Thoracolumbar Burst Fracture
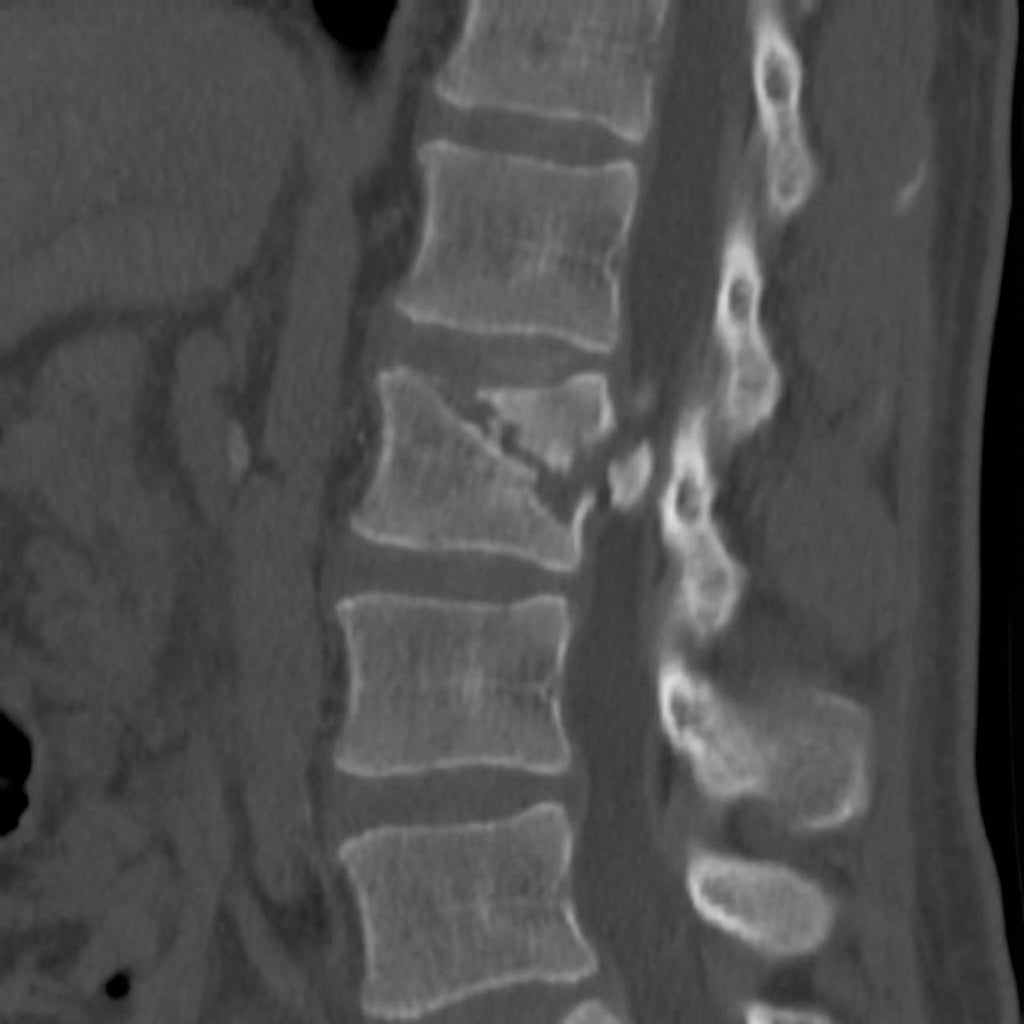
Sagittal and axial CT images demonstrating L1 burst fracture with loss of anterior vertebral body height, retropulsion of a posterior wall fragment causing 50% canal compromise, and widening of the interpedicular distance. The patient has an incomplete neurological deficit. This represents an unstable thoracolumbar junction injury requiring surgical stabilization.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the CT findings and classify this injury using TLICS.
What determines stability and how do you assess the posterior ligamentous complex?
What are the indications for surgery and what approach would you choose?
Describe your surgical technique for posterior instrumented fusion.
When is anterior surgery indicated and what is the technique?
What are the expected outcomes and rehabilitation considerations?
Must Mention
- •TLICS = Morphology + PLC + Neurology
- •TLICS ≥5 = surgical
- •PLC integrity - assess with MRI
- •Ligamentotaxis = distraction + lordosis
- •Posterior approach for most cases
- •Incomplete SCI = best recovery prognosis
- •2 above, 2 below for instrumentation
Common Pitfalls
- •Miscalculating TLICS
- •Missing PLC injury
- •Operating when non-op appropriate
- •Not using ligamentotaxis properly
- •Delayed surgery with neurological deficit
- •Inadequate follow-up imaging