Conservative: Thumb spica 4-6 weeks
- Most heal with immobilization
- 10-20% symptomatic non-union
- Fragment excision if symptomatic
- Excellent prognosis
Body Fracture Management
- Undisplaced: Cast 6-8 weeks
- Displaced (over 2mm step-off): ORIF
- Anatomic CMC reduction essential
- Headless screws or K-wires
- Malreduction = CMC arthritis
Imaging Strategy
- Standard PA/Lat: May miss ridge fractures
- Carpal tunnel (Roberts) view: Essential for ridge
- Betts view: Isolates trapezium
- CT: Body fracture surgical planning
Surgical Pearls
- Dorsal approach for body ORIF
- Volar approach for ridge excision
- Protect radial sensory nerve (dorsal)
- Assess FCR at surgery (volar)
Complications
- Ridge: FCR tenosynovitis, non-union
- Body: CMC arthritis from malreduction
- Body arthritis may need arthroplasty/fusion
- Ridge excision: over 95% success
Evidence Base
- Non-scaphoid carpal fractures are rare and frequently associated with concomitant carpal or metacarpal injury
- Trapezium fractures divide into intra-articular body and extra-articular ridge patterns
- Standard radiographs frequently miss these fractures; dedicated views and CT improve detection
- Anatomic restoration of the carpometacarpal articular surface is the priority for body fractures
- Early descriptive series establishing the trapezium (greater multangular) body fracture pattern
- Body fractures involve the carpometacarpal articular surface
- Displaced articular fractures benefit from reduction to restore joint congruity
- Malreduction predisposes to symptomatic carpometacarpal degeneration
- Malunited volar trapezial ridge fracture produced chronic flexor carpi radialis (FCR) tendinitis
- Symptoms localised to the volar wrist over the FCR with activity-related pain
- Excision of the malunited ridge fragment relieved symptoms
- Confirms the mechanistic link between the volar ridge and FCR irritation
- FCR insertion onto the trapezium present in all 42 cadaveric wrists
- Mean fibrous insertion length 11.8 mm (SD 4.14 mm)
- Confirms an intimate FCR–trapezial ridge relationship
- Explains FCR vulnerability in ridge fractures and in volar approaches/CMC arthroplasty
- Combined trapeziometacarpal dislocation with trapezium fracture is rare (about 15 reported cases)
- Closed reduction may leave residual dorsal instability
- Open anatomic reduction with internal screw fixation restored joint stability
- Small fragments may require supplementary ligament reconstruction (e.g. FCR strip)
- Population-based carpal fracture incidence in the Barwon region, Victoria, Australia
- Non-scaphoid carpal fracture incidence 15.9/100,000/year (males) and 4.5/100,000/year (females)
- Male predominance with a peak at 20–29 years; most fractures resulted from a fall
- Confirms that non-scaphoid carpal fractures (including trapezium) are uncommon
The evidence supports distinct management approaches for ridge and body fractures, anchored by a contemporary reference review, the classic body-fracture series, anatomic and clinical data linking the volar ridge to the FCR, and population-based epidemiology from the Geelong/Barwon cohort.