Metastatic Spinal Cord Compression
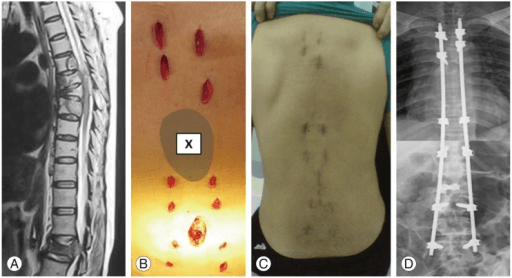
Sagittal T2-weighted MRI demonstrating T8 vertebral body collapse with posterior cortex retropulsion causing spinal cord compression. There is high signal within the cord at this level indicating edema/myelopathy. The lesion replaces normal bone marrow signal and there is an associated soft tissue mass extending epidurally. Multiple other vertebral lesions are visible. This represents metastatic spinal cord compression (MSCC) requiring urgent assessment and treatment.
Source: Minimally Invasive Spinal Stabilization in Patients with Spinal Metastasis • PMC4764548 • CC-BY
Questions
Describe the MRI findings and explain the urgency of this condition.
What scoring systems are used to guide treatment decisions?
What are the treatment options and how do you decide between them?
Describe your surgical technique for thoracic decompression and stabilization.
What is the role of radiotherapy and when is it used alone?
What are the expected outcomes and prognostic factors?
Must Mention
- •MSCC = emergency - dexamethasone 16mg immediately
- •Tokuhashi (survival), Tomita (surgical goal), SINS (stability)
- •Ambulatory status = best predictor of outcome
- •Surgery + RT > RT alone (Patchell) if fit and >3 months survival
- •Radiosensitivity guides treatment (myeloma = RT, renal = surgery)
- •Separation surgery + SBRT for radioresistant tumors
Common Pitfalls
- •Delayed steroids
- •Not calculating scores
- •Surgery in poor prognosis patients
- •RT for radioresistant tumors
- •Missing instability
- •Not involving MDT