Polytrauma and Damage Control Orthopaedics
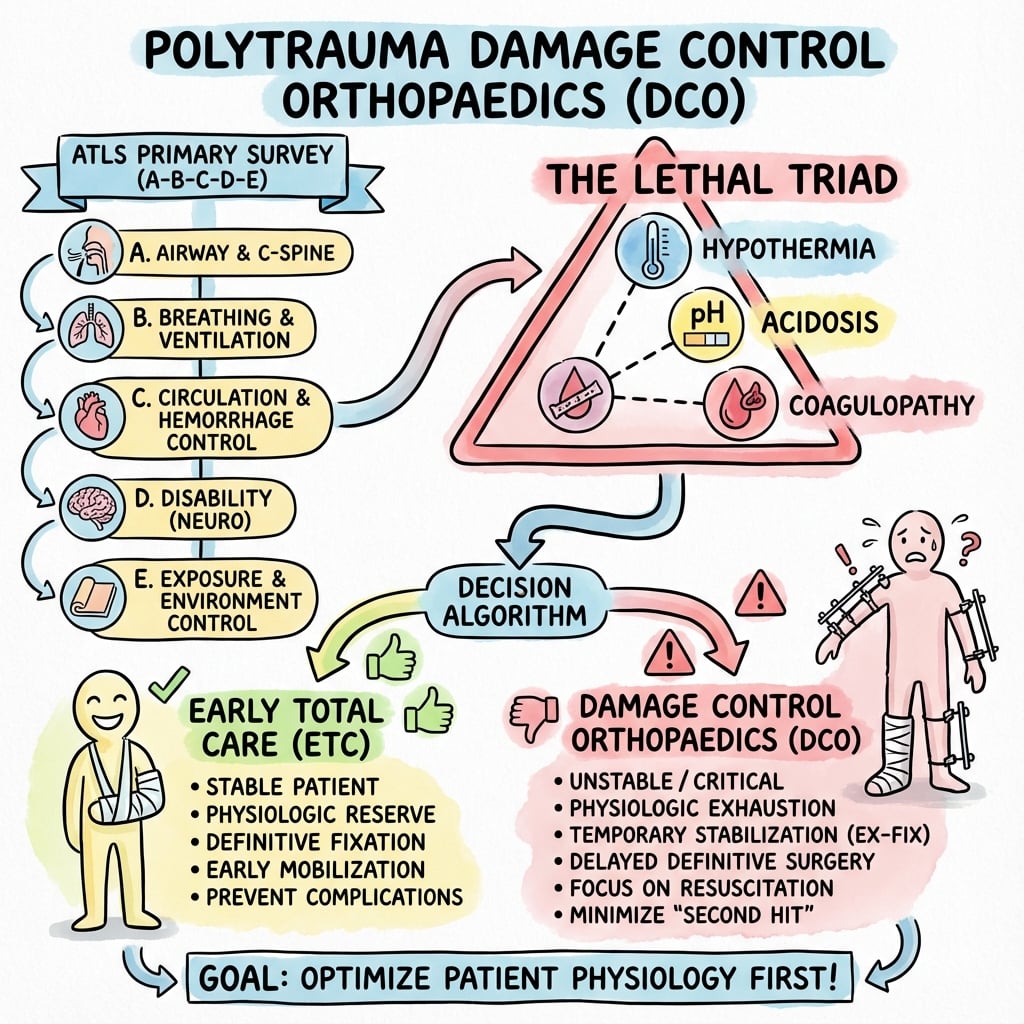
Diagram showing ATLS primary survey approach (A-B-C-D-E) with decision algorithm for Damage Control Orthopaedics versus Early Total Care based on physiological parameters (lethal triad: hypothermia, acidosis, coagulopathy).
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe your immediate management priorities in order for this patient.
Define Damage Control Orthopaedics (DCO) and explain the indications and rationale in this patient.
Describe your acute orthopaedic surgical management plan.
What parameters would you monitor and when would you proceed to definitive fixation?
The patient develops increasing oxygen requirements and confusion 48 hours post-injury. What is your differential and management?
Describe complications specific to polytrauma and how to prevent/manage them.
Must Mention
- •ATLS order: A-B-C-D-E (tension pneumothorax before ortho)
- •Lethal triad: hypothermia (<35°C), acidosis (pH <7.25), coagulopathy (INR >1.5)
- •"Second hit" phenomenon
- •DCO: temporary ex-fix → convert to IM nail in window (days 5-10)
- •Convert external fixator within 2 weeks (infection risk)
- •Fat embolism syndrome: hypoxia, confusion, petechiae at 24-72 hours
Common Pitfalls
- •ORIF in unstable patient (second hit → ARDS, MODS, death)
- •Not recognizing lethal triad (hypothermia, acidosis, coagulopathy)
- •Orthopaedics before life-threatening injuries (ATLS order)
- •Not applying pelvic binder early
- •Converting ex-fix to nail too late (>2 weeks = infection)
- •Missing fat embolism syndrome (confusion + hypoxia 24-72h)
- •Not doing tertiary survey for missed injuries
- •Not monitoring for compartment syndrome