Inflammation then fibrosis of the glenohumeral capsule | Painful global loss of movement | Clinical diagnosis | Loss of passive external rotation is the key sign | Usually self-limiting but slow
- It is a clinical diagnosis: painful, progressive, global restriction of shoulder movement with loss of both active AND passive range - the loss of passive external rotation with the arm by the side is the signature finding
- The pathology is inflammation followed by fibrosis of the glenohumeral capsule, especially the rotator interval and coracohumeral ligament, producing a thickened, contracted, low-volume joint
- Diabetes is the strongest association: diabetic frozen shoulder is more common, often bilateral, more resistant to treatment, and more likely to need a procedure
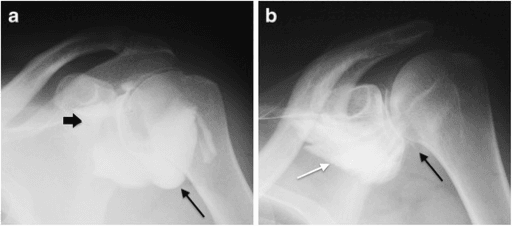
- Imaging is mainly to exclude other causes (osteoarthritis, a locked posterior dislocation, calcific disease): the radiograph is usually normal, and MRI or arthrogram changes are supportive rather than essential
- Most cases are self-limiting but recovery is slow (often 1 to 3 years); first-line care is pain control, an intra-articular steroid injection early, and stretching physiotherapy, with hydrodilatation, manipulation under anaesthesia or capsular release reserved for resistant cases
- “Loss of PASSIVE external rotation with the arm at the side is the discriminating sign - it separates true capsular restriction from a stiff shoulder caused by pain alone or a rotator cuff problem
- “A normal radiograph supports the diagnosis; an abnormal one points you to a secondary cause such as glenohumeral osteoarthritis or a missed posterior dislocation
- “Always check the glucose - new bilateral frozen shoulder can be the presenting sign of undiagnosed diabetes
- “An early intra-articular steroid injection gives the biggest gains in the painful freezing stage; physiotherapy alone works more slowly
Diagnose on the history and examination: painful, progressive, global restriction of shoulder movement with loss of both active and passive range. There is no single test or scan that makes the diagnosis - imaging is mainly to exclude other causes.
Loss of passive external rotation with the arm at the side is the signature sign. A capsular contracture restricts the passive range; pain or a cuff tear alone usually does not block passive external rotation in the same way. This is the most examined discriminator.
Diabetes is the strongest risk factor. Diabetic frozen shoulder is more common, frequently bilateral, more resistant, and more likely to need a procedure. New bilateral disease should prompt a glucose check.
A normal radiograph supports the diagnosis. An abnormal one warns of a secondary cause - glenohumeral osteoarthritis, a locked posterior dislocation (loss of external rotation after a seizure or shock), or calcific disease - that needs different treatment.
Overview
Adhesive capsulitis - the frozen shoulder - is a common, painful condition in which the glenohumeral joint capsule becomes inflamed and then fibrotic, so the shoulder gradually stiffens and loses movement in all directions. It typically affects people aged 40 to 60, is slightly more common in women, and is strongly linked to diabetes.
The hallmark is painful, progressive loss of both active and passive movement, with external rotation usually the first and worst affected. The natural history runs through three overlapping stages - freezing (painful), frozen (stiff), and thawing (recovering) - and most cases eventually settle, although recovery is slow and a minority are left with some lasting stiffness.
For the exam, the recurring themes are: what is happening in the capsule (inflammation then fibrosis), how to recognise it clinically (and separate it from the things it mimics), and how the evidence guides an escalating treatment ladder.
Pathophysiology
The disease process is best understood as inflammation that turns into fibrosis. According to PubMed, current concept reviews describe the pathology of frozen shoulder as capsular inflammation followed by fibrosis and contracture, with the cause of primary (idiopathic) disease still unknown.
Where the disease lives:
- The rotator interval - the triangular space at the front of the joint between the supraspinatus and subscapularis tendons - and the coracohumeral ligament within it are affected early. Contracture here limits external rotation, which is why external rotation is lost first and most severely.
- The anterior and inferior capsule, including the axillary recess, thickens and contracts, reducing the overall joint volume - the small, tight joint seen on an arthrogram.
The cellular story:
- What happens
- Synovial and capsular inflammation with increased inflammatory cytokines and new blood vessel formation
- Result
- Pain (the painful freezing stage), worse at night
- What happens
- Fibroblasts proliferate and transform into contractile myofibroblasts, laying down dense, disorganised collagen
- Result
- A thickened, less elastic capsule
- What happens
- The myofibroblast-rich capsule actively contracts and the rotator interval tightens
- Result
- Loss of movement, especially external rotation - the frozen stage
- What happens
- Over many months the fibrotic tissue slowly remodels and softens
- Result
- Gradual return of movement - the thawing stage
The myofibroblast point is high-yield and explains why a frozen shoulder behaves like other fibrotic, contractile conditions - there is a recognised overlap with Dupuytren disease, which shares the same myofibroblast-driven fibrosis. It also explains why forcing movement against an actively contracting, inflamed capsule early on is unhelpful and painful.
Why Diabetes Predisposes to Frozen Shoulder
Diabetes is the strongest risk factor, and the reason lies in the same collagen biology that drives the capsular contracture. Chronic hyperglycaemia drives non-enzymatic glycation of proteins, producing advanced glycation end-products (AGEs) that accumulate in capsular collagen. These AGEs form abnormal cross-links between collagen fibres, making the capsule stiffer and less compliant, and they also promote fibroblast and myofibroblast activity and a pro-inflammatory state. The result is a capsule more prone to the inflammation-then-fibrosis cascade and more resistant to remodelling.
This explains the clinical pattern of diabetic frozen shoulder: it is more common, often bilateral, more resistant to treatment, slower to recover, and more likely to need a procedure. Risk rises with longer diabetes duration and poorer glycaemic control, and similar glycation and fibrotic biology underlies the association with thyroid disease. It is also why a new bilateral frozen shoulder can be the presenting feature of undiagnosed diabetes, and why a glucose or HbA1c check is part of the work-up.
Advanced glycation end-products from chronic hyperglycaemia cross-link capsular collagen, stiffening the capsule and amplifying the fibrotic response. This mechanistic link explains the more common, bilateral, resistant and incompletely-recovering course of diabetic frozen shoulder, and justifies checking glucose or HbA1c in every new case.
Classification
Two ways of classifying frozen shoulder matter for the exam: by cause (primary versus secondary), and by clinical stage.

Primary (idiopathic) frozen shoulder has no identifiable cause. The international (ISAKOS) terminology reserves the term "frozen shoulder" for this idiopathic stiff shoulder.
Secondary frozen shoulder follows a known cause and is better called a secondary stiff shoulder. Causes include:
- Intrinsic - shoulder pathology such as a rotator cuff tear or calcific tendinitis.
- Extrinsic - a remote cause such as immobilisation after a wrist fracture, stroke, or cardiac/thoracic surgery.
- Systemic - diabetes and thyroid disease, which both predispose to the picture.
The distinction matters because a secondary stiff shoulder needs the underlying cause treated as well, and may behave differently from idiopathic disease.
Clinical Presentation and Examination
History. A patient (often 40 to 60, frequently with diabetes) describes shoulder pain that came on gradually with no major injury, is worse at night and on movement, and is followed by progressive stiffness. Ask specifically about diabetes, thyroid disease, a previous frozen shoulder on the other side, and any period of immobilisation.
Examination - the key is passive movement:
- What you see
- Reduced movement in all directions, active AND passive
- Why it matters
- Distinguishes true capsular restriction from pain-limited movement
- What you see
- With the arm at the side, passive external rotation is markedly reduced
- Why it matters
- The signature sign - a capsular contracture, not just pain or weakness
- What you see
- Power is preserved once pain is accounted for
- Why it matters
- Helps separate it from a large rotator cuff tear
- What you see
- The patient shrugs and uses the scapula to lift the arm
- Why it matters
- Confirms the glenohumeral joint itself is the limited part
The single most useful test is passive external rotation with the arm at the side. If passive external rotation is preserved, think again - pain inhibition or a rotator cuff problem can mimic a frozen shoulder, but they do not usually block passive external rotation the way a contracted capsule does. Lost passive external rotation also raises the spectre of a locked posterior dislocation after a seizure or electric shock, so always look at a radiograph.
Investigations
Frozen shoulder is a clinical diagnosis; investigations are used to exclude other causes and to support the diagnosis, not to make it.
Usually normal in primary disease - this supports the diagnosis. Their main value is to exclude glenohumeral osteoarthritis, a locked posterior dislocation, and calcific deposits. Always get an axillary or modified axillary view so a posterior dislocation is not missed.
Check glucose / HbA1c - undiagnosed diabetes is common - and consider thyroid function. There is no blood test for frozen shoulder itself.
Mainly to look for other pathology (a cuff tear, calcific disease). It can show thickening at the rotator interval and restricted movement but is operator-dependent and not required for diagnosis.
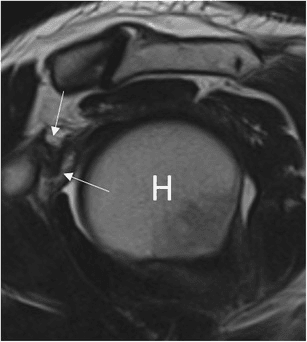
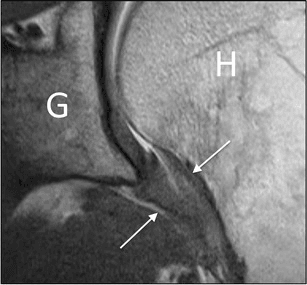
Supportive findings include a thickened coracohumeral ligament and rotator interval, thickened inferior capsule / axillary recess, and on arthrography a reduced joint volume. Reserve MRI for when the diagnosis is unclear or another problem is suspected.
The imaging gallery at the top of this page shows the classic supportive findings: the contracted joint on arthrogram, the thickened coracohumeral ligament, and the thickened axillary pouch.
Differential Diagnosis
Several conditions cause a painful, stiff shoulder, and the examiner rewards a structured differential that uses the passive external rotation sign and a radiograph to separate them. The most important mimic is glenohumeral osteoarthritis, which also restricts passive external rotation but is distinguished by the radiograph; the most dangerous to miss is a locked posterior dislocation.
- Distinguishing feature
- Global loss of active AND passive movement with lost passive external rotation
- Key test
- Clinical diagnosis; radiograph normal
- Distinguishing feature
- Also restricts passive external rotation (closest mimic); older patient, crepitus
- Key test
- Radiograph shows joint-space narrowing, osteophytes, sclerosis
- Distinguishing feature
- Arm fixed in internal rotation, cannot externally rotate past neutral, after seizure or electric shock
- Key test
- Axillary view (and the AP light-bulb sign)
- Distinguishing feature
- Weakness predominates; active loss greater than passive (passive range largely preserved)
- Key test
- Examination and ultrasound or MRI
- Distinguishing feature
- Acute severe pain; motion limited by pain rather than a fixed contracture
- Key test
- Radiograph shows a calcific deposit
- Distinguishing feature
- Painful arc with preserved passive range
- Key test
- Examination and response to subacromial injection
- Distinguishing feature
- Hot, systemically unwell, rapid onset - do not miss
- Key test
- Inflammatory markers and joint aspiration
Glenohumeral osteoarthritis is the condition that most closely mimics a frozen shoulder because it too restricts passive external rotation; the radiograph separates them. A locked posterior dislocation also abolishes external rotation but is easily missed on an AP film, so always obtain an axillary view, especially after a seizure or electric shock.
Management
Treatment is an escalating ladder. The guiding principle is that frozen shoulder is usually self-limiting, so most patients are managed without surgery, with procedures reserved for resistant or severely disabling disease. Match the treatment to the stage: injection helps most in the painful freezing stage; stretching, hydrodilatation, and release target the stiff frozen stage.
- Education and reassurance - explain the natural history and the long but generally favourable course. This alone changes expectations and reduces distress.
- Analgesia and NSAIDs - for pain control, particularly in the painful freezing stage.
- Intra-articular corticosteroid injection - most effective early, when pain dominates. It gives faster pain relief and earlier improvement than physiotherapy alone, although the long-term difference narrows.
- Physiotherapy - gentle, progressive stretching within a comfortable range. Forced, aggressive stretching of an inflamed capsule is counterproductive early on.
This combination - an early injection plus structured physiotherapy - is the backbone of treatment and is what most patients need.
Aggressive stretching or manipulation during the painful inflammatory (freezing) stage worsens pain and can provoke more fibrosis. Manipulation under anaesthesia in osteoporotic or diabetic patients carries a real risk of humeral fracture, dislocation, and cuff injury. Time the intervention to the stage, and choose a controlled release over a forceful manipulation when the bone or capsule is at risk.
Surgical Technique - Arthroscopic Capsular Release
The aim is a controlled, complete release of the contracted capsule, replacing the uncontrolled tearing of a manipulation. Release the diseased tissue, restore range on the table, then protect the result with early, structured physiotherapy so the capsule does not simply re-scar.
Complications
Complications arise both from the disease and from its treatment.
- Who and when
- A minority, especially diabetics
- What to do
- Escalate the treatment ladder; counsel on the long course
- Who and when
- Diabetics and prior frozen shoulder
- What to do
- Warn the patient; treat the other shoulder on its merits
- Who and when
- Manipulation under anaesthesia in osteoporotic or diabetic bone
- What to do
- Prefer a controlled release; manipulate gently or avoid in fragile bone
- Who and when
- During forceful manipulation
- What to do
- Controlled technique; recognise and treat the injury
- Who and when
- During inferior capsular release
- What to do
- Stay close to the capsule and protect the nerve inferiorly
- Who and when
- After injection, especially in diabetics
- What to do
- Warn diabetics about a transient rise in blood glucose; strict asepsis
Rehabilitation and Recovery
Rehabilitation is central, not an afterthought - both as primary treatment and after any procedure.
- Primary physiotherapy uses gentle, progressive stretching within a comfortable range, matched to the stage. Early on, the goal is to maintain range without provoking the inflamed capsule; later, the goal is to regain range as the capsule remodels.
- After manipulation or release, start immediate, intensive, supervised physiotherapy to hold the gains - the result is lost if the capsule re-scars.
- Home exercise between sessions is essential; a frozen shoulder is treated mostly by the patient at home.
- Expectations: most regain good, functional movement, but recovery is slow (often many months to a few years), and a minority keep some residual stiffness.
Outcomes and Prognosis
The overall prognosis is good but slow. Most patients improve substantially, whether treated conservatively or with a procedure, and the headline message of the best randomised evidence is that the different treatments end up close to each other by a year.
- Natural history: primary frozen shoulder is usually self-limiting, but recovery commonly takes 1 to 3 years, and a minority are left with some lasting restriction that is often well tolerated.
- Diabetes worsens the outlook: diabetic frozen shoulder is more resistant, more often bilateral, and more likely to need a procedure and to recover incompletely.
- Treatments converge: in secondary care, manipulation, capsular release, and structured physiotherapy with steroid injection all produced similar shoulder scores at 12 months, so the choice rests on risk and cost as much as on outcome.
Clinical Relevance
Frozen shoulder is one of the commonest shoulder complaints in clinic and a favourite exam topic because it tests clinical reasoning rather than fancy imaging. The examiner wants to see that you can diagnose it clinically (global loss of movement, lost passive external rotation), exclude the mimics (osteoarthritis, locked posterior dislocation, cuff tear) with a sensible history, examination and radiograph, recognise the diabetes link and check a glucose, and apply an evidence-based escalating ladder of treatment - reassurance and injection first, surgery last and only for resistant disease. Getting the passive external rotation sign and the escalation logic right is what separates a safe answer from a weak one.
Exam Points
Loss of passive external rotation with the arm at the side is the key examination finding and the most tested discriminator.
No scan makes the diagnosis. Radiographs are usually normal and are taken to exclude osteoarthritis and a locked posterior dislocation.
The strongest risk factor; diabetic disease is often bilateral, more resistant, and more likely to need surgery. Check a glucose.
UK FROST: manipulation, capsular release, and physiotherapy with injection give similar one-year scores - choose by risk and cost.
Injection helps most in the painful freezing stage; stretching, hydrodilatation and release target the stiff frozen stage.
Manipulation in osteoporotic or diabetic bone risks humeral fracture - prefer a controlled arthroscopic release.
Guidelines, Registries and Global Practice
- Diagnosis is consistently clinical. Systematic reviews of clinical practice guidelines for shoulder disorders agree that the initial assessment rests on history and examination, that MRI is usually not needed early, and that radiographs are used mainly to exclude other causes. The international (ISAKOS) terminology distinguishes primary frozen shoulder (idiopathic) from a secondary stiff shoulder (known cause).
- Conservative care first, side by side. Guidance from bodies such as the AAOS (US), BOA/BESS (UK), and equivalent European groups converges on the same ladder: education, analgesia, an early intra-articular steroid injection, and stretching physiotherapy, with hydrodilatation, manipulation, and arthroscopic capsular release reserved for resistant disease.
- Where guidance differs is mainly the threshold and timing for escalating to a procedure and the relative emphasis on hydrodilatation versus manipulation versus release - reflecting local resources and expertise rather than disagreement about the underlying disease.
- Best randomised evidence (UK FROST) shows the secondary-care options converge by one year, so many systems favour the least invasive, most cost-effective route, with surgery reserved for selected patients - especially the more resistant diabetic shoulder.
- Global practice variation largely reflects access (availability of image-guided injection, theatre time, and arthroscopy) rather than differences in the principles of stage-matched, escalating care.
Memory aids
DIABETESRisk Factors for Frozen Shoulder
Hook:The risks spell DIABETES - fitting, because diabetes is the single most important risk factor for a frozen shoulder.
FFTThe Three Stages
Hook:Freeze, Frozen, Thaw - FFT. Pain leads, stiffness follows, then slow recovery: the natural history of a frozen shoulder.
PAINSEscalating Treatment Ladder
Hook:Treat the PAINS in order - start simple (relief, injection, physio) and escalate to hydrodilatation then surgery only when needed.
At a Glance
The exam essentials are simple to state: frozen shoulder is a clinical diagnosis, the key sign is loss of passive external rotation, the strongest risk factor is diabetes, imaging is mainly to exclude other causes, and treatment escalates from pain control and an early injection through physiotherapy and hydrodilatation to surgical release only for resistant disease.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old woman presents with several months of right shoulder pain, worse at night, and increasing stiffness, with no injury. How would you assess her and what is your diagnosis?”
“A 58-year-old man with type 2 diabetes has a frozen shoulder that has not improved despite an injection and three months of physiotherapy. He still has severe stiffness and disability. How do you proceed?”
Diagnosis
- Clinical diagnosis - painful, progressive, GLOBAL loss of movement
- Loss of both active AND passive range
- Loss of passive external rotation with arm at side - the signature sign
- Radiograph usually normal; taken to exclude other causes
Pathology and Risk
- Capsular inflammation then fibrosis and contracture
- Rotator interval and coracohumeral ligament hit first (external rotation lost first)
- Myofibroblast-driven contracture - overlap with Dupuytren disease
- Diabetes is the strongest risk factor - often bilateral and resistant
Treatment Ladder
- Education, analgesia/NSAIDs, reassurance (usually self-limiting)
- Early intra-articular steroid injection in the painful freezing stage
- Gentle stretching physiotherapy; hydrodilatation if resistant
- Manipulation under anaesthesia or arthroscopic capsular release for refractory disease
Red Flags and Pitfalls
- Preserved passive external rotation - reconsider the diagnosis
- Lost external rotation after seizure/shock - exclude locked posterior dislocation (axillary view)
- Manipulation in osteoporotic/diabetic bone risks humeral fracture
- UK FROST: treatments converge at 1 year - choose by risk and cost; physiotherapy mandatory after any procedure
Evidence Base
According to PubMed, the following studies underpin the modern management of frozen shoulder.
Surgery versus Physiotherapy plus Steroid for Frozen Shoulder (UK FROST RCT)
- Multicentre, pragmatic, three-arm RCT of 503 adults with primary frozen shoulder across 35 UK hospitals
- Manipulation under anaesthesia versus arthroscopic capsular release versus early structured physiotherapy plus steroid injection
- Oxford Shoulder Scores at 12 months were similar across all three groups; no treatment was clinically superior
- Arthroscopic capsular release carried more serious adverse events; manipulation under anaesthesia was the most cost-effective option
Manual Therapy and Exercise for Adhesive Capsulitis (Cochrane Review)
- Systematic review of 32 randomised trials (1836 participants)
- Combined manual therapy and exercise for six weeks probably gives LESS short-term improvement than a glucocorticoid injection (pain difference about 26 points on a 100-point scale at seven weeks)
- Differences between manual therapy/exercise and injection were not clinically important by six and twelve months
- After arthrographic distension, manual therapy and exercise gave greater patient-reported success and active abduction at six weeks
Shoulder Stiffness - Current Concepts and Terminology (ISAKOS Review)
- International consensus reserving 'frozen shoulder' for the idiopathic stiff shoulder and 'secondary stiff shoulder' for a known cause
- Describes the pathophysiology as capsular fibrosis and inflammation with chondrogenesis, cause still unknown
- Conservative treatment (pain control, injection with or without distension, physiotherapy) is first-line
- For refractory stiffness, arthroscopic capsular release is preferred over manipulation because of the lower risk of manipulation-related complications
Hydrodilatation and Bursal Steroid plus Physiotherapy versus Physiotherapy Alone (RCT)
- Single-blind RCT of 70 patients with freezing-stage frozen shoulder
- Hydrodilatation plus subdeltoid bursal steroid, mobilisation and physiotherapy versus usual-care physiotherapy alone
- The combination group had significantly better pain, disability (SPADI), range of motion and self-assessment scores
- Benefits were significant and persisted at one, two, four and six months