foot ankle
Hallux Rigidus
intermediate
6 min
28 marks
6 questions
Clinical Scenario
A 58-year-old male accountant presents with progressive pain and stiffness of his right great toe over 2 years. He reports pain with walking, especially push-off, and difficulty squatting. He cannot wear dress shoes due to dorsal prominence. He has tried NSAIDs and orthotics with minimal relief. He is active and wants to maintain recreational walking.
Clinical examination reveals palpable dorsal osteophyte at the first MTP joint, with dorsiflexion limited to 20° (contralateral 60°) and pain at end-range. The plantar aspect of the joint is relatively preserved. There is no significant hallux valgus. Gait shows shortened stride with early heel-off.
Weight-bearing radiographs are provided.
Clinical examination reveals palpable dorsal osteophyte at the first MTP joint, with dorsiflexion limited to 20° (contralateral 60°) and pain at end-range. The plantar aspect of the joint is relatively preserved. There is no significant hallux valgus. Gait shows shortened stride with early heel-off.
Weight-bearing radiographs are provided.
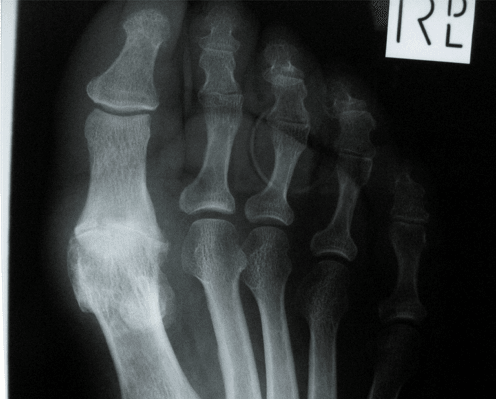
Clinical image for Hallux Rigidus
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Question 1 (4 marks)
What is hallux rigidus? Describe the aetiology and pathophysiology.
Question 2 (5 marks)
How would you classify hallux rigidus? What clinical and radiographic features differentiate each grade?
Question 3 (6 marks)
Describe the non-operative and operative treatment options. What factors influence your surgical decision?
Question 4 (5 marks)
Describe your technique for cheilectomy. What defines an adequate procedure?
Question 5 (4 marks)
When would you recommend first MTP fusion? Describe your preferred technique and key principles.
Question 6 (4 marks)
What is the role of joint-sparing procedures beyond cheilectomy? Discuss Moberg osteotomy and interpositional arthroplasty.