trauma
Vascular Injury with Knee Dislocation
advanced
6 min
28 marks
6 questions
Clinical Scenario
A 22-year-old man presents following a motor vehicle collision. He had a posterior knee dislocation that was reduced in the Emergency Department. On examination, the knee is now reduced but the foot is pale, cold, and pulseless. He can wiggle his toes but sensation is diminished in the foot.
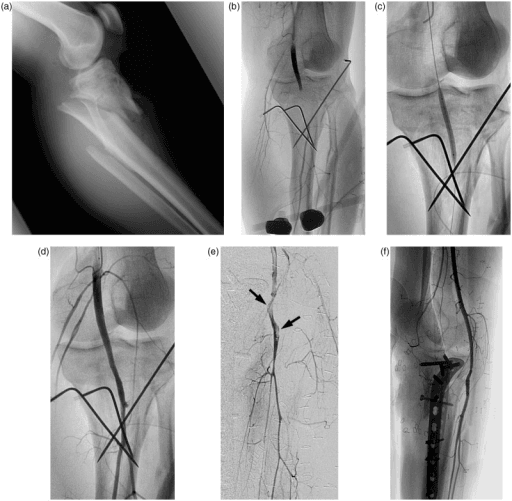
Post-reduction radiographs showing concentrically reduced knee joint. Clinical photograph demonstrates pale, cold foot with absent pulses indicating popliteal artery injury. The combination of knee dislocation and limb ischemia represents a limb-threatening emergency requiring immediate intervention.
Source: Popliteal Artery Injury Angiogram • PMC4001432 • CC-BY
Questions
Question 1 (4 marks)
What is the diagnosis and what is the urgency of treatment?
Question 2 (5 marks)
How do you assess for vascular injury and when do you investigate?
Question 3 (6 marks)
Describe the surgical management of this patient.
Question 4 (5 marks)
What is the role of fasciotomy and what is your technique?
Question 5 (4 marks)
What are the expected outcomes and long-term considerations?
Question 6 (4 marks)
How do you manage the multi-ligament knee injury?
Exam Day Cheat Sheet
Must Mention
- •Knee dislocation vascular injury = 20-40%
- •Hard signs = theatre IMMEDIATELY (no CTA)
- •6-hour warm ischemia window (amputation 50%+ if >8h)
- •Fasciotomies MANDATORY after revascularization
- •External fixator protects vascular repair
- •Common peroneal nerve injury 25-40%
Common Pitfalls
- •CTA with hard signs (delays surgery)
- •No fasciotomies (reperfusion compartment syndrome)
- •Early ligament surgery (wait for soft tissues)
- •Missing peroneal nerve injury
- •No external fixator (vascular repair disruption)
- •ABI >0.9 excludes injury (intimal tear can have normal ABI)