Chronic Elbow Dislocation
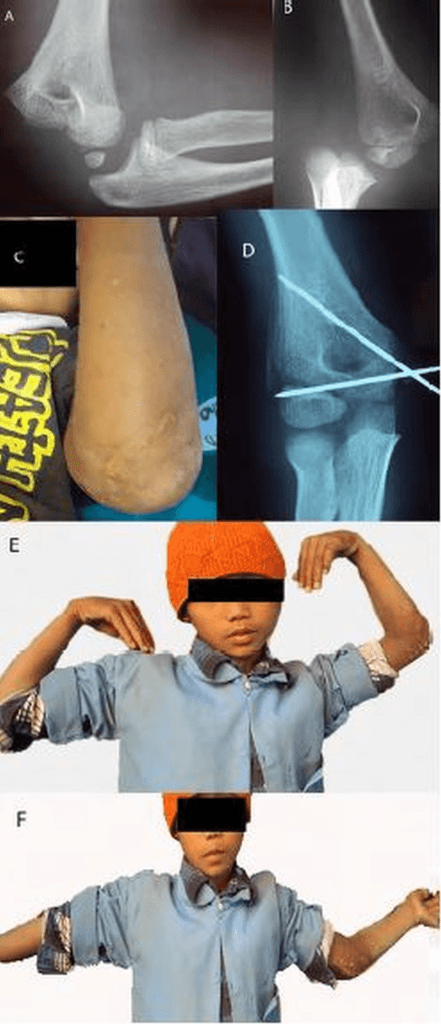
AP and lateral radiographs demonstrating chronic posterolateral elbow dislocation. There is heterotopic ossification around the joint, the coronoid is remodeled, and there is significant joint incongruity. The injury is 4 months old. The humeral trochlea shows early degenerative changes from chronic subluxation.
Source: Radiological and Functional Outcome of Medial Epicondyle Fracture Treated Surgically in Children • PMC5293142 • CC-BY
Questions
Describe the radiographic findings and define chronic elbow dislocation.
What are the blocks to closed reduction and why is open surgery required?
Describe your surgical approach and technique for open reduction.
What stabilization options are available after reduction?
How do you manage the ulnar nerve in this situation?
What are the expected outcomes and how do you counsel the patient?
Must Mention
- •Chronic = >3 weeks
- •Blocks: triceps, capsule, collaterals, HO, intra-articular fibrosis
- •Open reduction required
- •Ulnar nerve - identify FIRST, protect, consider transposition
- •Hinged external fixator if unstable
- •Goal is functional arc (30-130°), not full ROM
- •Outcome correlates with duration
Common Pitfalls
- •Attempting closed reduction
- •Not identifying ulnar nerve early
- •Not having hinged fixator available
- •Promising full ROM
- •Forcing reduction without adequate release
- •Missing HO on imaging (get CT)