Posterior Sternoclavicular Joint Dislocation
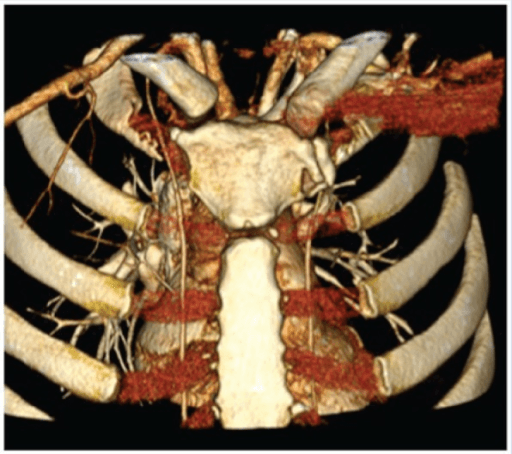
Axial CT scan demonstrating posterior displacement of the medial clavicle behind the sternum. The displaced clavicle is in close proximity to the trachea, esophagus, and great vessels. There is soft tissue swelling anteriorly. This represents a potentially life-threatening injury requiring reduction in a controlled setting with cardiothoracic backup.
Source: Posterior Sternoclavicular Dislocation in Professional Athlete • PMC4481669 • CC-BY
Questions
Describe the imaging findings and classify this injury.
What mediastinal structures are at risk and what symptoms might indicate injury?
Describe your approach to closed reduction of this injury.
When is open reduction required and what is your surgical technique?
How do you manage chronic posterior SCJ dislocation?
What stabilization options are available and what is your follow-up protocol?
Must Mention
- •Posterior SCJ = life-threatening (mediastinal structures at risk)
- •ALWAYS CT scan for posterior dislocation
- •Reduce in theatre with cardiothoracic standby
- •Abduction-extension with sandbag between scapulae
- •NO K-wires (fatal migration to heart)
- •Chronic (>3 weeks) = reconstruction required
- •Medial clavicle physis fuses last (23-25 years)
Common Pitfalls
- •Not recognizing severity (posterior = dangerous)
- •Not getting CT
- •Reducing without cardiothoracic backup
- •Using K-wires for stabilization
- •Missing symptoms of compression
- •Treating chronic like acute