Calcaneal Fracture
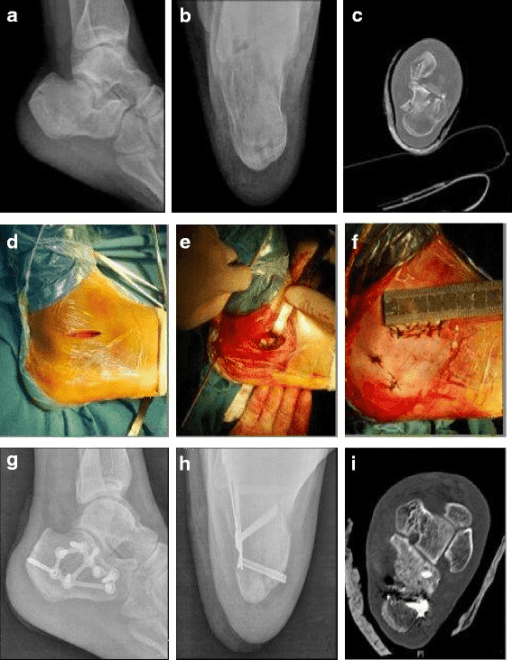
Lateral radiograph showing calcaneal fracture with decreased Bohler's angle (<10°) and loss of calcaneal height. CT coronal images demonstrate Sanders Type III fracture with 3 fragments of the posterior facet. Note widening of the calcaneal body and lateral wall blowout.
Source: Percutaneous cannulated screw fixation vs sinus tarsi approach for displaced intra-articular calcaneal fractures • Feng Y, Shui X, Wang J, et al. • PMC4946135 • CC-BY
Questions
What associated injuries must you assess for and why?
Describe the radiographic assessment including the Sanders classification.
The right heel has skin tenting posteriorly. How does this change your immediate management?
Discuss the evidence for operative versus non-operative treatment of calcaneal fractures.
Describe the surgical approach and key intraoperative steps.
What complications would you discuss with this patient?
Must Mention
- •10-15% spine fracture association - CHECK SPINE
- •Sanders classification (coronal CT, posterior facet fragments)
- •Bohler's angle: normal 20-40°, <20° = significant
- •Wrinkle test before ORIF (7-14 days)
- •Skin tenting = URGENT reduction
- •UK Heel Fracture Trial: no difference at 2 years
Common Pitfalls
- •Not checking spine (10-15% association)
- •ORIF before soft tissue recovery (wound complications)
- •Missing skin tenting as urgent
- •Operating on Sanders IV (consider primary fusion)
- •Missing foot compartment syndrome
- •Not discussing UK Heel Fracture Trial in counselling