Acute Spinal Cord Injury
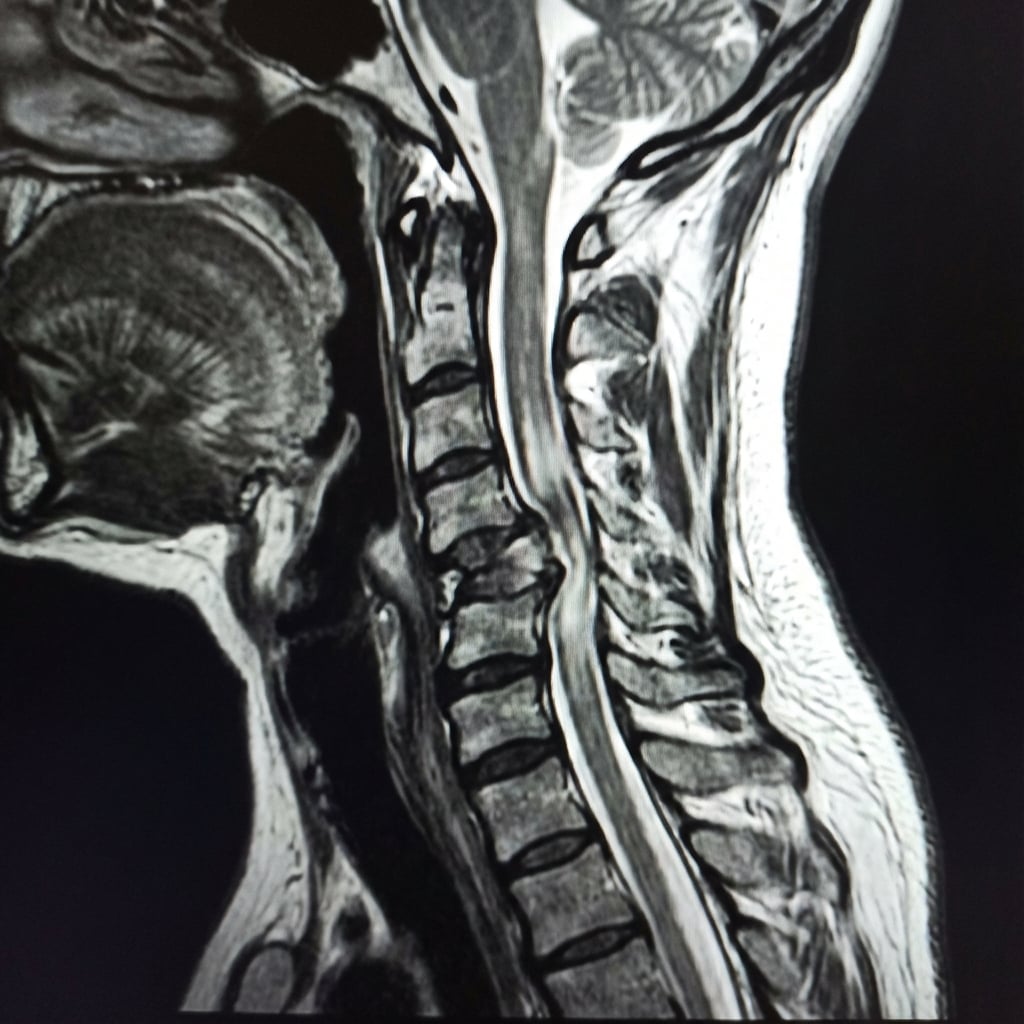
Sagittal T2-weighted MRI demonstrating C5-6 fracture-dislocation with anterior translation of C5 on C6. There is severe spinal cord compression with intramedullary T2 hyperintensity extending from C4 to C7 consistent with cord edema and contusion. The posterior ligamentous complex is disrupted. This represents complete spinal cord injury at C5 level.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the imaging findings and classify this injury.
Explain the ASIA classification and what is the neurological level?
How do you manage neurogenic shock and what is the initial resuscitation?
What is the evidence for timing of surgery and role of steroids?
What are the acute complications and how do you prevent them?
What are the expected outcomes and rehabilitation considerations?
Must Mention
- •ASIA classification (A = complete, B-D = incomplete)
- •Sacral sparing = incomplete (check S4-5 sensation, anal tone)
- •Neurogenic shock = hypotension + bradycardia
- •MAP ≥85 mmHg for 5-7 days
- •STASCIS: early surgery (<24h) = better outcomes
- •Steroids NOT standard of care
- •DVT prophylaxis mandatory
Common Pitfalls
- •Confusing shock types
- •Wrong ASIA classification
- •Steroids as standard
- •Delayed surgery
- •Missing respiratory monitoring
- •Forgetting DVT prophylaxis