Floating Elbow
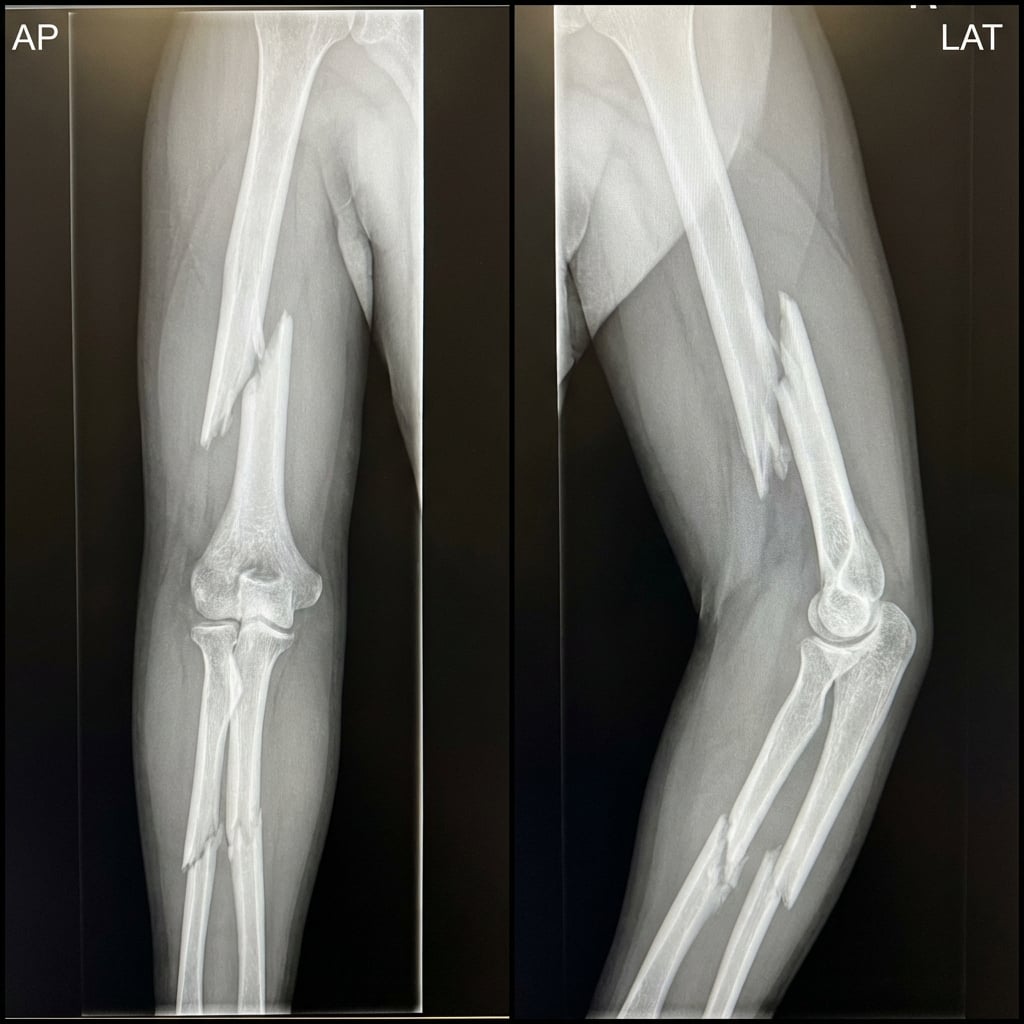
AP and lateral radiographs demonstrating displaced midshaft humerus fracture with spiral pattern and displaced both-bone forearm fracture in the same limb. The elbow joint appears concentrically reduced but without bony continuity to either shoulder or wrist. This is a floating elbow injury - a high-energy pattern with significant complication risk.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Define this injury pattern and what are your initial assessment priorities?
What is the significance of this injury pattern and what complications should you anticipate?
Describe your operative strategy for fixation of both fractures.
How do you manage the radial nerve palsy identified preoperatively?
What rehabilitation protocol do you follow and what are expected outcomes?
How does management differ in children with this injury pattern?
Must Mention
- •Document neuro status BEFORE manipulation
- •Fix BOTH fractures same sitting
- •Humerus first (limb stability)
- •Radial nerve palsy 15-20%, 90% recover
- •Early elbow ROM critical
- •Don't explore primary radial palsy routinely
Common Pitfalls
- •Not documenting neuro status pre-op
- •Exploring radial nerve unnecessarily
- •Fixing only one fracture
- •Delayed mobilization → stiffness
- •Missing compartment syndrome
- •Secondary palsy not explored