Lumbar Disc Herniation
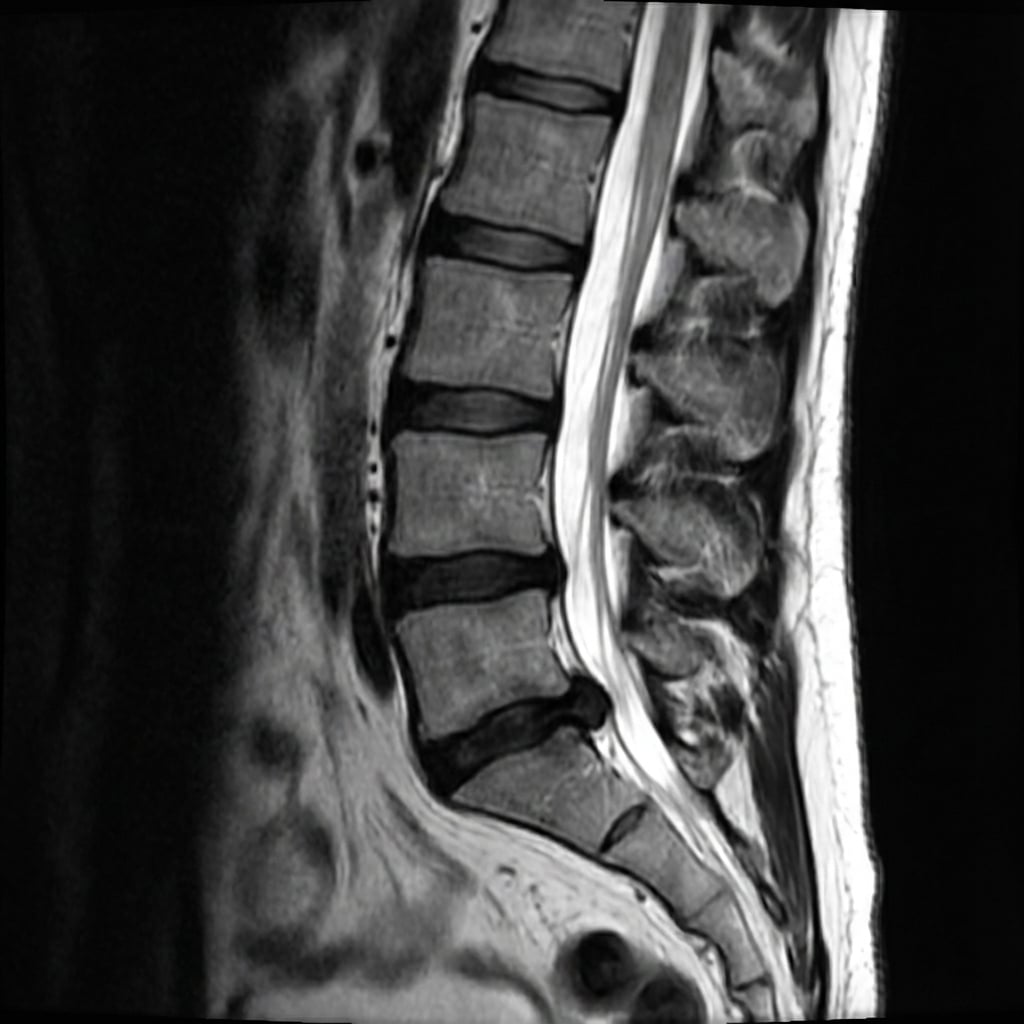
Sagittal and axial T2-weighted MRI demonstrating large left paracentral disc herniation at L5-S1. The disc fragment is extruded and extends inferiorly, compressing the left S1 nerve root in the lateral recess. There is loss of disc height and disc desiccation. The patient has left S1 radiculopathy with calf pain and absent ankle jerk.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the MRI findings and correlate with the clinical presentation.
What is the natural history and what are the indications for surgery?
Describe your surgical technique for microdiscectomy.
What are the potential complications and how do you prevent them?
What clinical features would suggest a different level of herniation?
What alternative surgical techniques exist and what is the evidence?
Must Mention
- •L5-S1 paracentral = S1 root (traversing)
- •Natural history: 90% improve without surgery
- •Conservative trial: 6-12 weeks
- •Absolute indications: CES, progressive motor deficit
- •Confirm level intraoperatively
- •Recurrence rate: 5-10%
- •Preserve >50% facet to prevent instability
Common Pitfalls
- •Wrong root correlation
- •Operating too early
- •Wrong level surgery
- •Excessive facet removal
- •Missing CES indications
- •Not recognizing natural history