Pilon Fractures (Tibial Plafond)
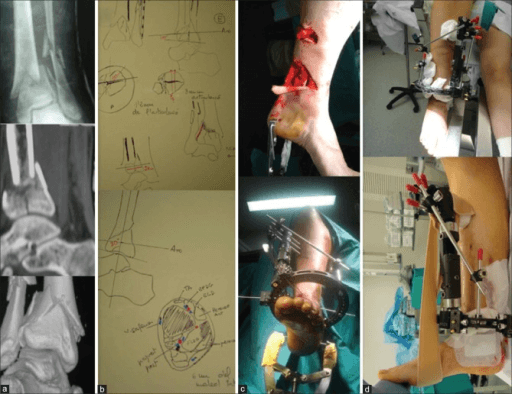
Coronal and sagittal CT reconstructions demonstrating a comminuted pilon fracture. The articular surface of the distal tibia is split into multiple fragments with central impaction (die-punch fragment). There is metaphyseal comminution and an associated fibular fracture. The talus has driven upward creating the 'explosion' injury pattern. This high-energy injury requires staged management.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the mechanism and classification of pilon fractures.
Explain the staged management approach.
Describe the surgical technique for definitive ORIF.
What are the soft tissue considerations?
Discuss complications and their prevention.
What are the outcomes and salvage options?
Must Mention
- •Pilon = "pestle" (axial load)
- •Staged management: ex-fix → wait → ORIF
- •Wrinkle test for timing (10-21 days)
- •Ruedi-Allgower 4 steps
- •Skin bridge ≥7cm between incisions
- •50%+ develop arthritis
Common Pitfalls
- •Operating too early
- •Not recognizing soft tissue injury
- •Missing compartment syndrome
- •Insufficient bone grafting
- •Wrong incision planning
- •Not knowing staged approach