Wound Healing
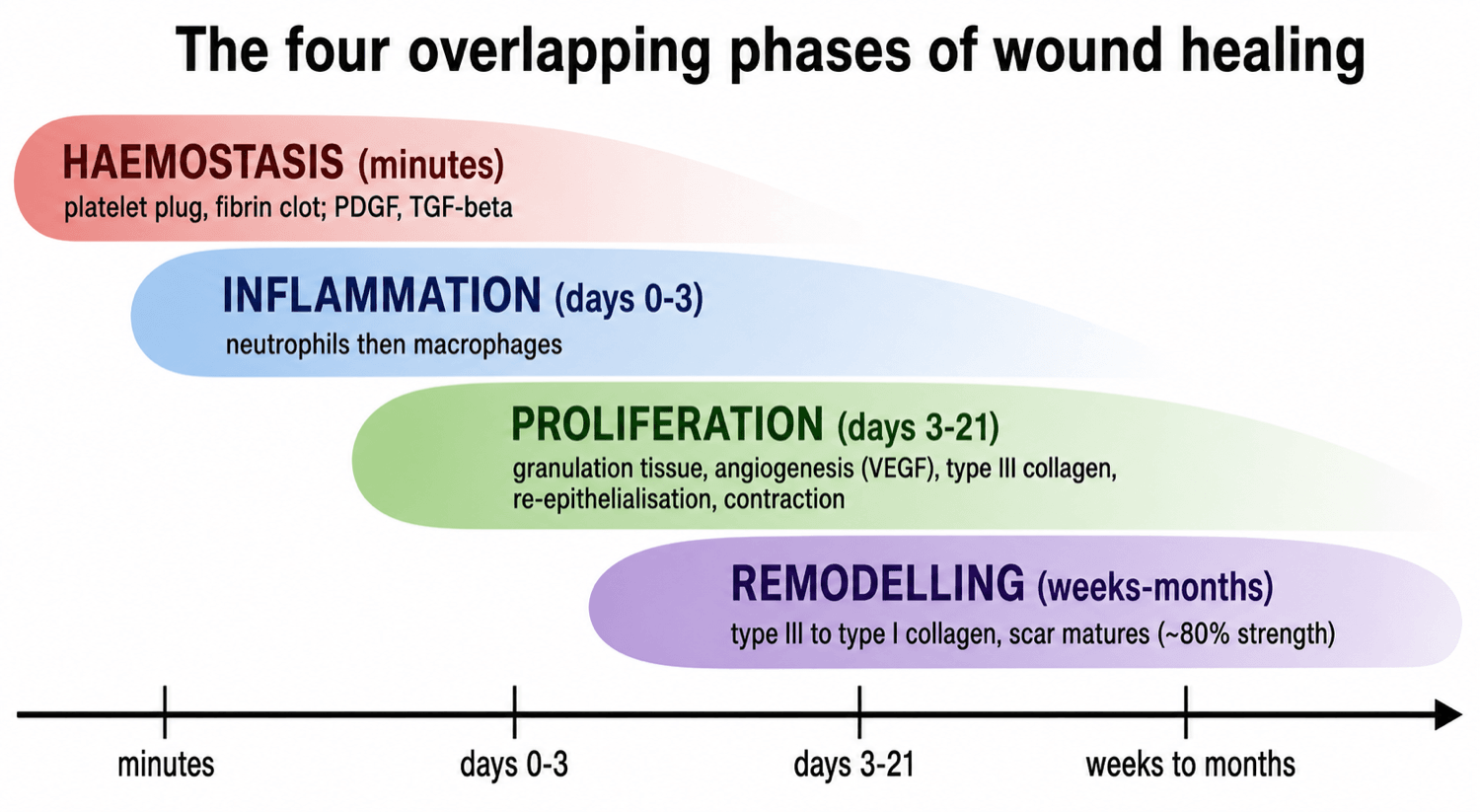
Know them in order and overlapping: haemostasis (clot, platelet plug), inflammation (neutrophils then macrophages), proliferation (granulation tissue, angiogenesis, re-epithelialisation, collagen synthesis) and remodelling (collagen reorganised and cross-linked over months). They are a continuum, not separate boxes.
Platelets start it (clot plus first growth factors). Neutrophils clear bacteria early. Macrophages are the master regulators - they clear debris and then drive repair. Fibroblasts lay down collagen, and myofibroblasts contract the wound.
Early scar is type III collagen, later remodelled to stronger type I. A scar never regains full strength - around 80 percent of normal at best. The wound is weakest at the end of the first week, the high-risk time for dehiscence.
Healing fails or slows with poor blood supply or hypoxia, infection, diabetes, smoking, corticosteroids, malnutrition, foreign material and excess tension. Chronic wounds are stuck in inflammation and never reach proliferation.
Overview
Wound healing is the body's organised response to tissue injury. After any cut, surgical incision, ulcer or open injury, a predictable sequence of events restores the protective barrier and structural integrity of the tissue. For most adult soft tissues and skin this is repair - the wound is filled with a fibrous scar - rather than true regeneration of the original organised tissue.
The process is usually described as four overlapping phases: haemostasis, inflammation, proliferation and remodelling. They are not separate, tidy steps; they blend into one another, and different parts of the same wound can be in different phases at the same time.
For the exam, three threads recur throughout this topic and are worth holding onto: the phases and their key cells (a classic basic-science viva), how a surgical wound closed by primary intention differs from an open wound healing by secondary intention, and why healing fails - the long list of local and systemic factors that examiners love, because they are exactly what you manipulate at the bedside.
Principles: The Four Phases of Healing
- Timing
- Immediate (minutes)
- What happens
- Vasoconstriction, platelet plug, fibrin clot forms a provisional matrix
- Key cells / mediators
- Platelets, clotting cascade, fibrin
- Timing
- Day 0 to about day 3
- What happens
- Clear bacteria and debris; recruit and activate repair cells
- Key cells / mediators
- Neutrophils first, then macrophages; histamine, cytokines
- Timing
- About day 3 to day 21
- What happens
- Granulation tissue, new vessels, re-epithelialisation, collagen synthesis
- Key cells / mediators
- Macrophages, fibroblasts, endothelial cells, keratinocytes
- Timing
- Weeks to many months
- What happens
- Collagen reorganised and cross-linked, type III replaced by type I, scar matures
- Key cells / mediators
- Fibroblasts, myofibroblasts, matrix metalloproteinases
1. Haemostasis - stopping the bleeding
Within seconds of injury, damaged vessels constrict and exposed collagen activates platelets. The platelets aggregate and the clotting cascade lays down fibrin, forming a clot that both stops bleeding and acts as a provisional matrix (a scaffold) for cells to migrate along. Activated platelets also release the first wave of growth factors - notably platelet-derived growth factor (PDGF) and transforming growth factor-beta (TGF-beta) - that recruit inflammatory cells and start the repair signal.
2. Inflammation - cleaning the wound
Over the first few days, blood vessels become leaky and inflammatory cells flood in. Neutrophils arrive first (peaking at roughly 24 to 48 hours) to kill bacteria and clear debris. Macrophages then take over (peaking around days 2 to 3) and are the central orchestrating cell: they finish the clearance, then switch to a reparative phenotype and release the growth factors that drive angiogenesis and fibroblast activity. A wound that cannot move on from this phase becomes a chronic wound.
3. Proliferation - rebuilding the tissue
This is where the wound is filled in, and it has several parallel processes:
- Granulation tissue forms - the red, granular wound bed made of new capillaries plus fibroblasts in a loose collagen matrix.
- Angiogenesis - endothelial cells sprout new capillaries (driven by vascular endothelial growth factor, VEGF) to supply the metabolically active wound.
- Fibroplasia - fibroblasts migrate in and lay down type III collagen and ground substance.
- Re-epithelialisation - keratinocytes migrate from the wound edges and skin appendages across the granulation tissue to restore the surface barrier.
- Wound contraction - some fibroblasts become myofibroblasts (expressing smooth-muscle actin) and pull the wound edges together, shrinking the defect.
4. Remodelling - making the scar
The longest phase, lasting months to over a year. The disorganised type III collagen of the early scar is gradually replaced and cross-linked into stronger, better-aligned type I collagen, while excess capillaries and cells regress (the scar pales and flattens). The balance between collagen synthesis and its breakdown by matrix metalloproteinases determines the final result. Even a well-healed scar regains only about 80 percent of the original tissue's tensile strength.
Growth Factors and Collagen
A small group of growth factors are worth knowing by name, because examiners ask which cell makes them and what they do:
- Main source
- Platelets, macrophages
- Main role
- Recruits and activates fibroblasts and macrophages; early repair signal
- Main source
- Platelets, macrophages
- Main role
- Drives fibroblast collagen synthesis - central to scar formation and fibrosis
- Main source
- Macrophages, endothelial cells
- Main role
- Drives angiogenesis - the new capillaries of granulation tissue
- Main source
- Macrophages, fibroblasts
- Main role
- Stimulates fibroblasts, angiogenesis and re-epithelialisation
- Main source
- Platelets, keratinocytes
- Main role
- Drives keratinocyte proliferation and re-epithelialisation
The collagen story is high-yield: the wound starts with type III collagen (laid down quickly but mechanically weak) and, during remodelling, this is steadily replaced by type I collagen, which is stronger and better organised. The shift in the type I to type III ratio back toward normal is a marker of a maturing, strengthening scar. Vitamin C is essential here because it is a cofactor for the hydroxylation of proline and lysine during collagen synthesis - which is why scurvy causes wound breakdown.
Tendon (and ligament) heals differently from skin and is highly examinable in orthopaedics. It heals by two mechanisms that occur together:
- Extrinsic healing — cells and vessels invade from the surrounding tendon sheath and tissue. It is fast, but the price is adhesions that restrict gliding.
- Intrinsic healing — the tendon's own tenocytes (from the epitenon and endotenon) proliferate. It is slower but gives better gliding and fewer adhesions, and is favoured by an intact blood supply and motion.
It passes through the same broad phases — inflammatory (about the first week), proliferative/collagen-producing (about week 1 to 6, disorganised type III collagen), and remodelling/consolidation (about 6 weeks to a year, type III to type I with collagen aligning along the line of pull). The key clinical point is the strength timeline: the repair depends on the suture early and is at its weakest around the end of the first to second week (biological strength low, suture loosening), which is when it is most likely to rupture. Early controlled (protected) mobilisation rather than rigid immobilisation promotes intrinsic healing, improves collagen alignment and strength, and reduces adhesions — the rationale behind modern flexor-tendon rehabilitation protocols.
Primary, Secondary and Delayed Closure
- Primary intention
- Clean incision with edges apposed (sutured)
- Secondary intention
- Open wound with tissue loss left to heal from the base
- Primary intention
- Minimal
- Secondary intention
- Abundant - fills the defect
- Primary intention
- Little
- Secondary intention
- Marked (myofibroblasts)
- Primary intention
- Fast, fine scar
- Secondary intention
- Slow, larger scar, higher infection risk
Tertiary intention (delayed primary closure) sits in between: the wound is deliberately left open for a few days - to let contamination, swelling or doubtful tissue viability declare themselves - and then closed surgically once it is clean and safe. This is common in contaminated trauma wounds and in compartment syndrome fasciotomies.
A closed surgical incision heals by primary intention with very little granulation tissue, so the visible "wound bed" of granulation tissue you see in an open wound or ulcer is the picture of secondary-intention healing. Recognising granulation tissue is a common clinical-photo question.
When a defect cannot simply be apposed, surgeons climb the reconstructive ladder from simplest to most complex: secondary-intention healing → direct primary closure → delayed primary closure → split-thickness skin graft → full-thickness skin graft → local/regional flap → free (microvascular) flap (in practice the best option is chosen, not just the lowest rung — the "reconstructive elevator").
- Skin grafts have no blood supply of their own and survive off the recipient bed in three stages: imbibition (plasmatic nutrition, the first day or two), inosculation (graft and bed capillaries link up, around days 2 to 3), then revascularisation (new vessel ingrowth, around days 4 to 7). A graft therefore needs a clean, vascularised bed and will NOT take on bare cortical bone, bare tendon or exposed metalwork.
- Split-thickness grafts (epidermis plus part of the dermis) cover large areas and the donor re-epithelialises, but they contract more and are less durable; full-thickness grafts (epidermis plus the full dermis) contract less and wear better but need a directly-closed donor and a better bed.
- Flaps carry their own blood supply, so they can cover an avascular bed — exposed bone, tendon without paratenon, an implant, an open joint or a major vessel/nerve — and are the answer for a high-grade open fracture needing soft-tissue coverage (the "fix and flap" principle).
Factors That Impair Healing
Examiners group these into local and systemic factors - a clean framework that scores well.
Poor blood supply / hypoxia, infection (the commonest local cause of failure), excess tension on the closure, foreign material or necrotic tissue, dead space and haematoma, and repeated trauma or pressure (for example pressure ulcers).
Diabetes, smoking (vasoconstriction and hypoxia), corticosteroids and immunosuppression, malnutrition (protein, vitamin C, zinc), older age, obesity, renal or liver failure, chemotherapy and radiotherapy, and peripheral vascular disease.
Factors affecting wound healing
- Successful healing requires the four phases (haemostasis, inflammation, proliferation, remodelling) to occur in the correct sequence and time frame
- Many factors interfere with one or more phases and so cause impaired healing
- Reviewed modifiers include oxygenation, infection, age and sex hormones, stress, diabetes, obesity, medications, alcohol, smoking and nutrition
- Most impaired wounds are stalled by a disrupted or prolonged inflammatory phase
Smoking is one of the most important and most modifiable risk factors for wound problems in orthopaedic and arthroplasty surgery. Nicotine causes vasoconstriction and tissue hypoxia and impairs collagen synthesis, raising the risk of wound breakdown, infection and (in fractures and fusions) non-union. Where possible, stop smoking before elective surgery.
Abnormal Scars and Chronic Wounds
When healing goes wrong it tends to fail in one of two directions - too much scar, or no progress at all:
- Hypertrophic scar
- Stays within the original wound boundary
- Keloid
- Grows beyond the original wound boundary
- Hypertrophic scar
- Soon after injury, often regresses with time
- Keloid
- Can appear later, persists and recurs
- Hypertrophic scar
- Across joints and high-tension areas
- Keloid
- More common in darker skin; sternum, shoulders, earlobes
- Hypertrophic scar
- Lower
- Keloid
- High - excision alone often makes it worse
A chronic wound is one that has failed to heal in the expected time, typically because it is stuck in a prolonged inflammatory phase and never progresses to proliferation and remodelling. Common examples are diabetic foot ulcers, venous and pressure ulcers, and infected surgical wounds. Management aims to restart the process: debride non-viable tissue, control infection and pressure, improve blood supply, and optimise systemic factors.
Clinical Relevance
Wound healing underpins almost everything in orthopaedic practice. Every surgical incision relies on it, and a wound complication after a joint replacement or fracture fixation can be the gateway to deep infection and disaster. In trauma, the decision to close a wound primarily, leave it open, or use delayed closure is a daily judgement that flows directly from these principles. In basic-science vivas, the phases, key cells and growth factors, and the local-versus-systemic list of impairing factors are classic, examinable material. And at the bedside, the things that most improve healing - good blood supply, no infection, controlled diabetes, no smoking, adequate nutrition, and a tension-free closure - are exactly the modifiable factors this topic teaches.
Guidelines, Registries and Global Practice
- Surgical site infection prevention guidance worldwide (for example WHO global guidelines and NICE in the UK) targets exactly the modifiable wound-healing factors - perioperative glycaemic control, smoking cessation, normothermia, tissue oxygenation and tension-free closure - because these protect the healing wound from breakdown and infection.
- Diabetic foot ulcer care is standardised across major bodies (such as the International Working Group on the Diabetic Foot and national diabetes societies), centred on debridement, offloading pressure, infection control, vascular assessment, and good glycaemic control - the practical application of restarting a stalled wound.
- Negative pressure wound therapy (NPWT) is widely endorsed as an adjunct for open, exuding and difficult wounds, promoting granulation and contraction; the strongest randomised evidence is in diabetic foot and complex surgical wounds.
- Across all settings the principle is the same: healing is a biological process you support rather than force - keep the wound clean, perfused and tension-free, and correct the systemic factors that hold it back.
Memory aids
HIPRThe Phases in Order
Hook:HIPR - Haemostasis, Inflammation, Proliferation, Remodelling, in the order they happen.
DIDNT HEALFactors That Impair Healing
Hook:A wound that DIDNT HEAL - run through the systemic and local reasons one by one.
123Healing by Intention
Hook:1-2-3: edges together, fill from the bottom, or close later when clean.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows you a healing open wound with a red granular base and asks you to take them through how a wound heals.”
“A 62-year-old man with type 2 diabetes who smokes has a surgical wound on the leg that is still open and discharging six weeks after a fracture fixation. How do you think about and manage this?”
The Four Phases
- Haemostasis: clot, platelet plug, provisional fibrin matrix (immediate)
- Inflammation: neutrophils first, then macrophages (days 0 to 3)
- Proliferation: granulation tissue, angiogenesis, re-epithelialisation, collagen (days 3 to 21)
- Remodelling: type III to type I collagen, scar matures (weeks to months)
Key Cells and Factors
- Macrophage: master regulator - clears debris then drives repair
- Myofibroblast: contracts the wound
- PDGF and TGF-beta: fibroblast recruitment and collagen
- VEGF: angiogenesis; vitamin C: collagen cofactor
Closure and Strength
- Primary intention: edges together, minimal granulation, fine scar
- Secondary intention: open, granulation and contraction, big scar
- Tertiary: delayed primary closure when clean
- Scar regains about 80 percent of strength; weakest at end of week 1
What Impairs Healing
- Local: infection, hypoxia, tension, foreign material, dead space
- Systemic: diabetes, smoking, steroids, malnutrition, age, vascular disease
- Chronic wound: stuck in prolonged inflammation
- Modifiable wins: control diabetes, stop smoking, treat infection, nutrition
Evidence and Mechanisms
Every citation below has been checked against its source record in PubMed. Peña & Martin give the modern immune-orchestrated, multi-cell picture of the phases; the Dalmedico meta-analysis is the randomised evidence for negative-pressure wound therapy in stalled diabetic foot ulcers; and the Guo & DiPietro review (cited in the impaired-healing section) catalogues the local and systemic modifiers you can actually change at the bedside.
Cellular and molecular mechanisms of skin wound healing
- Healing requires tightly coordinated cell migration, proliferation, matrix deposition and remodelling alongside inflammation and angiogenesis
- Small wounds heal in days, while large traumatic or surgical wounds take weeks and usually leave a fibrotic scar
- Both innate and adaptive immune cells shape the behaviour of keratinocytes, fibroblasts and endothelial cells
- Understanding these mechanisms is the basis for therapies to reduce scarring and heal chronic wounds
Negative Pressure Wound Therapy for Diabetic Foot Ulcers (Systematic Review)
- Systematic review and meta-analysis of randomised controlled trials of negative pressure wound therapy (NPWT) in diabetic foot ulcers
- Fourteen trials reviewed; NPWT showed superior total wound healing where this outcome was reported
- Most trials comparing wound area reduction favoured NPWT over standard care
- Authors note methodological limitations and heterogeneity but a consistent potential benefit