Pelvic Ring Injury
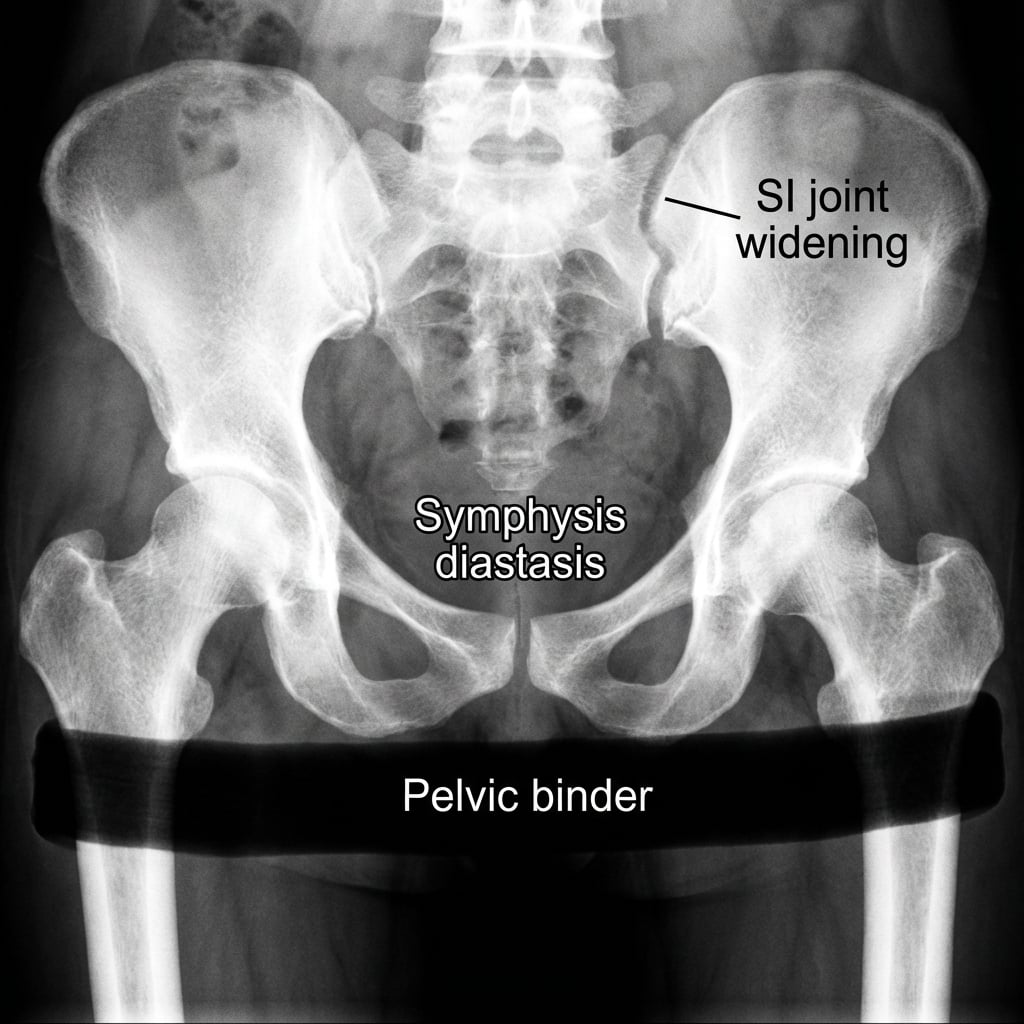
AP pelvis radiograph showing APC-III (open book) injury with symphysis pubis diastasis >2.5cm and widening of the left sacroiliac joint. The hemipelvis is externally rotated indicating complete posterior ring disruption. Pelvic binder in situ.
Source: Educational radiograph of an APC-III pelvic ring injury • OrthoVellum Medical Education Team • OrthoVellum Educational Use
Questions
Classify this pelvic injury using both Young-Burgess and Tile classifications. Describe the implications for hemorrhage.
Describe your immediate resuscitation priorities and the hemorrhage control algorithm.
There is blood at the urethral meatus. What associated injuries must you assess for?
The patient stabilizes after angioembolization. Describe your definitive fixation strategy.
What are the indications for emergent interventions? Describe REBOA, pelvic packing, and angioembolization.
What complications and long-term outcomes would you counsel the patient about?
Must Mention
- •Pelvic binder at GREATER TROCHANTERS (not iliac crests)
- •Blood at meatus = DO NOT catheterize until retrograde urethrogram
- •MTP 1:1:1 ratio; avoid crystalloid boluses
- •80% venous (packing), 20% arterial (angio)
- •Posterior ring fixation is priority (SI screws)
- •APC injuries respond best to binder (reduces volume)
Common Pitfalls
- •Pelvic binder at iliac crests (should be at trochanters)
- •Urethral catheter with blood at meatus
- •Repeated pelvic spring test (increases bleeding)
- •Crystalloid boluses (dilutional coagulopathy)
- •Anterior-only fixation for unstable (Type C) injury
- •Operating before physiological optimization