External rotation/open book injuries - high hemorrhage risk
Young-Burgess APC Classification
Critical Must-Knows
- HEMORRHAGE is the primary killer - massive pelvic volume expansion
- External rotation opens pelvic ring increasing pelvic volume
- Binder/sheet CLOSES the book - early hemorrhage control
- APC-II = 'open book' with intact posterior SI ligaments
- APC-III = complete SI disruption = highest mortality
Clinical Pearls
- "Symphysis widening 2.5cm is key threshold (APC-I vs II)
- "Posterior injury determines stability - not anterior widening
- "Urgent pelvic binder before imaging in unstable patients
- "External fixator for anterior stabilization, NOT definitive for posterior
- "Assess for urological injury - bladder and urethra at high risk
Exam Warning
Hemorrhage Mechanism
Volume Expansion: External rotation 'opens the book', creating a massive potential space for venous bleeding.
Life-Saving Maneuver
CLOSE THE BOOK: Pelvic binder/sheet at GT level restores tamponade. Do this before CT if unstable.
The 2.5cm Rule
<2.5cm: APC-I (Posterior ligaments intact, stable). >2.5cm: APC-II (Anterior SI torn, rotationally unstable).
Stability Check
Do NOT 'spring' the pelvis repeatedly. One gentle check only. Clots can dislodge.
At a Glance
| Feature | APC-I | APC-II | APC-III |
|---|---|---|---|
| Symphysis widening | Less than 2.5cm | Greater than 2.5cm | Greater than 2.5cm + vertical |
| Posterior SI ligaments | Intact | Intact | Disrupted |
| Sacrospinous ligament | Intact | Torn | Torn |
| Rotational stability | Stable | Unstable | Unstable |
| Vertical stability | Stable | Stable | Unstable |
| Hemorrhage risk | Moderate | High | Very high |
| Typical management | Conservative | Surgical fixation | Urgent surgical fixation |
OPENAPC - Key Features
| O | Opens Opens pelvic ring (external rotation mechanism) |
| P | Posterior Posterior ligaments determine stability |
| E | Exsanguination Exsanguination risk is highest of all patterns |
| N | Need Need urgent binder to CLOSE the book |
| O | Opens Opens pelvic ring (external rotation mechanism) | E | Exsanguination Exsanguination risk is highest of all patterns |
| P | Posterior Posterior ligaments determine stability | N | Need Need urgent binder to CLOSE the book |
Hook:APC injuries OPEN the pelvis - remember to CLOSE it with a binder
BLEEDBLEED - Why APC Hemorrhages
| B | Book Book opens - volume expands dramatically |
| L | Lost Lost tamponade effect from intact ring |
| E | External External rotation tears venous plexus |
| E | Eighty Eighty percent of bleeding is venous |
| D | Dangerous Dangerous - highest mortality pattern |
| B | Book Book opens - volume expands dramatically | E | Eighty Eighty percent of bleeding is venous |
| L | Lost Lost tamponade effect from intact ring | D | Dangerous Dangerous - highest mortality pattern |
| E | External External rotation tears venous plexus |
Hook:APC injuries BLEED - the open book loses tamponade
2.5TWO-FIVE - APC-I vs APC-II Threshold
| 2 | Two Two point five centimeters is the critical threshold |
| . | Decimal Decimal point reminds you - precision matters |
| 5 | Five Five mm normal, 25 mm is the cutoff |
| 2 | Two Two point five centimeters is the critical threshold |
| . | Decimal Decimal point reminds you - precision matters |
| 5 | Five Five mm normal, 25 mm is the cutoff |
Hook:2.5cm symphysis widening separates APC-I (conservative) from APC-II (surgical)
BINDBIND - Pelvic Binder Protocol
| B | Below Below iliac crests at greater trochanter level |
| I | Internal Internal rotation force closes the book |
| N | Not Not too tight - check skin, reassess in 24 hours |
| D | Definitive Definitive fixation needed - binder is temporary |
| B | Below Below iliac crests at greater trochanter level | N | Not Not too tight - check skin, reassess in 24 hours |
| I | Internal Internal rotation force closes the book | D | Definitive Definitive fixation needed - binder is temporary |
Hook:BIND the pelvis to close the open book - applied at trochanter level
Overview
Introduction
Anteroposterior compression (APC) injuries result from external rotation forces applied to the pelvis, classically from direct anterior impact or forced external rotation of the lower extremities. These injuries "open" the pelvic ring like a book, disrupting anterior structures first and progressing posteriorly with increasing force.
APC injuries are critical to understand because they have the highest hemorrhage risk of all pelvic injury patterns. The external rotation mechanism opens the pelvic ring, dramatically increasing pelvic volume and allowing massive retroperitoneal hemorrhage from venous plexus disruption and arterial bleeding.

Epidemiology
Incidence:
- 15-20% of all pelvic ring injuries
- Second most common pattern after LC injuries
- Most common cause of massive pelvic hemorrhage
Mechanism:
- Motorcycle accidents (handlebar impact)
- Pedestrian vs vehicle (direct anterior blow)
- Falls with legs forced into external rotation
- Crush injuries with AP vector
Demographics:
- Young males predominate (high-energy trauma)
- Associated polytrauma in majority
- Higher ISS scores than LC injuries typically
Clinical Significance
Why APC Injuries Are High-Stakes:
- Hemorrhage risk: Highest of all patterns
- Volume expansion: Pelvis can accommodate several liters of blood
- Venous plexus: Presacral venous plexus disruption
- Arterial injury: Superior gluteal artery vulnerable
- Urological injury: Bladder and urethra directly affected by symphysis disruption
Anatomy and Pathophysiology
Pelvic Ring Biomechanics
The pelvis functions as a ring structure with anterior and posterior components. Stability primarily depends on the posterior structures.
Anterior Structures
Pubic Symphysis:
- Fibrocartilaginous joint
- Minimal inherent stability
- Disruption alone does not cause instability
- Normal width approximately 5mm
Pubic Rami:
- Connect symphysis to acetabulum
- Fractures common with symphysis disruption
- Bilateral rami fractures may occur
Posterior Structures (Critical for Stability)
Sacroiliac Joint:
- Anterior SI ligaments: First to fail in APC
- Interosseous SI ligaments: Main restraint to external rotation
- Posterior SI ligaments: Ultimate stability (strongest)
- Sacrospinous ligament: Resists external rotation
- Sacrotuberous ligament: Resists vertical displacement
APC Injury Progression
Force applied anteriorly causes sequential failure:
- Stage 1 (APC-I): Symphysis diastasis, anterior SI strain, posterior intact
- Stage 2 (APC-II): Complete anterior SI tear, sacrospinous ligament tear, posterior SI intact
- Stage 3 (APC-III): Complete SI disruption including posterior ligaments

Hemorrhage Mechanism
Why APC Bleeds Most:
Volume Expansion:
- Normal pelvic volume approximately 1.5L
- APC-III can increase to greater than 4L
- Tamponade effect lost when ring opens
Vascular Anatomy:
- Presacral venous plexus: Low pressure, high volume
- Internal iliac branches: Superior gluteal artery most common
- Corona mortis: Aberrant obturator vessels (present in 30%)
Bleeding Sources:
- 80-90% venous (plexus disruption)
- 10-20% arterial (often superior gluteal)
- Cancellous bone surfaces contribute
Classification
Young-Burgess APC Classification
The Young-Burgess classification stratifies APC injuries by severity and stability based on progressive ligamentous disruption.

APC-I (Stable)
Definition: Symphysis widening less than 2.5cm
Structures Disrupted:
- Symphysis pubis (partial)
- Anterior SI ligaments (sprained, not torn)
Structures Intact:
- Sacrospinous ligament
- Sacrotuberous ligament
- Posterior SI ligament complex
- Interosseous SI ligaments
Clinical Features:
- Mechanically stable
- Moderate hemorrhage risk
- Usually ambulatory with weight-bearing restrictions
- Conservative management often appropriate
The 2.5cm threshold is the key differentiator for APC-I injuries.
Clinical Assessment
Primary Survey
APC injuries are diagnosed in the context of major trauma. Pelvic assessment follows ATLS principles.
Mechanism History
High-Risk Mechanisms:
- Motorcycle collision (handlebars)
- Pedestrian struck anteriorly
- Frontal vehicle collision with AP force vector
- Crush injury with anterior compression
- Fall from height with legs apart
Physical Examination
Inspection:
- Limb length discrepancy (APC-III)
- External rotation deformity of lower limbs
- Perineal swelling/ecchymosis
- Scrotal or labial hematoma
- Visible symphysis widening (severe cases)
- Blood at urethral meatus
Do NOT repeatedly "spring" or compress the pelvis. A single gentle assessment is acceptable - repeated manipulation can dislodge clot and restart hemorrhage. If instability is suspected, apply a binder and obtain imaging.
Palpation (gentle, once only):
- Symphysis gap palpable
- Tenderness over SI joints posteriorly
- Iliac crest tenderness
Associated Injuries (Always Assess):
Urological:
- Blood at meatus: High-riding prostate, urethral injury
- Hematuria: Bladder injury
- Do NOT catheterize if urethral injury suspected
Vascular:
- Peripheral pulses
- Signs of hypovolemic shock
- Expanding hematoma
Neurological:
- L5/S1 nerve root function
- Perineal sensation (S2-4)
- Rectal tone
Hemodynamic Assessment
Unstable Patient:
- Tachycardia greater than 100 bpm
- Hypotension (SBP less than 90mmHg)
- Reduced GCS (hypoperfusion)
- Poor peripheral perfusion
- Need for ongoing resuscitation
Presumed Pelvic Source If:
- Pelvic instability on examination
- No other obvious hemorrhage source
- High-risk mechanism
- APC pattern on imaging
Differential Diagnosis
The "open book" appearance and pelvic instability of an APC injury must be distinguished from other patterns that look similar on the AP film but demand opposite management (for example, a binder is contraindicated in lateral compression).
Differential Diagnosis of the Widened / Unstable Pelvis
| Condition | Mechanism / vector | Key distinguishing feature | Management contrast |
|---|---|---|---|
| APC (open book) | Anterior force, external rotation | Symphysis widening greater than 2.5cm, pelvis opens | Binder CLOSES the book - first line |
| Lateral compression (LC) | Lateral force, internal rotation | Overlapping/impacted rami, pelvis closes; sacral impaction | Binder may over-compress - apply with caution |
| Vertical shear (VS) | Axial/vertical force (fall from height) | Cephalad hemipelvis migration on outlet view | Needs traction plus posterior fixation, not binder alone |
| Acetabular fracture | Force through femoral head | Disruption of acetabular lines (iliopectineal/ilioischial), ring often intact | Binder may displace - protected/ORIF pathway |
| Physiological symphyseal widening (pregnancy/peripartum) | Hormonal laxity, not trauma | No high-energy mechanism, typically less than 1cm, no posterior injury | Conservative; pelvic support, analgesia |
| Isolated pubic rami fracture (low energy, elderly) | Low-energy fall | Stable ring, no symphysis diastasis or SI disruption | Conservative, early mobilisation |
Investigations
Imaging Approach
Plain Radiography
AP Pelvis:
- First-line imaging in trauma
- Can be done in resuscitation bay
- Assess symphysis width (normal approximately 5mm)
- Greater than 25mm suggests APC-II or higher
- Look for associated pubic rami fractures
- Evaluate SI joint symmetry
Inlet View:
- Demonstrates AP displacement
- Shows symphysis diastasis clearly
- Evaluates SI joint anteriorly
Outlet View:
- Demonstrates vertical displacement
- Better view of sacrum
- Helps differentiate APC-III from APC-II
CT Imaging
Indications:
- All stable patients with suspected pelvic injury
- Hemodynamically stable patients for surgical planning
- Define posterior injury pattern precisely
Findings:
- Symphysis diastasis measurement
- Anterior SI joint widening
- Posterior SI ligament integrity
- Associated fractures (sacrum, rami)
- Contrast extravasation (CT angiography)
CT Angiography:
- Active arterial extravasation
- Guides angioembolization
- Superior gluteal artery most common source
Retrograde Urethrogram
Indications:
- Blood at urethral meatus
- High-riding prostate on DRE
- Perineal hematoma
- Before catheterization if urethral injury suspected
Technique:
- 20-30mL water-soluble contrast
- Inject gently via meatus
- Fluoroscopic or plain film guidance
Cystogram
Indications:
- Hematuria with pelvic fracture
- After urethral integrity confirmed
- Evaluate for bladder rupture
Findings:
- Intraperitoneal rupture: Contrast around bowel
- Extraperitoneal rupture: Flame-shaped extravasation (more common with APC)
Management
Acute Hemorrhage Control
The pelvic binder is FIRST-LINE treatment for suspected APC injury with hemodynamic instability. Apply BEFORE imaging. The binder CLOSES the open book, reducing pelvic volume and restoring tamponade. Do not wait for X-ray confirmation.
Pelvic Binder Application
Principles:
- Applies internal rotation force
- Closes the "open book"
- Reduces pelvic volume
- Restores tamponade effect
- Temporary measure (not definitive)
Technique:
- Position at level of greater trochanters (NOT iliac crests)
- Apply circumferential compression
- Commercial binder or sheet wrap acceptable
- Do not over-tighten (skin necrosis risk)
- Re-evaluate after 24-48 hours maximum
Contraindications:
- LC injuries (already internally rotated - binder makes worse)
- Acetabular fractures (may displace)
Damage Control Resuscitation
Principles:
- Permissive hypotension (SBP 80-90mmHg)
- Balanced transfusion (1:1:1 ratio)
- Avoid crystalloid overload
- Early TXA administration
- Correct coagulopathy aggressively
Early mechanical stabilization combined with damage control resuscitation saves lives.
Surgical Technique
Anterior Symphysis Fixation
Indications:
- APC-II injuries (symphysis widening over 2.5cm)
- APC-III injuries (combined with posterior fixation)
- Symphysis diastasis over 2.5cm with rotational instability
Pfannenstiel Approach:
- Transverse skin incision 2cm above symphysis
- Incise linea alba vertically
- Protect bladder (retract inferiorly)
- Expose symphysis and superior pubic rami
- Reduce symphysis with clamp
- Apply superior pubic plate (3.5mm reconstruction plate)
- 4-6 hole plate preferred for stability
Technical Pearls:
- Reduce symphysis before plating
- Superior plate position (strongest)
- Protect bladder throughout
- Consider second inferior plate for APC-III
The Pfannenstiel approach provides excellent access with minimal soft tissue damage.

Complications
Associated Injuries
Urological Injuries
Bladder Injury:
- 15-25% of APC injuries
- Extraperitoneal more common (symphysis disruption)
- Intraperitoneal with full bladder at impact
- Hematuria is key finding
Management:
- Extraperitoneal: Catheter drainage 10-14 days
- Intraperitoneal: Surgical repair required
Urethral Injury:
- More common in males (long membranous urethra)
- Blood at meatus, high-riding prostate
- Do NOT blind catheterize
- Retrograde urethrogram first
- Suprapubic catheter if complete disruption
Vascular Injuries
Arterial:
- Superior gluteal artery most common
- Internal iliac branches
- Corona mortis (variant obturator vessels)
Venous:
- Presacral venous plexus (major source)
- Internal iliac veins
- Low pressure but high volume bleeding
Neurological Injuries
Lumbosacral Plexus:
- L5 nerve root most vulnerable
- Foot drop, sensory loss
- S2-4 sacral roots: Bladder, bowel, sexual function
Documentation Essential:
- Motor function L2-S1
- Sensory examination
- Perineal sensation
- Rectal tone
Open Pelvic Fractures
Faringer Classification:
- Type I: Iliac wing (low risk)
- Type II: Perineum/buttock (moderate)
- Type III: Rectum/vagina (high mortality)
Management:
- Fecal diversion for rectal involvement
- Wound debridement
- Broad spectrum antibiotics
- High mortality (up to 50%)
Early Complications
Hemorrhagic Shock:
- Most common cause of early death
- Massive transfusion requirements
- Coagulopathy compounds bleeding
Thromboembolic Events:
- High DVT risk (venous stasis, injury)
- PE can be fatal
- Early prophylaxis when safe
Infection:
- Open fractures: High mortality
- Surgical site infections
- Osteomyelitis rare with closed injuries
Late Complications
Malunion:
- Residual diastasis
- SI joint malreduction
- Affects gait and pain
Nonunion:
- Rare with adequate fixation
- Symphysis nonunion: Painful instability
- SI nonunion: May need fusion
Hardware Issues:
- Symphysis plate loosening (activity related)
- Screw pullout
- May need removal if symptomatic
Chronic Pain:
- SI joint arthritis
- Symphysis pain
- May benefit from SI fusion
Sexual and Urological:
- Dyspareunia
- Erectile dysfunction
- Chronic urethral stricture
Postoperative Care
Immediate Postoperative (Days 0-14)
ICU Management:
- Continued hemodynamic monitoring
- Serial hemoglobin checks
- DVT prophylaxis (LMWH when hemostasis achieved)
- Early removal of pelvic binder (once fixation stable)
Mobility:
- Bed rest initially for severe injuries
- Toe-touch weight-bearing when hemodynamically stable
- Log-roll precautions for posterior fixation
Wound Care:
- Monitor surgical incisions
- Pin site care for external fixation
- Watch for infection signs
Early mobilization improves outcomes but must be balanced against injury stability.
Outcomes and Prognosis
Overall Outcomes
Mortality:
- APC-I: Under 5%
- APC-II: 5-15%
- APC-III: Up to 25%
- Mortality correlates with associated injuries and hemorrhage
Functional Outcomes:
Outcomes by APC Grade
| APC Grade | Union Rate | Return to Work | Chronic Pain |
|---|---|---|---|
| APC-I | Over 95% | 3-4 months | 10-15% |
| APC-II | 90-95% | 4-6 months | 20-30% |
| APC-III | 85-90% | 6-12 months | 40-50% |
Long-term Complications
Chronic Pain:
- SI joint pain: 20-40% of APC-II/III
- Symphysis pain: 15-25%
- Sacral fracture malunion: contributor to pain
Sexual Dysfunction:
- More common with urethral injury
- Erectile dysfunction: 15-30% in males
- Dyspareunia: 20-40% in females
Leg Length Discrepancy:
- Rare with accurate reduction
- May result from malreduction of vertical component
Prognosis depends heavily on initial injury severity and associated injuries.
Evidence Base
Young-Burgess Classification (Landmark)
- Series of 210 high-energy pelvic ring disruptions stratified by force vector into lateral compression, anteroposterior compression, vertical shear and combined mechanical injury - the basis of the Young-Burgess system.
- Anteroposterior compression injuries had the highest mean blood replacement (14.8 units vs 3.6 for lateral compression) and the highest pattern-specific mortality (20%).
WSES Classification & Guidelines for Pelvic Trauma
- International consensus classifying pelvic trauma primarily by haemodynamic status rather than fracture pattern alone, and integrating non-invasive compression, pre-peritoneal packing, angioembolisation and REBOA.
- Recommends immediate circumferential pelvic compression and physiology-driven escalation in unstable patients.
CRASH-2: Tranexamic Acid in Trauma Haemorrhage (Landmark RCT)
- 20,211 trauma patients across 40 countries; tranexamic acid reduced all-cause mortality (14.5% vs 16.0%, RR 0.91, 95% CI 0.85-0.97) with no excess vascular occlusive events.
- Death due to bleeding was significantly reduced (4.9% vs 5.7%, RR 0.85, 95% CI 0.76-0.96).
Evolution of Algorithms for Unstable Pelvic Ring Injuries
- Systematic review of 32 published treatment algorithms over ~40 years; use of pelvic binders/sheets and CT plus angiography has risen steadily while diagnostic peritoneal lavage has become obsolete.
- Physiological assessment remains the central trigger for escalation, with external fixation the most commonly used stabilisation technique and REBOA/INFIX increasingly incorporated.
Predictors of Mortality After Severe Pelvic Ring Fracture (Registry)
- 348 severe pelvic ring fractures from the population-based Victorian State Trauma Registry (Australia); overall mortality 19%.
- Scene hypotension (AOR 5.5), admission hypotension (AOR 3.7) and age 65 years or older (AOR 7.6) independently predicted death; definitive hospital did not after adjustment.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
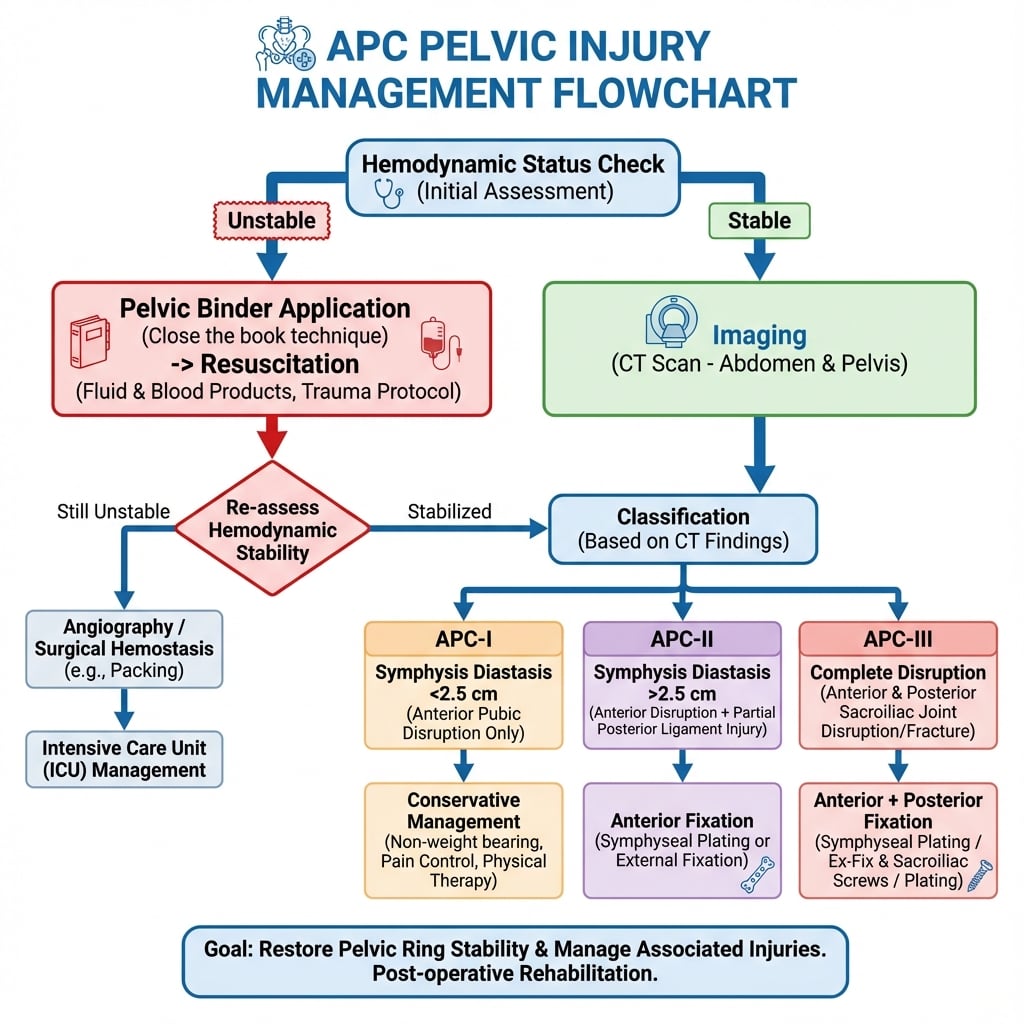
Unstable APC Injury Management
"A 35-year-old motorcyclist presents after a head-on collision. He is tachycardic (HR 125), hypotensive (BP 85/50), and has gross external rotation of both lower limbs. AP pelvis shows symphysis diastasis of 4cm. Describe your immediate management."
Immediate Recognition: This is an APC-II or APC-III injury with hemodynamic instability - life-threatening hemorrhage.
Immediate Actions (Simultaneous):
- Pelvic binder at greater trochanter level - CLOSE THE BOOK
- Massive transfusion protocol activation (1:1:1)
- TXA administration (1g IV)
- Permissive hypotension (target SBP 80-90)
- Avoid crystalloid overload
Secondary Assessment:
- Complete ATLS primary and secondary survey
- Identify other hemorrhage sources
- Check for blood at urethral meatus - do NOT blind catheterize
- Perineal/rectal examination for open fracture
If Responding to Resuscitation:
- CT with angiography
- Define posterior injury (APC-II vs III)
- Angioembolization if arterial blush
- Definitive fixation when stable
If NOT Responding:
- Consider external fixator in ED
- Preperitoneal packing
- Angioembolization if available
- REBOA as bridge if trained personnel
Young-Burgess APC Classification
"Describe the Young-Burgess APC classification and explain why understanding this system is important for management decisions."
Young-Burgess APC Classification:
APC-I:
- Symphysis widening less than 2.5cm
- Anterior SI ligaments sprained but intact
- Posterior ligaments completely intact
- Mechanically STABLE
- Usually conservative management
APC-II (Open Book):
- Symphysis widening greater than 2.5cm
- Anterior SI ligaments disrupted
- Sacrospinous ligament torn
- Posterior SI ligaments INTACT (key distinction)
- Rotationally unstable, vertically stable
- Surgical fixation of symphysis usually required
APC-III:
- Complete SI disruption (anterior AND posterior)
- Hemipelvic external rotation
- Rotationally AND vertically unstable
- Highest hemorrhage and mortality risk
- Requires anterior AND posterior fixation
Clinical Importance:
- Hemorrhage risk increases with grade
- APC-I may be managed conservatively
- APC-II needs anterior fixation only
- APC-III needs BOTH anterior and posterior fixation
- Posterior injury determines stability - not anterior widening
Symphysis Fixation Technique
"A patient with an APC-II pelvic injury is scheduled for symphysis fixation. Describe your surgical approach and technique."
Preoperative Planning:
- Confirm APC-II (CT showing intact posterior SI ligaments)
- Review for associated injuries (bladder, urethra)
- Ensure hemodynamic stability
- Discuss with urology if catheter issues
Positioning:
- Supine on radiolucent table
- Ensure fluoroscopy access (inlet, outlet, AP views)
- Prep widely including both iliac crests
Approach:
- Pfannenstiel incision (transverse, 2cm above symphysis)
- Incise rectus sheath transversely
- Separate rectus muscles in midline (do NOT detach)
- Identify and protect bladder (often contused)
- Expose superior pubic ramus bilaterally
Reduction:
- Large pointed reduction forceps across symphysis
- Reduce internal rotation to close the book
- Confirm reduction on inlet view (symmetric ring)
- Accept less than 1cm residual diastasis
Fixation:
- 3.5mm reconstruction plate or specific symphysis plate
- Position on superior aspect of pubis
- 2-hole plate for simple diastasis
- 4-hole plate if rotational control needed
- Consider second plate superiorly if highly unstable
Closure:
- Close rectus sheath securely
- Subcutaneous and skin closure
- Catheter remains for bladder monitoring
MCQ Practice Points
Classification Question
Q: What symphysis widening threshold distinguishes APC-I from APC-II? A: 2.5cm. Less than 2.5cm = APC-I (stable, usually conservative). Greater than 2.5cm = APC-II or III (unstable, usually surgical).
Stability Question
Q: What determines stability in APC injuries - anterior or posterior structures? A: Posterior ligaments. The posterior SI ligament complex determines stability. APC-II has intact posterior ligaments (rotationally unstable). APC-III has complete disruption (globally unstable).
Pelvic Binder Question
Q: Where should the pelvic binder be positioned? A: At the level of the greater trochanters (NOT the iliac crests). This applies internal rotation force to close the "open book."
Contraindication Question
Q: What pelvic injury pattern is a CONTRAINDICATION to pelvic binder? A: Lateral compression (LC) injuries. The pelvis is already internally rotated - a binder would worsen the deformity.
Hemorrhage Question
Q: What percentage of pelvic hemorrhage is venous vs arterial? A: 80% venous, 20% arterial. The pelvic binder addresses venous bleeding by restoring tamponade. Angioembolization targets arterial bleeding.
Guidelines, Registries & Global Practice
Global Epidemiology
- Severe pelvic ring disruption is uncommon but high-lethality. In the population-based Victorian State Trauma Registry (Australia), overall mortality after severe pelvic ring fracture was 19%, with scene/admission hypotension and age 65 years or older as the dominant predictors (Gabbe et al., 2011, PMID 21733513).
- In the original Young-Burgess cohort, the APC pattern carried the highest pattern-specific mortality (20%) and the greatest transfusion requirement (mean 14.8 units) of all pelvic patterns (Burgess et al., 1990, PMID 2381002).
- High-energy mechanisms (motor vehicle, motorcycle, pedestrian, fall from height) dominate worldwide; bimodal age distribution exists, with high-energy injuries in younger patients and lower-energy ring injuries in older patients.
Side-by-Side Guideline & System Guidance
International Guidance on Unstable APC/Pelvic Haemorrhage
| Body / System | Core recommendation | Evidence basis |
|---|---|---|
| WSES (global consensus) | Classify by haemodynamic status; immediate circumferential compression then physiology-guided escalation (packing / angioembolisation / REBOA) | Consensus guideline (PMID 28115984) |
| ATLS / ACS (North America) | Pelvic binder at trochanters in suspected unstable ring injury before imaging; balanced 1:1:1 transfusion | Course/consensus standard |
| NICE NG37 (UK) | Apply purpose-made pelvic binder for suspected active bleeding from pelvic fracture; CT in haemodynamically normal/stabilised adults | Guideline (level varies) |
| BOAST / BOA (UK) | Time-critical transfer to specialist pelvic unit; binder plus damage-control resuscitation; definitive fixation by pelvic surgeon | Standard of care |
| AO Foundation | Anterior fixation for rotational (APC-II) instability; combined anterior plus posterior fixation for APC-III; percutaneous SI screws for posterior ring | Technique consensus |
Tranexamic Acid and Resuscitation
The CRASH-2 randomised trial established that tranexamic acid given within 3 hours of injury reduces all-cause and bleeding-related mortality in trauma haemorrhage without increasing vascular occlusive events (PMID 20554319). It is now embedded in essentially all major trauma-system massive transfusion protocols globally.
Registry & Practice-Variation Evidence
- Registry data (Victorian State Trauma Registry) show no independent association between the definitive hospital and mortality after adjustment, reinforcing that rapid physiological control rather than the receiving centre drives survival (PMID 21733513).
- A 40-year systematic review of published algorithms confirms convergence of global practice: steadily rising use of pelvic binders/sheets and CT plus angiography, external fixation as the most common stabilisation technique, and increasing incorporation of REBOA and INFIX, while diagnostic peritoneal lavage has been abandoned (PMID 39731120).
- Persistent variation remains in the first-line haemorrhage adjunct: many North American centres favour pre-peritoneal packing, while several European and Asian centres prioritise early angioembolisation - the WSES framework accommodates both within a physiology-led pathway.
Australian Context
Australian inclusive trauma systems triage suspected unstable pelvic injuries to major trauma services with rapid binder application and damage-control resuscitation, aligning with WSES principles. Venous thromboembolism prophylaxis uses low-molecular-weight heparin (enoxaparin, PBS-listed) once haemostasis is achieved, typically continued for several weeks with extended prophylaxis for prolonged immobility. State-funded rehabilitation networks support functional recovery, though chronic pain after higher-grade injuries remains a significant long-term burden.
Exam Focus Points
High-Yield Concepts
Clinical Pearl
The 2.5cm symphysis widening threshold is CRITICAL for exam purposes. Less than 2.5cm = APC-I (stable, usually conservative). Greater than 2.5cm = APC-II or III (unstable, usually surgical). This simple number drives management decisions.
Key Differentiators
APC vs LC Injuries:
- APC: External rotation, pelvis OPENS
- LC: Internal rotation, pelvis CLOSES
- APC: Higher hemorrhage (volume expands)
- LC: Associated head injury (same vector)
APC-II vs APC-III:
- Both have symphysis widening greater than 2.5cm
- APC-II: Posterior SI ligaments INTACT (key)
- APC-III: Complete SI disruption
- APC-II: Anterior fixation only
- APC-III: Anterior AND posterior fixation
Hemorrhage Management Sequence
- Recognize APC pattern and instability
- BIND - Pelvic binder at trochanters
- Resuscitate - MTP, TXA, permissive hypotension
- Image - When stable enough for CT
- Intervene - Angioembolization if arterial source
- Fix - Definitive surgical stabilization
Surgical Fixation Principles
Anterior (Symphysis):
- Pfannenstiel approach
- Superior plate position
- Protect bladder
- 2-4 hole plate
Posterior (SI Joint):
- Percutaneous SI screws (most common)
- S1 body target (avoid ala)
- Protect L5 nerve root
- May need multiple screws
APC Pelvic Injuries
Clinical summary
Classification
- •APC-I: Symphysis less than 2.5cm, stable
- •APC-II: Symphysis greater than 2.5cm, posterior SI intact
- •APC-III: Complete SI disruption, unstable
- •Posterior ligaments determine stability
Hemorrhage
- •HIGHEST hemorrhage risk of all patterns
- •80% venous, 20% arterial bleeding
- •Pelvic binder addresses venous component
- •Angioembolization for arterial bleeding
Immediate Management
- •Pelvic binder at TROCHANTERS (not iliac crests)
- •MTP activation (1:1:1 ratio)
- •TXA 1g IV
- •Permissive hypotension (SBP 80-90)
Surgical Fixation
- •APC-II: Symphysis plating only
- •APC-III: BOTH anterior AND posterior fixation
- •Pfannenstiel approach for symphysis
- •SI screws target S1 body (avoid ala)
Key Pitfalls
- •Delaying binder for imaging
- •Binder at iliac crests (too high)
- •Blind catheterization with blood at meatus
- •LC injuries contraindicate binder