Patella Fracture
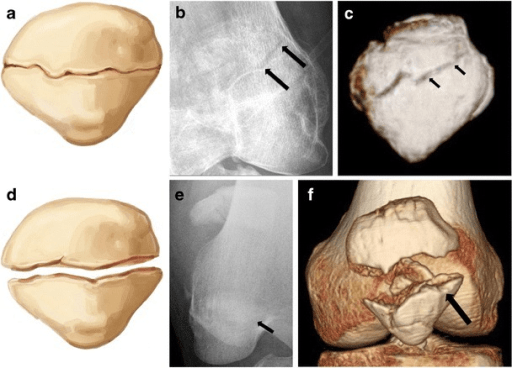
AP and lateral radiographs demonstrating displaced transverse patella fracture through the mid-portion with 5mm separation between fragments. The proximal pole is migrated superiorly due to quadriceps pull, indicating extensor mechanism disruption. Knee effusion is present.
Source: Imaging of Patellar Fractures: Transverse Fracture • PMC5265199 • CC-BY
Questions
Describe the radiographic findings and classify this fracture.
What clinical features determine operative versus non-operative management?
Describe the surgical techniques available and your tension band wiring technique.
What is the post-operative rehabilitation protocol?
What complications would you discuss and when would you remove hardware?
How does management differ for comminuted inferior pole fractures?
Must Mention
- •SLR = key clinical test for extensor mechanism
- •Surgery if: >2-3mm gap, unable to SLR, >2mm step
- •TBW converts tensile → compressive forces
- •Wire anterior to transverse axis of patella
- •Hardware prominence 20-30% (most common complication)
- •Early ROM essential
Common Pitfalls
- •K-wires posterior to transverse axis (lose TBW advantage)
- •Not repairing retinaculum
- •Delayed mobilization → stiffness
- •Not checking ROM in theatre
- •Attempting TBW for severely comminuted
- •Missing bipartite patella (check contralateral)