Tibial Shaft Fracture
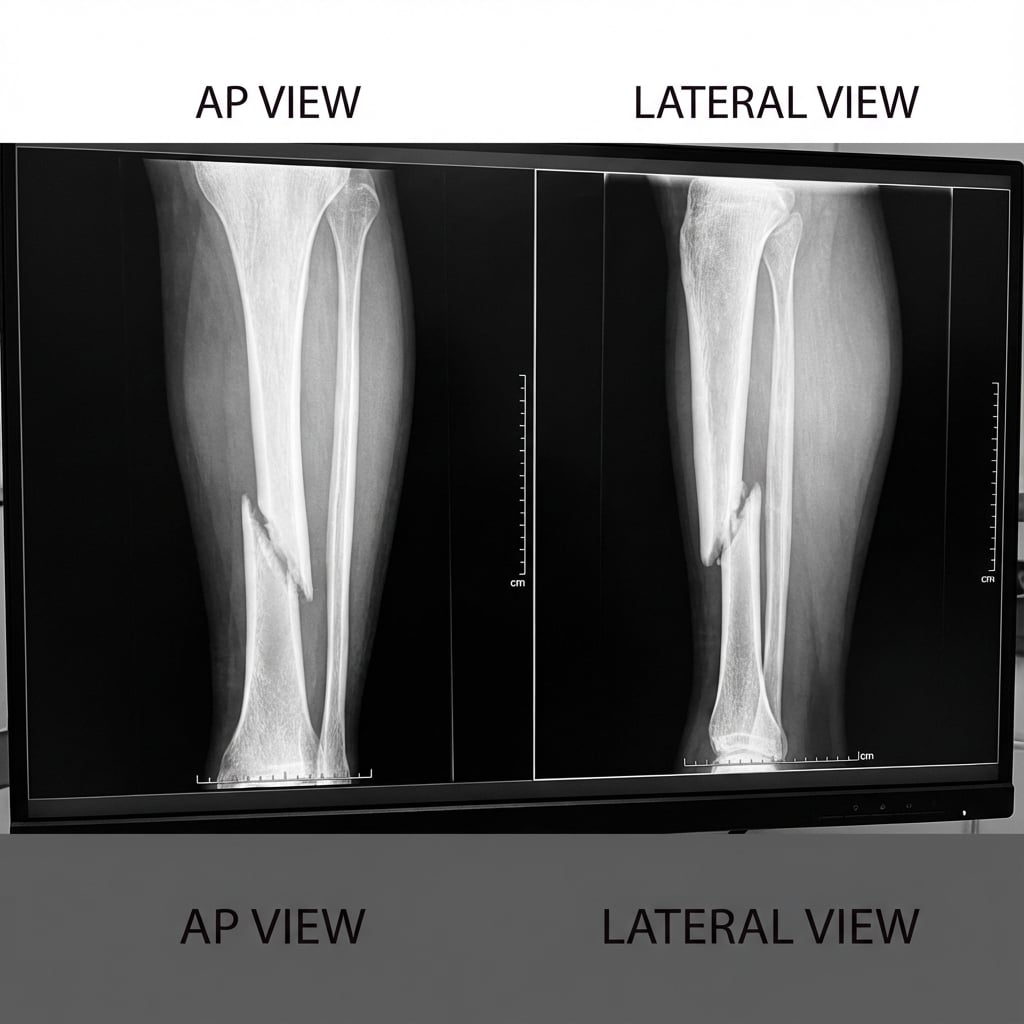
AP and lateral radiographs demonstrating displaced spiral fracture of the tibial shaft at the junction of middle and distal thirds with intact fibula. Approximately 1cm shortening with minimal angulation. The spiral pattern suggests a rotational mechanism with relatively low energy.
Image source: Open Access medical literature (NIH/PubMed Central) • CC-BY License
Questions
Describe the radiographic findings and classify this fracture.
What are your clinical concerns and how do you assess them?
What are the treatment options and describe your preferred surgical technique?
What is the significance of the intact fibula and how do you manage it?
What complications would you discuss and what are the expected outcomes?
How does the management differ for proximal and distal third fractures?
Must Mention
- •IM nail = gold standard (>95% union)
- •Intact fibula = varus malunion risk
- •Compartment syndrome assessment (5 Ps)
- •Entry point determines alignment
- •Blocking screws for proximal/distal fractures
- •Rotation check essential (compare contralateral)
Common Pitfalls
- •Not assessing for compartment syndrome serially
- •Rotational malalignment (check clinically)
- •Wrong entry point causing deformity
- •Not using blocking screws for metaphyseal extension
- •Missing open wound (small lacerations)
- •Not checking ankle/knee for associated injury