Lumbar Spinal Stenosis
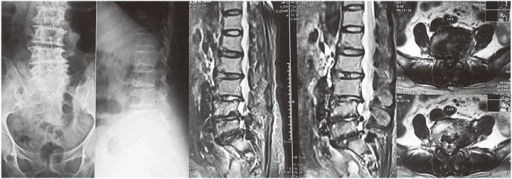
Axial and sagittal T2-weighted MRI demonstrating severe central canal stenosis at L4-5 with trefoil-shaped canal. There is bilateral ligamentum flavum hypertrophy, facet joint hypertrophy, and disc bulge causing circumferential compression of the cauda equina. Multiple levels show degenerative changes. This represents degenerative lumbar spinal stenosis causing neurogenic claudication.
Source: Sacral Insufficiency Fractures Mimicking Lumbar Spine Pathology • PMC4917777 • CC-BY
Questions
Describe the MRI findings and classify this stenosis.
What are the clinical features and how do you differentiate from vascular claudication?
What is the evidence for treatment and when do you recommend surgery?
Describe your surgical technique for decompression.
When is fusion indicated and what are the fusion options?
What are the expected outcomes and complications?
Must Mention
- •Neurogenic claudication: positional, bicycle test positive
- •Vascular: cramping, relieved by standing still
- •SPORT trial: surgery superior for stenosis
- •Decompression alone if no spondylolisthesis
- •Fusion if spondylolisthesis or instability
- •Preserve facets (<50%) to prevent instability
Common Pitfalls
- •Missing vascular claudication
- •Not knowing SPORT
- •Unnecessary fusion
- •Excessive facet removal
- •Incomplete lateral decompression
- •Missing instability