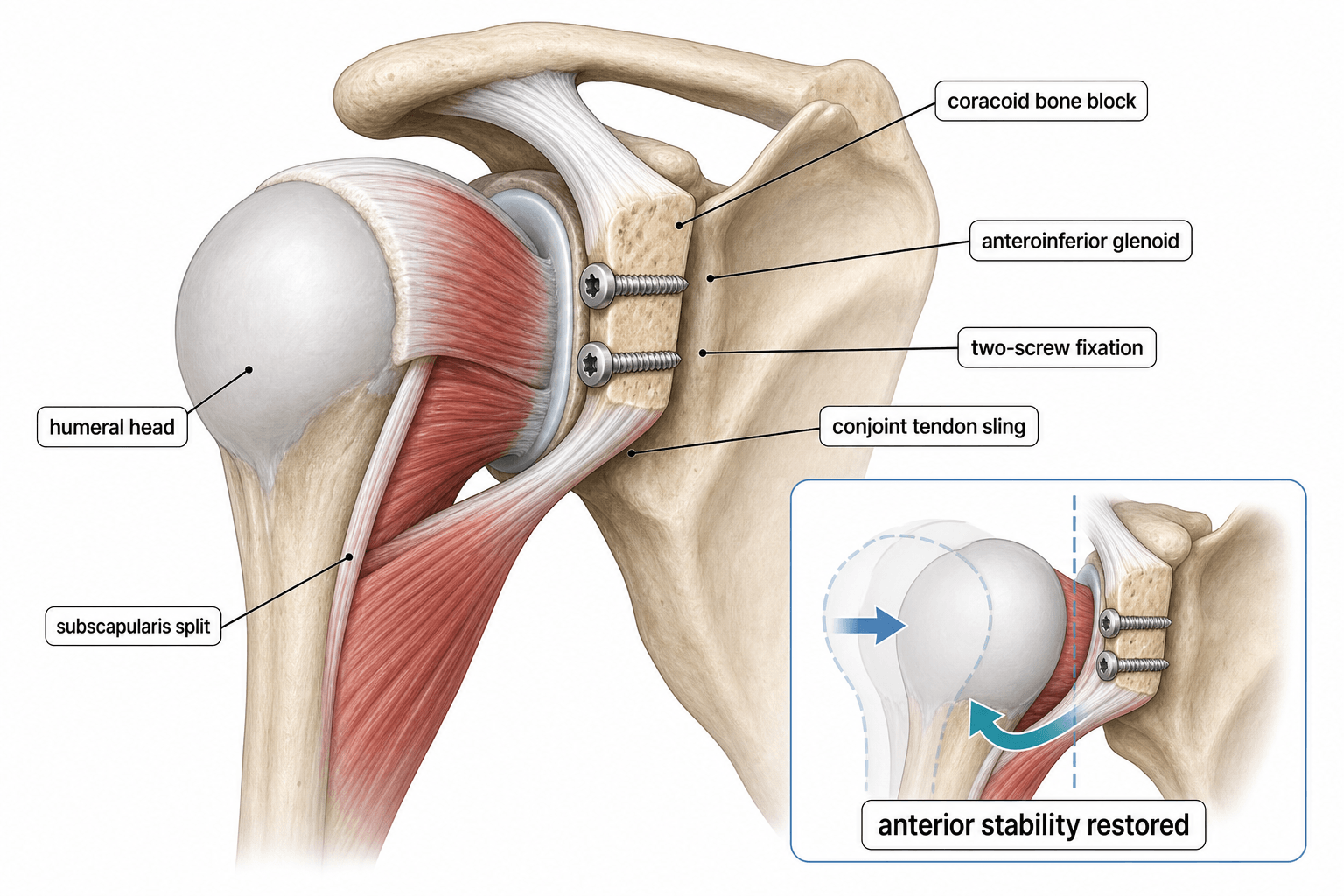
Coracoid Transfer | Anterior Instability | Glenoid Bone Loss
- Coracoid transfer creates a triple blocking effect: bone block, sling effect, and capsular repair
- Indicated when glenoid bone loss is greater than 25 percent (inverted pear) or off-track Hill-Sachs
- Latarjet uses two screws to fix coracoid flush on anterior glenoid neck in the decubitus position
- Complications: nerve injury (axillary, musculocutaneous), hardware issues, graft nonunion, recurrent instability
- Bristow-Latarjet is the gold standard for recurrent anterior instability with significant bone loss
- “Inverted pear glenoid = greater than 25 percent bone loss = operative (Latarjet)
- “Triple effect: bone block + conjoint tendon sling + inferior capsular shift
- “Musculocutaneous nerve lies 5-8 cm distal to coracoid tip — blunt dissection only
- “Recurrent dislocation after soft tissue repair alone + bone loss = Latarjet indication
Glenoid bone loss greater than 25 percent (inverted pear glenoid), off-track Hill-Sachs lesion, failed arthroscopic Bankart repair, contact or collision athletes with bone loss, revision instability surgery.
Voluntary dislocators, active infection, severe glenohumeral arthritis, inadequate coracoid bone stock (elderly osteopenic patients), uncontrolled seizure disorder.
Coracoid process gives attachment to conjoint tendon (short head of biceps + coracobrachialis), pectoralis minor, and coracoacromial (CA) ligament. Transfer preserves conjoint tendon attachment, creating a dynamic sling across the anteroinferior glenoid.
Bristow transfers only the coracoid tip attached via the CA ligament, fixed with one screw. Latarjet transfers the entire coracoid process flat on the anterior glenoid neck, fixed with two screws, providing a larger bone block and greater surface area for healing.
- Classic Bristow
- Tip only (coracoid tip with CA ligament)
- Latarjet (Original)
- Full coracoid process laid flat
- Congruent Arc Modification
- Full coracoid rotated 90 degrees
- Classic Bristow
- Single screw
- Latarjet (Original)
- Two screws (parallel)
- Congruent Arc Modification
- Two screws
- Classic Bristow
- Small — cancellous surface only
- Latarjet (Original)
- Larger flat surface, flush on glenoid
- Congruent Arc Modification
- Matches glenoid curvature — maximum congruence
- Classic Bristow
- Attached via CA ligament, hangs as a sling
- Latarjet (Original)
- Flush on anterior glenoid rim (lying flat)
- Congruent Arc Modification
- Rotated so inferior surface faces glenoid
- Classic Bristow
- Historical — largely abandoned
- Latarjet (Original)
- Gold standard for bone loss
- Congruent Arc Modification
- Gaining favour for improved congruence
BSSLatarjet Triple Blocking Effect
Hook:BSS = Bone block + Sling + Soft tissue — the triple effect that makes Latarjet work when Bankart fails!
CORACOIDLatarjet Key Steps
Hook:Remember CORACOID for every step — omit nothing and the graft heals perfectly!
Overview and Epidemiology
The Bristow-Latarjet procedure is the most important surgical option for anterior shoulder instability with bone loss. The classic Bristow was first described by Helfet in 1958, modifying Latarjet's 1954 original technique. The modern Latarjet has become the gold standard for glenoid bone loss exceeding 25 percent because it addresses bone deficiency, creates a dynamic soft tissue sling, and restores the labral bumper. Understanding the differences between Bristow and Latarjet, the indications for coracoid transfer versus arthroscopic soft tissue repair, and the specific complications is essential for fellowship exams.
- Anterior shoulder dislocation is the most common large joint dislocation
- Recurrent instability develops in 50-90 percent of young athletes after first dislocation
- Glenoid bone loss present in up to 70 percent of recurrent dislocators
- Greater than 25 percent bone loss (inverted pear) occurs in approximately 20 percent of recurrent dislocators
- Latarjet (1954): Original description of coracoid transfer to anterior glenoid
- Bristow (1958): Modified technique — coracoid tip with CA ligament, single screw
- Patte (2000s): Revived Latarjet with biomechanical rationale (triple blocking effect)
- Modern era: All-arthroscopic Latarjet developed; congruent arc modification described
Pathophysiology
Anterior glenoid bone loss creates a bony deficiency that cannot be overcome by soft tissue repair alone. When the anteroinferior glenoid rim is deficient, the labrum and capsule have no stable anchor point, and the humeral head can translate over the deficient rim even after Bankart repair. The critical threshold is greater than 25 percent of the glenoid diameter lost (the "inverted pear" glenoid), below which arthroscopic Bankart repair has acceptable results, and above which coracoid transfer is indicated. An off-track Hill-Sachs lesion (engaging lesion that crosses the glenoid track) is an additional indication even with lesser degrees of glenoid bone loss.
- Normal
- Intact labral bumper, deep concavity
- With Bone Loss
- Flattened, deficient anteroinferior rim
- After Latarjet
- Restored by coracoid graft
- Normal
- Centred within glenoid fossa
- With Bone Loss
- Translates anteriorly over deficient rim
- After Latarjet
- Graft blocks translation, sling reinforces
- Normal
- Negative intra-articular pressure maintained
- With Bone Loss
- Lost with rim fracture/attrition
- After Latarjet
- Restored via capsular repair to CA ligament
- Normal
- Balanced rotator cuff and capsuloligamentous structures
- With Bone Loss
- Deficient AIGHL and labrum
- After Latarjet
- Conjoint tendon sling provides dynamic restraint in abduction-external rotation
Glenoid track = the contact area of the humeral head on the glenoid through the arc of motion. The track width equals approximately 84 percent of the glenoid width.
On-track Hill-Sachs: lesion remains within the glenoid track — does not engage
Off-track Hill-Sachs: lesion width plus bone defect exceeds glenoid track — engages and dislocates
Clinical implication: Off-track lesions need bony procedures (Latarjet or remplissage + Bankart)
Normal glenoid: Wider inferiorly than superiorly (pear-shaped)
Greater than 25 percent bone loss: Superior width now equals or exceeds inferior width (inverted pear)
Diagnostic methods: Three-dimensional CT with Bernageau view, best circle fit method on AP or axillary radiograph, MRI with sagittal oblique reconstructions
Key point: The inverted pear sign on imaging is a reliable indicator that arthroscopic Bankart repair alone will have unacceptably high failure rates
Classification and Types
Classification of Glenoid Bone Loss
- Glenoid Morphology
- Normal pear shape
- Recommended Treatment
- Arthroscopic Bankart repair
- Rationale
- Soft tissue repair sufficient, low recurrence
- Glenoid Morphology
- Borderline — still pear-shaped
- Recommended Treatment
- Bankart + remplissage or Latarjet (debated)
- Rationale
- Consider patient factors: sport, contact, Hill-Sachs
- Glenoid Morphology
- Inverted pear
- Recommended Treatment
- Latarjet (gold standard)
- Rationale
- Bony reconstruction required; Bankart failure rate exceeds 30 percent
- Glenoid Morphology
- Severe deficiency
- Recommended Treatment
- Iliac crest bone graft (Eden-Hybinette) or distal tibial allograft
- Rationale
- Coracoid graft may be insufficient for massive defects
The 25 percent threshold is the most commonly cited critical value, though some authors argue for earlier intervention at 15-20 percent in high-risk patients.
Clinical Assessment
- Instability episodes: Number, mechanism, first vs recurrent
- Prior surgery: Details of any previous Bankart repair or stabilisation
- Functional demands: Contact sport, overhead athlete, manual labourer
- Neurological symptoms: Numbness or weakness after dislocation episodes
- Apprehension test: Positive in anterior instability in abduction-external rotation
- Relocation test: Relief of apprehension with posteriorly directed force
- Load and shift: Assess anterior and posterior translation (graded 0-3)
- Generalised ligamentous laxity: Beighton score — hypermobile patients need different approach
- Rotator cuff assessment: Exclude concomitant cuff pathology
Before planning a Latarjet, you must:
- Quantify glenoid bone loss: 3D CT scan with Bernageau or en-face view — use the best-fit circle method to measure defect as a percentage of glenoid diameter
- Assess Hill-Sachs lesion: Size, depth, and location on MRI or CT — determine on-track vs off-track
- Evaluate coracoid size and bone quality: Especially important in older patients with osteopenia — a small or osteoporotic coracoid may not provide adequate graft
- Document neurovascular status: Axillary and musculocutaneous nerve function pre-operatively — establishes baseline for post-operative comparison
- Arthroscopic Bankart
- Less than 15 percent (no inverted pear)
- Latarjet (Coracoid Transfer)
- Greater than 25 percent (inverted pear)
- Arthroscopic Bankart
- Non-engaging or small
- Latarjet (Coracoid Transfer)
- Off-track / engaging with bone loss
- Arthroscopic Bankart
- Primary repair
- Latarjet (Coracoid Transfer)
- Revision after failed Bankart
- Arthroscopic Bankart
- Low-demand, non-contact
- Latarjet (Coracoid Transfer)
- Contact/collision athlete, high demand
- Arthroscopic Bankart
- 5-15 percent
- Latarjet (Coracoid Transfer)
- 1-5 percent
Investigations

Imaging Protocol
Views: True AP, axillary, Stryker notch, Bernageau (if available)
Look for: Hill-Sachs lesion (Stryker notch), glenoid rim fracture or erosion (axillary), hardware from prior surgery
Limitation: Underestimates glenoid bone loss compared to CT
Indication: Mandatory for any patient being considered for Latarjet
Technique: Thin-slice CT with 3D reconstruction, en-face glenoid view (sagittal oblique)
Measurement: Best-fit circle on inferior glenoid — defect width divided by circle diameter gives percentage bone loss
Key finding: Inverted pear (superior width greater than or equal to inferior width) confirms greater than 25 percent loss
Indication: Assess labrum, capsule, rotator cuff, and articular cartilage
Findings: Bankart lesion, labral tears, HAGL, capsular volume, Hill-Sachs dimensions
Utility: Surgical planning for concomitant pathology; combined with CT for comprehensive assessment
The best-fit circle method on a sagittal oblique CT reconstruction is the standard technique for measuring glenoid bone loss. A circle is drawn to fit the inferior glenoid rim (which is typically intact in anterior bone loss). The missing anterior bone is measured as a percentage of the circle diameter. The inverted pear sign is a reliable qualitative indicator that bone loss exceeds 25 percent.
Management and Surgical Technique
Open Latarjet: Step-by-Step
Positioning: Beach chair or lateral decubitus. Arm free-draped for full ROM assessment.
Surgical Steps
Approach: Standard deltopectoral interval. Identify cephalic vein (retract laterally with deltoid). Expose coracoid from tip to base.
Key landmark: Coracoclavicular ligaments (trapezoid and conoid) — osteotomy must be distal to these.
Caution: Identify the axillary nerve inferiorly and musculocutaneous nerve medially (lies 5-8 cm distal to coracoid tip penetrating coracobrachialis).
Detach pectoralis minor: Sharp release from medial coracoid. Preserve conjoint tendon attachment laterally.
Release CA ligament: Sharply from lateral coracoid, maintaining a stump for later capsular repair.
Osteotomy: Using an oscillating saw or osteotome, cut the coracoid at its base, just distal to the coracoclavicular ligaments. This yields a graft approximately 2.5-3 cm in length.
Prepare graft: Decorticate the medial (deep) surface to expose cancellous bone. Drill two parallel holes for screw fixation.
Expose anterior glenoid: Retract subscapularis (split or tenotomy depending on surgeon preference). Identify the glenoid rim and neck.
Decorticate: Freshen the anterior glenoid neck to bleeding cancellous bone using a burr or curette.
Position: The graft should sit flush with the anteroinferior glenoid rim, extending from approximately the 2 to 5 o'clock position (right shoulder). The graft must not overhang into the joint.
Screws: Two parallel cortical screws (typically 3.5 or 4.0 mm malleolar screws) aimed posteriorly and slightly superiorly. Bicortical fixation is ideal — palpate the posterior glenoid neck to confirm screw penetration without prominent tips.
Check position: Intra-operative fluoroscopy to confirm graft position, screw length, and absence of step-off.
Capsular repair: Suture the capsule and remaining CA ligament to the lateral aspect of the graft, recreating the labral bumper.
Subscapularis repair: If split was used, repair the upper and lower portions. If tenotomy, repair with strong sutures through bone tunnels or anchors.
Deltopectoral interval: Loose closure to prevent adhesions.
Immobilisation: Sling in internal rotation for 4-6 weeks.
The most common technical error is medial placement of the graft — it should be flush with the glenoid rim, not medial on the neck. A medially placed graft does not restore the articular arc and may lead to persistent instability. An overly lateral graft that overhangs into the joint causes early osteoarthritis. The goal is flush to the rim.
A key examinable technical decision the steps above mention only in passing is how to handle the subscapularis to reach the glenoid:
- Subscapularis split (preferred): a horizontal split is made between the upper two-thirds and lower one-third of the subscapularis tendon (the relatively avascular junction), and the coracoid graft is passed through the split. This preserves the subscapularis attachment and function and is the modern standard - the conjoint-tendon sling then acts precisely at the position of apprehension (abduction-external rotation) as the lower subscapularis tensions.
- Subscapularis tenotomy (L-shaped/complete): gives wider exposure of the glenoid but requires repair and risks subscapularis insufficiency, fatty infiltration and weakness - a postoperative positive belly-press or lift-off test, and potential loss of internal-rotation power.
- Why the split matters for the sling: the dynamic sling effect of the Latarjet depends on the conjoint tendon passing through the lower subscapularis; the split positions the sling correctly to reinforce the inferior capsule in ABER.
Exam point: prefer a subscapularis split at the upper-two-thirds/lower-one-third junction (preserves function and positions the conjoint sling correctly); a complete tenotomy gives exposure but risks subscapularis insufficiency and fatty infiltration.
Complications
- Incidence
- 5-15 percent
- Risk Factors
- Poor fixation, medial placement, smoking, osteopenia
- Management
- Most asymptomatic; revise if unstable
- Incidence
- Up to 30 percent partial at 1 year
- Risk Factors
- Screw prominence, biological factors
- Management
- Monitor with CT; revise if instability recurs
- Incidence
- 2-10 percent
- Risk Factors
- Small graft, screw holes weakening, early mobilisation
- Management
- Hardware removal if symptomatic; revision graft if unstable
- Incidence
- 1-5 percent
- Risk Factors
- Medial graft placement, resorption, off-track Hill-Sachs
- Management
- CT to assess graft; revision with iliac crest graft if needed
- Incidence
- 1-8 percent (mostly neuropraxia)
- Risk Factors
- Retraction, drilling, screw placement
- Management
- Most resolve within 3-6 months; EMG if persistent
- Incidence
- 5-15 percent
- Risk Factors
- Prominent screw heads, thin soft tissue coverage
- Management
- Remove screws after graft union (typically 6 months)
- Incidence
- 5-10 percent
- Risk Factors
- Prolonged immobilisation, subscapularis over-tightening
- Management
- Physiotherapy; manipulation under anaesthesia if persistent beyond 6 months
- Incidence
- 20-30 percent at long-term follow-up
- Risk Factors
- Graft overhang, malrotation, residual instability
- Management
- Treat OA according to severity; may need arthroplasty
Axillary nerve injury can occur during retraction of the inferior capsule or from drill/screw penetration through the posterior glenoid neck. Musculocutaneous nerve injury occurs during medial retraction of the conjoint tendon or coracobrachialis. The musculocutaneous nerve enters the coracobrachialis 5-8 cm distal to the coracoid tip. Both injuries are usually neuropraxias that resolve, but permanent injury is catastrophic. Always stay lateral to the conjoint tendon during dissection and use blunt retraction only.
GRAFTComplications to Cite in the Viva
Hook:Cite GRAFT complications to show the examiner you know the downsides, not just the indications!
Outcomes and Prognosis
- Short-term (Under 2 years)
- 1-3 percent
- Mid-term (2-5 years)
- 2-5 percent
- Long-term (Over 10 years)
- 5-8 percent
- Short-term (Under 2 years)
- 80-90 percent
- Mid-term (2-5 years)
- 75-85 percent
- Long-term (Over 10 years)
- Contact sport return approximately 70-80 percent
- Short-term (Under 2 years)
- 85-95 percent
- Mid-term (2-5 years)
- Stable after union
- Long-term (Over 10 years)
- Late resorption possible in some
- Short-term (Under 2 years)
- Significant improvement
- Mid-term (2-5 years)
- Maintained improvement
- Long-term (Over 10 years)
- Slight decline with OA changes
- Short-term (Under 2 years)
- Minimal new changes
- Mid-term (2-5 years)
- Mild changes in 10-20 percent
- Long-term (Over 10 years)
- Moderate-severe in 20-30 percent
Best prognosis: Young patient, primary bony procedure (not revision), contact athlete motivated for rehabilitation, good bone quality, graft positioned flush with rim
Poor prognosis: Revision surgery after multiple prior procedures, poor bone quality (osteopenic coracoid), medial graft malposition, post-operative stiffness, voluntary dislocator
Key point: The Latarjet achieves the lowest recurrence rate of any instability procedure in the setting of bone loss, but the trade-off is a higher complication rate than arthroscopic soft tissue repair.
Guidelines, Registries and Global Practice
- Anterior shoulder dislocation is the commonest joint dislocation, with incidence peaking in males aged 20-30 years
- Recurrent instability rates vary: up to 90 percent in young male contact athletes, less than 20 percent in older low-demand patients
- Glenoid bone loss is present in the majority of recurrent dislocators undergoing surgical stabilisation
- Latarjet is the most performed bony procedure worldwide for instability with bone loss
- High-resource settings: CT-based 3D planning, patient-specific instrumentation, arthroscopic Latarjet in specialist centres
- Limited-resource settings: Open Latarjet with intra-operative fluoroscopy remains the standard; CT may not be available for pre-operative planning
- Universal principle: Graft position (flush with rim) and adequate fixation (two bicortical screws) are non-negotiable regardless of setting
- Rehabilitation protocols vary globally but the principle of protected immobilisation followed by progressive ROM is universal
- Indications Emphasis
- Greater than 25 percent bone loss or off-track Hill-Sachs; failed Bankart
- Technique Preference
- Open or arthroscopic Latarjet at surgeon discretion
- Key Recommendation
- CT mandatory before any bony procedure; report bone loss as percentage
- Indications Emphasis
- Bone loss assessment essential; Latarjet for inverted pear
- Technique Preference
- Open Latarjet preferred; arthroscopic in experienced centres
- Key Recommendation
- Multi-disciplinary discussion for borderline cases; shared decision-making
- Indications Emphasis
- Risk stratification based on bone loss, sport, and prior surgery
- Technique Preference
- Both open and arthroscopic Latarjet acceptable; remplissage considered for moderate bone loss
- Key Recommendation
- Discussion of OA risk and return-to-sport timeline essential for informed consent
- Indications Emphasis
- Principles of graft fixation: compression, stability, congruent position
- Technique Preference
- Technique focuses on precise graft positioning and bicortical fixation
- Key Recommendation
- Emphasise anatomical reduction of the graft flush with glenoid rim
There is no dedicated global registry specifically tracking Latarjet outcomes, though some national shoulder registries (Danish, Norwegian) capture instability procedures. The evidence base includes one landmark randomised trial (Bessiere et al.) plus multiple large case series and meta-analyses. The Walch-Lyon school in France holds the largest single-surgeon series with long-term follow-up. Current guidelines are consensus-based, drawing from Level 2-4 evidence.
Record in every Latarjet:
- Pre-operative bone loss measurement (percentage on CT) and Hill-Sachs classification (on-track vs off-track)
- Graft size and fixation method (screw diameter, bicortical confirmation)
- Intra-operative fluoroscopy confirming graft position flush with rim
- Any concern for nerve irritation or injury during the case
- Post-operative rehabilitation plan and return-to-sport timeline
A poorly positioned graft that requires revision is a major source of medicolegal claims. Document graft position with intra-operative imaging and clearly communicate rehabilitation restrictions.
Controversies and Areas of Uncertainty
No high-quality randomised trial has definitively shown superiority of one approach over the other. Arthroscopic Latarjet offers better visualisation and cosmesis but has a steep learning curve. Open Latarjet has longer track record and more outcome data. Current consensus: either approach is acceptable if performed by an experienced surgeon.
The management of borderline bone loss remains debated. Some advocate Latarjet for all contact athletes regardless of bone loss percentage, while others reserve it for confirmed inverted pear glenoids. The SMOOTH trial and similar studies are attempting to clarify this grey zone.
Arthroscopic remplissage (posterior capsulotenodesis to the Hill-Sachs defect) combined with Bankart repair may be an alternative to Latarjet in moderate bone loss. However, it does not address glenoid deficiency and may cause loss of external rotation. Its role is best defined for on-track Hill-Sachs with minimal glenoid bone loss.
Partial graft resorption is common on CT but its clinical significance is debated. Some studies show no correlation between partial resorption and instability recurrence, while others suggest it predisposes to failure. Complete resorption is rare but catastrophic.
The classic Latarjet fixes the coracoid with two cortical screws, but a modern alternative is cortical suture-button (EndoButton-type) fixation - worth knowing as it directly targets the screw-related complications:
- The screw construct: two parallel bicortical screws give strong compression and is the long-track-record standard, but screws cause many of the procedure's specific complications - graft fracture through the screw holes, hardware irritation/prominence, intra-articular or posterior screw penetration, and nerve injury from the drill/screw trajectory near the suprascapular/axillary nerves.
- The suture-button (Boileau guided-Latarjet) construct: the graft is held against the glenoid by a double cortical-button/suture loop passed through bone tunnels (no metal across the graft). It avoids screw-related graft fracture and hardware prominence and is favoured in the arthroscopic guided Latarjet.
- The trade-offs: button fixation provides less rigid compression at the graft-glenoid interface (relying more on the suture-loop and bone apposition), so concerns include graft positioning/healing and a different complication profile; comparative data show broadly similar union/recurrence with fewer hardware complications.
- The constant: whatever the fixation, the graft must sit flush with the rim and the construct must be stable enough for early protected motion.
Exam point: screws (two bicortical) are the standard but cause graft-fracture/hardware/nerve complications; suture-button fixation (the guided arthroscopic Latarjet) avoids metal across the graft at the cost of less rigid compression - both depend on a flush, well-positioned graft.
MCQ Practice Points
Q: What is the critical threshold of glenoid bone loss above which arthroscopic Bankart repair alone is contraindicated? A: Greater than 25 percent of the glenoid diameter (inverted pear glenoid). Below this, arthroscopic soft tissue repair has acceptable recurrence rates. Above this, bony augmentation (Latarjet) is the gold standard because the labrum and capsule have no stable rim to anchor to.
Q: What is the triple blocking effect of the Latarjet procedure? A: Bone block (coracoid graft replaces the deficient anteroinferior glenoid rim), sling effect (the conjoint tendon creates a dynamic sling that reinforces the anteroinferior capsule in abduction-external rotation), and capsular repair (the CA ligament remnant is used to reattach the capsule, restoring the labral bumper). This triple mechanism explains why Latarjet succeeds where Bankart fails in bone loss.
Q: Which nerve is at greatest risk during the Latarjet procedure and how do you protect it? A: The musculocutaneous nerve is at greatest risk. It enters the coracobrachialis muscle 5-8 cm distal to the coracoid tip. Protection requires: staying lateral to the conjoint tendon during dissection, using blunt retraction only (no sharp retractors medially), and avoiding excessive medial retraction of the coracobrachialis. The axillary nerve is also at risk during inferior capsular exposure and drill/screw penetration through the posterior glenoid neck.
Q: What is the most common technical error during the Latarjet procedure? A: Medial placement of the coracoid graft. The graft should be positioned flush with the glenoid rim (not medial on the glenoid neck). A medially placed graft does not restore the articular arc and fails to prevent anterior humeral head translation. Overly lateral placement (overhanging into the joint) causes early osteoarthritis.
Q: What is the incidence and significance of graft osteolysis after Latarjet? A: Partial graft resorption is common (up to 30 percent at 1 year on CT) but its clinical significance is debated. Most partial resorption does not cause recurrent instability. Complete graft resorption is rare but catastrophic, requiring revision with an alternative graft source (iliac crest bone graft or distal tibial allograft).
Q: When is an Eden-Hybinette iliac crest bone graft preferred over a Latarjet? A: When glenoid bone loss exceeds 35-40 percent, when the coracoid is insufficient (small, osteoporotic, or previously harvested), or in revision after a failed Latarjet with complete graft resorption. The iliac crest provides a larger bone block but does not include the dynamic sling effect of the conjoint tendon.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old rugby player has sustained 5 anterior dislocations of his dominant right shoulder over 3 years. He had an arthroscopic Bankart repair 2 years ago but redislocated 6 months post-operatively during a tackle. A CT scan shows 30 percent anteroinferior glenoid bone loss with an inverted pear glenoid. There is an engaging Hill-Sachs lesion. What is your management?”
“A 30-year-old contact athlete underwent an open Latarjet procedure 8 weeks ago for recurrent anterior instability with 28 percent glenoid bone loss. At routine follow-up, he reports persistent tingling over the lateral forearm and weakness of elbow flexion. A CT scan shows the coracoid graft is positioned 5 mm medial to the glenoid rim with early signs of resorption at the superior screw. How do you manage this?”
Indications
- Glenoid bone loss greater than 25 percent (inverted pear on CT)
- Off-track (engaging) Hill-Sachs lesion
- Failed arthroscopic Bankart repair with bone loss
- Contact or collision athletes with recurrent instability and bone deficiency
- Revision anterior stabilisation surgery
Triple Blocking Effect
- Bone block: coracoid graft replaces deficient anteroinferior glenoid rim
- Sling effect: conjoint tendon creates dynamic reinforcement in ABER position
- Soft tissue repair: capsular reattachment to CA ligament remnant restores bumper
Key Surgical Steps
- Deltopectoral approach, identify and protect cephalic vein
- Osteotomise coracoid at base distal to coracoclavicular ligaments
- Preserve conjoint tendon attachment, release pectoralis minor medially
- Decorticate anterior glenoid neck, position graft flush with rim
- Fix with two parallel bicortical screws, confirm position with fluoroscopy
Complications
- Graft nonunion (5-15 percent), resorption (up to 30 percent partial), fracture (2-10 percent)
- Recurrence (1-5 percent) — usually from medial graft or resorption
- Musculocutaneous nerve (5-8 cm from coracoid tip) and axillary nerve at risk
- Hardware irritation (5-15 percent), late OA (20-30 percent at 10+ years)
Bristow vs Latarjet
- Bristow: coracoid tip with CA ligament, single screw — largely historical
- Latarjet: full coracoid flat on glenoid, two screws — current gold standard
- Congruent arc: coracoid rotated 90 degrees for better articular congruence
- Both create triple blocking effect but Latarjet provides larger bone block
Evidence Base and Key Trials
The open Latarjet procedure is more reliable in terms of shoulder stability than arthroscopic Bankart repair
- Prospective comparative study of arthroscopic Bankart versus open Latarjet in patients with recurrent anterior instability
- Open Latarjet group had significantly lower recurrence rate compared with arthroscopic Bankart group
- Better outcomes in Latarjet group for sport participation and patient-reported scores
- Higher complication rate in Latarjet group but most were minor and self-limiting
Long-Term Restoration of Anterior Shoulder Stability: A Retrospective Analysis of Arthroscopic Bankart Repair Versus Open Latarjet Procedure
- Retrospective comparison of arthroscopic Bankart repair versus open Latarjet at long-term follow-up
- Latarjet group had significantly lower recurrence rate compared with Bankart group
- Progression of osteoarthritis seen in a significant proportion at long-term follow-up
- Patient satisfaction remained high despite radiographic arthritis changes
A systematic review and meta-analysis of clinical and patient-reported outcomes following two procedures for recurrent traumatic anterior instability of the shoulder: Latarjet procedure vs. Bankart repair
- Systematic review and meta-analysis comparing Latarjet versus Bankart repair for recurrent anterior instability
- Pooled recurrence rate was significantly lower after Latarjet compared with Bankart repair
- Graft nonunion and hardware complications were the most common surgical complications of Latarjet
- Neurological injury was uncommon and typically transient
Complications and re-operations after Bristow-Latarjet shoulder stabilization: a systematic review
- Systematic review of 45 studies reporting complications after Bristow-Latarjet shoulder stabilization
- Overall complication rate was approximately 15-30 percent across all reported series
- Nerve injury (mostly neuropraxia) occurred in 1-8 percent of cases, with axillary and musculocutaneous nerves most commonly affected
- Hardware-related complications and graft nonunion were the most frequent indications for re-operation
Results of modified Latarjet reconstruction in patients with anteroinferior instability and significant bone loss
- Case series of modified Latarjet reconstruction in patients with anteroinferior instability and significant glenoid bone loss
- Excellent results with very low recurrence rate in patients with inverted pear glenoids
- Demonstrated that coracoid transfer effectively addresses instability in the setting of bone deficiency where soft tissue repair alone would fail
- Established the rationale for the congruent arc modification of the Latarjet technique