Rare Carpal Fracture | Second Metacarpal Articulation
- Rarest Carpal Fracture: Less than 1% of all carpal fractures.
- Location: Distal carpal row. Articulates with Trapezium, Capitate, Scaphoid, and 2nd MC.
- Protection: The trapezoid is well-protected (recessed in the distal row, keystone of 2nd CMC).
- Mechanism: Axial load through 2nd metacarpal (punch, fall on flexed wrist).
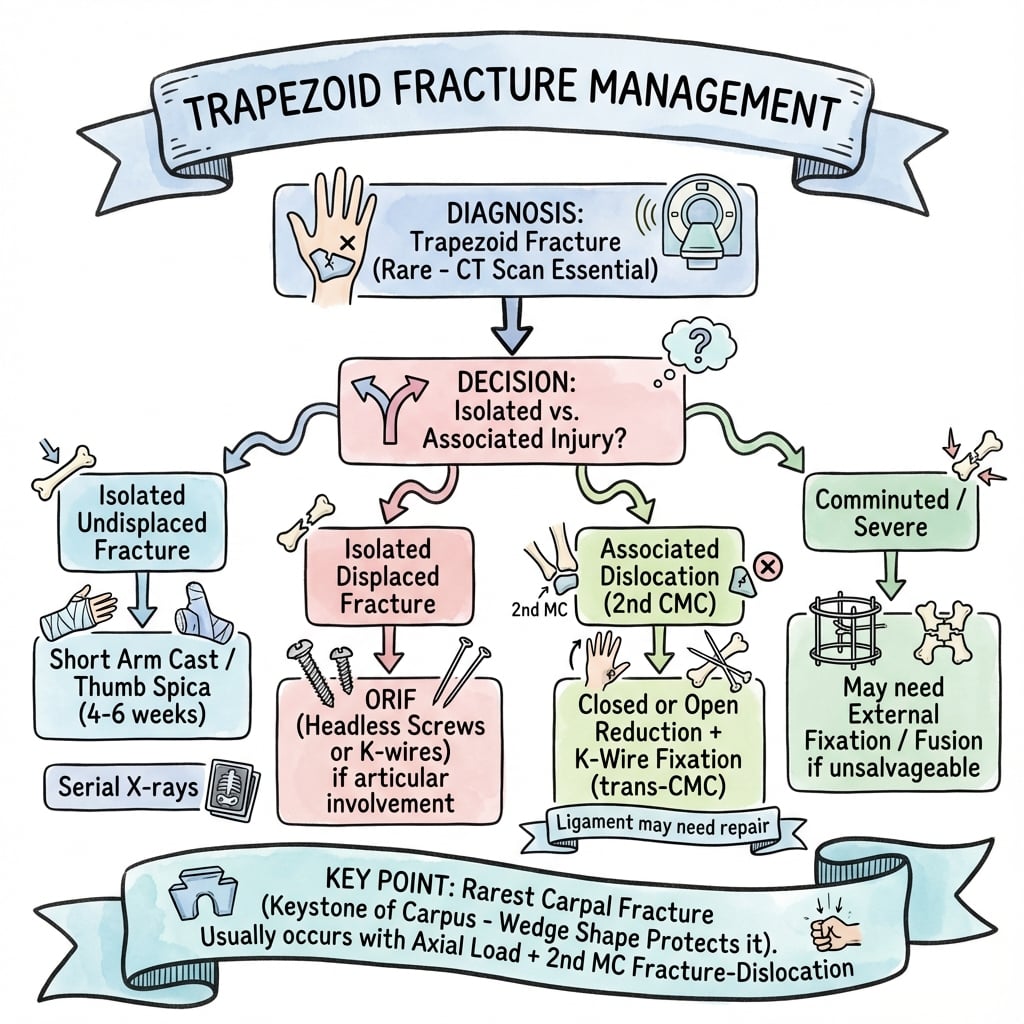
- Treatment: Non-displaced = Cast. Displaced/Dislocated = ORIF.
- “Trapezoid is the RAREST carpal bone to fracture.
- “Look for associated injuries (2nd CMC dislocation, scaphoid fracture).
- “CT is essential for diagnosis and surgical planning.
- “Most non-displaced fractures can be managed with immobilization.
CT is Key. Trapezoid fractures are easily missed on X-ray due to overlapping carpal bones. Get CT if suspicious.
2nd CMC Dislocation. Often associated with 2nd CMC fracture-dislocation. Assess entire carpus.
Keep in Differential. Because it's rare, it may be overlooked. Maintain high suspicion with dorsal wrist pain after axial load.
Post-Traumatic OA. Important for wrist biomechanics. Articular fractures may lead to 2nd CMC arthrosis.
- Frequency
- ~70%
- Key Associated Injury
- Distal Radius, Perilunate
- Frequency
- ~15%
- Key Associated Injury
- Perilunate, Lunate
- Frequency
- ~3%
- Key Associated Injury
- Kienböck's (if AVN)
- Frequency
- ~3%
- Key Associated Injury
- Thumb CMC, Bennett's
- Frequency
- ~2%
- Key Associated Injury
- Scaphocapitate Syndrome
- Frequency
- ~2%
- Key Associated Injury
- Hook fracture, Boxer's
- Frequency
- less than 1%
- Key Associated Injury
- 2nd CMC Dislocation
- Frequency
- ~1%
- Key Associated Injury
- FCU tendon injury
She Looks Too Pretty; Try To Catch HerCarpal Bones
Hook:Carpal bone order: Proximal then Distal.
TRAP-2Trapezoid Articulations
Hook:Trapezoid is the keystone of 2nd CMC.
PUNCHMechanism
Hook:Punch injury mechanism.
Overview and Epidemiology
Trapezoid fractures are fractures of the trapezoid bone, the second bone of the distal carpal row. It is the rarest carpal bone to fracture, accounting for less than 1% of all carpal fractures.
- Incidence: Extremely rare.
- Mechanism: Axial load through 2nd metacarpal (punch, fall on flexed wrist).
- Associated Injuries: 2nd CMC dislocation, Perilunate injury, Scaphoid fracture.
- Trapezoid is recessed within the distal carpal row.
- Protected by surrounding bones.
- Strong ligamentous attachments.
- Keystone of the rigid 2nd CMC joint.
Anatomy and Pathophysiology
- Location: Distal carpal row. Between trapezium (radial) and capitate (ulnar).
- Shape: Wedge-shaped - broad (wide) dorsally, narrow (apex) palmarly/volarly.
- Articulations:
- Proximal: Scaphoid.
- Distal: 2nd Metacarpal base (key articulation).
- Radial: Trapezium.
- Ulnar: Capitate.
- 2nd CMC Joint: Most stable CMC joint (index finger ray). Keystone is the trapezoid.
- Force Transmission: Axial load through 2nd MC can fracture trapezoid.
- Enters from dorsal and palmar surfaces.
- AVN is rare.
Classification
Simple Classification
- Non-Displaced: Fracture without significant articular step-off.
- Displaced: Significant displacement or articular incongruity.
- With Dislocation: Associated 2nd CMC or intercarpal dislocation.
- Comminuted: Multiple fragments (often with high-energy).
CT is necessary to classify accurately.
Clinical Assessment
- Mechanism: Punch? Fall on flexed wrist? Axial load?
- Pain Location: Dorsal wrist, over 2nd MC base.
- Tenderness: Over trapezoid (dorsal, between 1st and 2nd MC bases).
- Swelling: Dorsal wrist.
- Pain: With axial loading of 2nd metacarpal.
- ROM: Painful wrist flexion/extension.
- Neurovascular: Usually intact.
Investigations
- X-ray (PA, Lateral, Oblique): May show fracture, but often missed due to overlap.
- CT Scan: Essential for diagnosis. Defines fracture pattern, displacement.
- MRI: Rarely needed. For occult fractures or soft tissue assessment.
- X-ray: Subtle cortical irregularity. Overlap with scaphoid/capitate.
- CT: Clearly delineates fracture. Assess articular involvement.
Differential Diagnosis
The trapezoid fracture presents as dorsal wrist pain at the index-ray base after axial load — overlapping with several commoner injuries. CT is the discriminator.
- Distinguishing Feature
- Tenderness at 2nd MC base; pain on axial load of index ray; often missed on plain film
- Best Test
- CT
- Distinguishing Feature
- Dorsal prominence of index MC base; cascade-line disruption; commonly coexists
- Best Test
- Lateral/oblique radiograph + CT
- Distinguishing Feature
- Anatomical snuffbox and scaphoid tubercle tenderness; radial-sided
- Best Test
- Scaphoid views; CT/MRI if occult
- Distinguishing Feature
- Thumb-base tenderness; pain on thumb axial load (Bennett-type force)
- Best Test
- CT; carpal tunnel/Bett view
- Distinguishing Feature
- Diffuse tenderness, no bony point tenderness; normal CT
- Best Test
- Clinical + negative CT
Management Algorithm
Non-Displaced Fractures
Conservative Management.
- Immobilization: Short arm cast or thumb spica for 4-6 weeks.
- Follow-up: Repeat X-ray/CT at 4-6 weeks for healing.
- Rehabilitation: ROM exercises after cast removal.
Most non-displaced fractures heal well.
Surgical Technique
Dorsal Approach
Incision: Dorsal longitudinal incision centered over 2nd MC base
Structures at Risk:
- Radial artery (anatomical snuffbox)
- Extensor tendons (EPL, ECRL, ECRB)
- Superficial branch radial nerve
Exposure: Capsulotomy between 2nd and 3rd extensor compartments
Complications
- Risk Factor
- Articular fracture
- Management
- Fusion (CMC) / Excision
- Risk Factor
- Inadequate reduction
- Management
- Osteotomy / Accept
- Risk Factor
- Prolonged immobilization
- Management
- Physiotherapy
- Risk Factor
- Rare (good blood supply)
- Management
- Bone graft / Fixation
Postoperative Care
- ROM exercises at 4-6 weeks.
- Strengthen at 6-8 weeks.
- Splint 2 weeks, then cast/removable splint.
- ROM at 4-6 weeks.
- K-wire removal at 6-8 weeks if used.
Outcomes
- Non-Displaced: Good prognosis with immobilization.
- Displaced/Dislocated: Risk of 2nd CMC arthrosis if not anatomically reduced.
The Wedge Shape and Why It Dislocates Dorsally
The topic notes a dorsal 2nd CMC dislocation and a rare palmar trapezoid dislocation but never explains why the trapezoid dislocates the way it does.
- The wedge and the ligaments. The trapezoid is wedge-shaped - broad dorsally, narrow (apex) palmarly - and its palmar (volar) intercarpal ligaments are stronger than the dorsal ones.
- So it dislocates dorsally. An axial force on the index metacarpal, resisted by the strong palmar ligaments, levers the wedge dorsally out of its mortise and tears the weaker dorsal capsule - so dorsal dislocation is the usual pattern (as reported in the trapezoid-dislocation literature).
- Palmar dislocation is rarer. A volar (palmar) dislocation requires higher energy (the strong palmar ligaments must fail) and is typically seen in polytrauma - much less common than the dorsal pattern.
Q: Why does the trapezoid usually dislocate dorsally?
A: It is wedge-shaped (broad dorsally, narrow/apex palmarly) with stronger palmar (volar) than dorsal ligaments; an axial force on the index metacarpal, resisted by the strong palmar ligaments, levers the wedge dorsally out of its mortise (tearing the weaker dorsal capsule) - so dorsal dislocation predominates. Volar/palmar dislocation is rarer, needs higher energy (strong palmar ligaments must fail), and is typically seen in polytrauma.
The Keystone of the Hand's Fixed Pillar
The topic calls the 2nd CMC 'the most stable CMC joint' with the trapezoid its keystone, and 'important for wrist biomechanics', but never explains the fixed-central-pillar concept.
- The fixed central pillar. The 2nd and 3rd (index and middle) carpometacarpal joints are essentially immobile, forming the fixed central pillar of the hand - the rigid unit around which the mobile thumb (1st CMC, a saddle joint) and the ulnar rays (4th about 10-15 degrees, 5th about 20-30 degrees of flexion-extension) move for grip and cupping.
- The trapezoid is the keystone. Recessed and mortised between the trapezium, capitate, scaphoid and 2nd metacarpal, the trapezoid locks the index ray into the carpus, giving it the rigid, stable base needed for precision and power grip.
- Why the injury matters. A trapezoid fracture or a 2nd-CMC fracture-dislocation destabilises this fixed pillar - threatening grip strength and risking 2nd-CMC arthrosis - which is why displaced injuries are anatomically reduced and the CMC stabilised.
Q: Why is the trapezoid the 'keystone' of the hand's fixed pillar?
A: The 2nd and 3rd (index/middle) CMC joints are essentially immobile - the fixed central pillar of the hand - around which the mobile thumb (1st CMC saddle joint) and ulnar rays (4th about 10-15 degrees, 5th about 20-30 degrees) move. The trapezoid, mortised between trapezium/capitate/scaphoid/2nd-MC, locks the index ray into the carpus (the rigid base for grip). A trapezoid fracture or 2nd-CMC fracture-dislocation destabilises this pillar, threatening grip and risking 2nd-CMC arthrosis - hence anatomic reduction.
Guidelines, Registries & Global Practice
There are no condition-specific society guidelines or arthroplasty-registry data for trapezoid fractures given their rarity; practice is governed by general carpal-injury and hand-trauma principles.
Global epidemiology
- Carpal bones contribute roughly 18% of hand fractures, of which the scaphoid dominates (~60% of carpal fractures); the trapezoid is consistently the least frequently fractured carpal bone (classically under 1%).
- Reported cases cluster in young men after high-energy axial mechanisms (punch injury, falls on the flexed wrist, motor-vehicle trauma).
Side-by-side guideline principles
- Relevant Principle
- Clinically suspected carpal injury with normal radiographs should be immobilised and re-imaged or progressed to advanced imaging rather than discharged.
- Relevant Principle
- Cross-sectional imaging (CT) for occult or complex carpal fractures and pre-operative planning; anatomic reduction of displaced intra-articular carpal fractures.
- Relevant Principle
- Articular congruity and stable fixation of displaced carpal fractures; transarticular K-wires for associated CMC instability.
- Relevant Principle
- Low threshold for CT in high-energy wrist trauma and polytrauma to avoid missed carpal injuries among distracting fractures.
High- vs limited-resource practice variation
- Well-resourced settings: Ready CT access enables early detection and ORIF of displaced fractures and associated 2nd CMC dislocations; this is the main reason reported incidence is rising.
- Limited-resource settings: Reliance on plain radiographs means occult and undisplaced trapezoid fractures are frequently missed; immobilisation of the clinically suspicious wrist with delayed re-imaging is a reasonable strategy where CT is unavailable.
- Referral: Displaced fractures and fracture-dislocations warrant referral to a hand/upper-limb surgeon wherever the resource pathway allows.
Controversies & Areas of Uncertainty
The literature on trapezoid fractures is limited to case reports and small series, so several questions remain unresolved:
- Imaging threshold: There is no consensus on which patients with a "normal" radiograph warrant CT. Most authorities favour a low threshold for cross-sectional imaging given how often the injury is missed, but the cost-effectiveness of routine CT after axial index-ray trauma is undefined.
- Screw vs K-wire fixation: No comparative data exist for displaced fragments. Headless compression screws are preferred for fragments large enough to accept them; K-wires are used for comminuted or small fragments. Choice remains surgeon preference.
- Management of the associated 2nd CMC instability: Whether transarticular K-wiring alone, ligament repair, or temporary CMC fixation gives the best long-term result is unknown — the rarity of the injury precludes trials.
- True incidence: Historical "less than 1%" figures predate routine CT. The real incidence of occult, undisplaced trapezoid fractures is probably higher than classically reported, as several authors have argued.
- Late presentation: Optimal treatment of a missed/chronic trapezoid fracture or dislocation (delayed ORIF vs excision vs limited fusion) is not established.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your next step?”
“Answer the question.”
“Provide the ranking.”
MCQ Practice Points
Q: What is the rarest carpal bone to fracture? A: Trapezoid (less than 1% of carpal fractures).
Q: Where is the trapezoid located? A: Distal carpal row. Between the trapezium (radial) and capitate (ulnar). Articulates with the 2nd metacarpal distally.
Q: What is the typical mechanism for trapezoid fracture? A: Axial load through the 2nd metacarpal (e.g., punch injury, fall on flexed wrist).
Q: What is the most common associated injury with trapezoid fractures? A: 2nd CMC (carpometacarpal) fracture-dislocation.
Q: What imaging is best for trapezoid fractures? A: CT scan. X-rays often miss trapezoid fractures due to overlapping bones.
Key Facts
- Rarest carpal fracture
- less than 1% of carpal fractures
- Distal row (2nd CMC)
- Punch mechanism
Diagnosis
- X-ray often negative (overlap)
- CT is essential for diagnosis
- Tenderness at 2nd MC base
- Pain with axial load of index finger
Treatment
- Non-displaced: Short arm cast 4-6 weeks
- Displaced: ORIF via dorsal approach
- Fixation: Headless screws or K-wires
- Post-op: Cast 4-6 weeks, ROM after healing
Associated
- 2nd CMC dislocation (most common)
- Perilunate injuries (greater arc)
- Scaphoid fractures (high-energy)
- Multiple carpal fractures (assess entire carpus)
Evidence Base
Relative Incidence of Carpal Fractures
- Prospective audit of 1,000 consecutive hand fractures in Bergen, Norway over ~10 months.
- Carpal bones accounted for 18% of all hand fractures; the scaphoid alone made up 10.6% of the total series.
- Trapezoid fractures were essentially absent from this unselected series, confirming their status as the rarest carpal fracture.
Occult Undisplaced Trapezoid Fracture
- Two cases of isolated, undisplaced trapezoid fracture diagnosed with CT/MRI after negative or equivocal radiographs.
- Authors argue the lesion has historically been under-diagnosed and that modern cross-sectional imaging makes detection more frequent.
- Both undisplaced fractures healed with immobilisation alone.
First True Isolated Trapezoid Fracture
- First reported isolated trapezoid fracture with NO accompanying dislocation or associated metacarpal, carpal or distal radius injury.
- Managed non-operatively with a favourable clinical outcome.
- Reviews presentation, diagnostic workup and treatment of trapezoid fractures generally.
Trapezoid Dislocation — Missed on Plain Films
- Isolated trapezoid dislocation following high-speed motor-vehicle trauma.
- Highlights that these injuries are commonly missed on standard radiographs.
- Management invariably required open reduction and internal fixation.
Palmar Trapezoid Dislocation in Polytrauma
- Rare palmar trapezoid dislocation with associated distal radius fracture in a major-trauma patient.
- Distracting injuries risk misdiagnosis or delayed diagnosis of the carpal component.
- ORIF performed after stabilisation of major injuries yielded satisfactory hand and wrist function.
2nd CMC Fracture-Dislocation with Trapezoid Fracture
- Dorsal 2nd CMC dislocation with trapezoid fracture plus a Rolando fracture after a road-traffic crash.
- Treated by closed reduction with percutaneous K-wires then CT-guided open trapezoid reduction and K-wire fixation.
- Literature review of 71 cases of injuries involving 2nd CMC dislocation; good pain-free outcome at 1 year.