Non-Tuberculous Mycobacteria | M. marinum Classic | Rice Body Tenosynovitis | Prolonged Multi-Drug Therapy
- High index of suspicion in chronic culture-negative infection with granulomatous histology
- M. marinum is classic for hand tenosynovitis after aquarium or fish exposure (fish tank granuloma)
- Rice bodies in tenosynovitis are pathognomonic - fibrin deposits within tendon sheath
- AFB culture takes 2-6 weeks - must specifically request mycobacterial culture
- Surgical debridement PLUS prolonged antibiotics (3-6 months) is standard treatment
- “M. marinum optimal growth at 30-32C (cooler extremities) - incubate at lower temperature
- “Rapidly growing mycobacteria cause post-surgical wound infections (M. fortuitum, M. abscessus)
- “MAC disseminated infection occurs in severely immunocompromised (CD4 count less than 50)
- “Clarithromycin is the cornerstone of most NTM regimens - never use as monotherapy
Think NTM in: chronic indolent tenosynovitis, culture-negative joint infection, chronic wound with granulomas, atypical presentation not responding to standard antibiotics, immunocompromised host, aquarium/fish exposure, post-procedural wound infection.
Classic presentation: Aquarium enthusiast, fish handler, or swimming pool exposure presenting with nodular hand/wrist tenosynovitis weeks to months later. May have sporotrichoid spread (ascending nodules along lymphatics). Optimal growth at 30-32C - cool incubation required.
Pathognomonic finding: Multiple white rice-grain sized bodies within tendon sheath. Fibrin deposits from chronic inflammation. Classic for NTM but also seen in TB and rheumatoid arthritis. Requires synovectomy and prolonged antibiotics for cure.
AFB culture takes 2-6 weeks - must specifically request. Standard bacterial cultures negative. Histology shows granulomas with or without caseation. PCR allows rapid species identification. AFB smear often negative (low organism burden).
| Organism | Source/Exposure | Clinical Presentation | Treatment Approach |
|---|---|---|---|
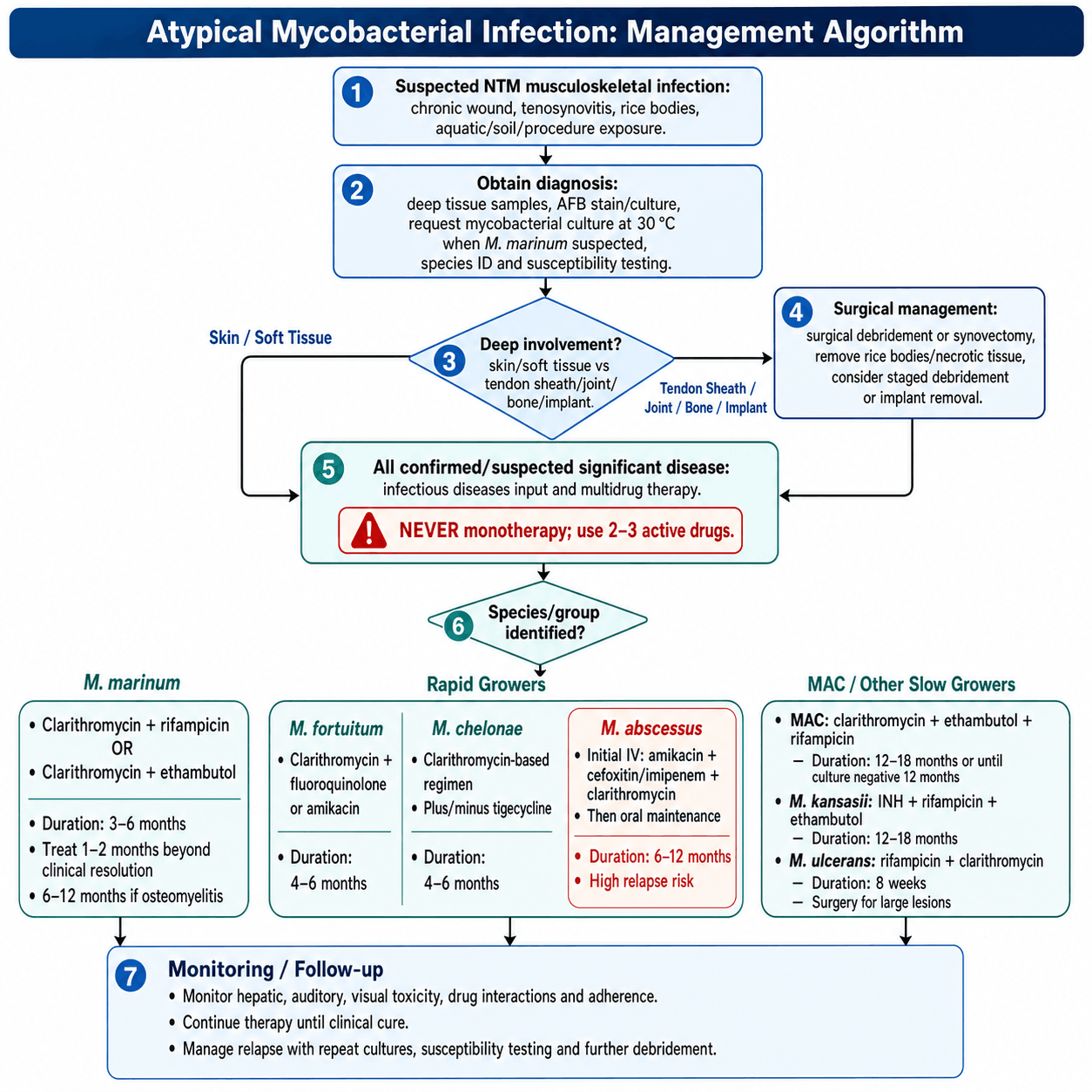
| M. marinum | Aquarium, fish, swimming pools | Hand/wrist tenosynovitis, sporotrichoid spread | Clarithromycin + rifampicin OR ethambutol, 3-6 months |
| M. avium complex (MAC) | Environmental (soil, water) | Disseminated in AIDS, pulmonary in elderly, rare joint infection | Clarithromycin + ethambutol +/- rifampicin, 12+ months |
| M. kansasii | Water supply, geographic clusters | Pulmonary TB-like, tenosynovitis, osteomyelitis | Isoniazid + rifampicin + ethambutol, 12-18 months |
| M. fortuitum | Soil, water, surgical contamination | Post-surgical wound infection, catheter infection | Clarithromycin + amikacin +/- fluoroquinolone, 4-6 months |
| M. chelonae | Soil, water, contaminated solutions | Skin/soft tissue, post-injection abscess | Clarithromycin-based, avoid aminoglycosides (resistant) |
| M. abscessus | Water, contaminated equipment | Post-surgical, skin/soft tissue, most resistant rapid grower | Clarithromycin + amikacin + cefoxitin, most difficult to treat |
| M. ulcerans | Endemic zones (West/Central Africa, SE Australia, S. America, W. Pacific) | Buruli ulcer - painless progressive skin ulcer | Rifampicin + clarithromycin 8 weeks, surgery for large lesions |
FISH TANKNTM Suspicion Triggers
Hook:FISH TANK exposure should trigger suspicion for atypical mycobacteria - always ask about aquarium and water exposure!
SLOW vs FASTNTM Growth Rate Classification
Hook:SLOW growers from environment, FAST growers cause healthcare infections - both need multi-drug therapy!
AQUARIUMM. marinum Features
Hook:Think AQUARIUM when you see chronic hand tenosynovitis - M. marinum is the fish tank granuloma!
COMBONTM Treatment Principles
Hook:COMBO therapy is mandatory - clarithromycin plus additional agents for prolonged duration with surgical debridement!
Overview and Epidemiology
Atypical mycobacterial infections are commonly missed due to their indolent nature and the need for specific culture requests. In the exam, NTM should be considered in any chronic culture-negative tenosynovitis or wound, especially with exposure history. The key learning points are recognition, appropriate investigation, and understanding of prolonged multi-drug therapy.
- Increasing incidence worldwide over past decades
- Environmental organisms - soil, water, not human-to-human transmission
- M. marinum most common NTM causing hand infections
- MAC most common NTM overall in immunocompromised
- Rapid growers increasingly recognized in surgical site infections
- Risk factors: Immunosuppression, aquatic exposure, fish handling, tropical travel
- Tenosynovitis - especially hand and wrist flexor sheaths
- Septic arthritis - chronic, indolent presentation
- Osteomyelitis - less common, usually adjacent to soft tissue
- Post-surgical infection - rapid growers after procedures
- Bursitis - olecranon, prepatellar
- Often presents as culture-negative chronic infection
Definition
Non-Tuberculous Mycobacteria (NTM), also known as atypical mycobacteria or mycobacteria other than tuberculosis (MOTT), are a diverse group of acid-fast bacilli found ubiquitously in the environment. Unlike M. tuberculosis, they are not obligate human pathogens and do not require isolation precautions. They cause a spectrum of disease from localized skin and soft tissue infections to disseminated disease in immunocompromised hosts.
NTM infections are frequently missed because standard bacterial cultures do not detect them, and AFB cultures must be specifically requested. Always consider NTM in chronic indolent infections, especially in the hand, that fail standard antibiotic therapy and have negative routine cultures.
Aetiology and Microbiology
Runyon Classification of NTM
The traditional classification is based on growth rate and pigment production, though molecular identification is now standard.
| Group | Growth Rate | Pigment Production | Key Species |
|---|---|---|---|
| Group I - Photochromogens | Slow (more than 7 days) | Yellow pigment in light only | M. marinum, M. kansasii |
| Group II - Scotochromogens | Slow (more than 7 days) | Pigmented in dark and light | M. scrofulaceum, M. gordonae |
| Group III - Nonchromogens | Slow (more than 7 days) | No pigment production | M. avium complex, M. ulcerans |
| Group IV - Rapid growers | Fast (less than 7 days) | Variable | M. fortuitum, M. chelonae, M. abscessus |
Photochromogens (M. marinum, M. kansasii) produce yellow-orange pigment only when exposed to light. Scotochromogens produce pigment in both light and dark. Nonchromogens (MAC) produce no pigment. This traditional classification is still tested but molecular methods now provide definitive identification.
The classification helps predict clinical syndromes and guides initial therapy.
Clinical Presentation
NTM Tenosynovitis - Classic Presentation
Flexor tenosynovitis of the hand and wrist is the most common orthopaedic presentation of NTM infection, particularly M. marinum.
- Gradual onset over weeks to months
- Swelling along flexor tendon sheath
- Carpal tunnel syndrome from synovial thickening
- Variable pain - often less than expected for degree of swelling
- Finger triggering may be present
- Range of motion progressively limited
- Usually single digit or carpal tunnel region
- May extend to palm (horse-shoe abscess)
- Pathognomonic finding - white rice-grain sized bodies
- Represent fibrin deposits from chronic synovial inflammation
- Found within tendon sheath at surgery
- Classic for NTM but also seen in:
- Tuberculosis
- Rheumatoid arthritis
- Seronegative arthritis
- Require debridement/synovectomy for cure
When you encounter rice bodies at surgery for chronic tenosynovitis, always send tissue for AFB culture and TB culture in addition to routine bacterial culture and histology. The differential includes NTM (especially M. marinum), TB, and rheumatoid disease. Rice bodies are fibrin deposits, not the organisms themselves.
The classic triad is chronic tenosynovitis, rice bodies, and granulomatous histology - think mycobacteria.
Investigations and Diagnosis
Microbiological Diagnosis
| Test | Utility | Limitations |
|---|---|---|
| AFB smear (Ziehl-Neelsen) | Rapid, same-day result if positive | Low sensitivity (10-40%), paucibacillary infections often negative |
| AFB culture | Gold standard for diagnosis, allows susceptibility testing | Takes 2-6 weeks, must specifically request, temperature-dependent for M. marinum |
| PCR/NAAT | Rapid species identification, high sensitivity | Not available everywhere, cannot determine susceptibility |
| 16S rRNA sequencing | Definitive species identification | Takes days, reference laboratory needed |
| Histopathology | Granulomatous inflammation supports diagnosis | Non-specific, cannot identify species, may miss early infection |
AFB cultures are NOT performed unless specifically requested. In any chronic culture-negative musculoskeletal infection, always request: 1) AFB culture and smear, 2) Fungal culture, 3) Extended bacterial culture. For suspected M. marinum, request incubation at 30-32C.
Multiple tissue samples increase diagnostic yield.


Management
Management Principles
- Required for most NTM musculoskeletal infections
- Tenosynovectomy for flexor sheath involvement
- Debridement of infected/necrotic tissue
- Remove rice bodies and thickened synovium
- Obtain multiple tissue samples for culture
- May require staged procedures for extensive disease
- Always multi-drug regimens (prevents resistance)
- Duration 3-6 months minimum for skin/soft tissue
- 6-12+ months for bone/joint involvement
- Clarithromycin is cornerstone of most regimens
- Susceptibility testing guides specific choices
- Monitor for drug toxicity (hepatic, auditory, visual)
Mycobacterial infections must NEVER be treated with single-agent therapy. Resistance develops rapidly with monotherapy. Always use combination regimens with at least 2-3 active agents based on species identification and susceptibility testing.
Combined surgical debridement and prolonged multi-drug therapy is the standard of care.
Complications
| Complication | Cause | Prevention/Management |
|---|---|---|
| Treatment failure/relapse | Inadequate duration, non-compliance, drug resistance | Prolonged therapy, compliance support, susceptibility-guided treatment |
| Tendon rupture | Chronic tenosynovitis, steroid injection (misdiagnosis) | Avoid steroids if infection suspected, surgical debridement |
| Carpal tunnel syndrome | Synovial thickening, compression of median nerve | Carpal tunnel release at time of synovectomy |
| Spread to adjacent structures | Delayed diagnosis, inadequate debridement | Early diagnosis, thorough surgical debridement |
| Joint destruction | Chronic septic arthritis | Early treatment, surgical intervention |
| Drug toxicity | Prolonged multi-drug therapy | Monitor LFTs (rifampicin), visual acuity (ethambutol), hearing (aminoglycosides) |
| Chronic sinus tract | Inadequate debridement, resistant organism | Radical debridement, revision surgery |
If tenosynovitis is misdiagnosed as De Quervain's or trigger finger and treated with corticosteroid injection, NTM infection may spread dramatically. Steroids suppress local immunity and allow uncontrolled bacterial proliferation. Always consider infection in atypical presentations before injecting steroids.
Controversies & Areas of Uncertainty
No randomised trials define duration for musculoskeletal NTM. Practice ranges from "1-2 months beyond clinical resolution" (skin-limited M. marinum, roughly 3-4 months total) to 6-12+ months for tenosynovial/osseous disease. Most regimens are extrapolated from pulmonary guidelines and expert opinion rather than dedicated bone/joint evidence.
Whether all rice-body tenosynovitis needs synovectomy, or whether early-recognised superficial M. marinum can be cured medically, is debated. Aubry's series cured 52% without surgery, but deep extension reliably predicts failure. The threshold for, and extent of, debridement is individualised.
Clarithromycin is the "cornerstone," yet inducible erm(41) resistance makes it unreliable for true M. abscessus despite favourable in-vitro MICs. How heavily to weight (and how routinely to test) inducible resistance, and the role of newer agents (e.g. amikacin liposome inhalation, clofazimine, tedizolid, bedaquiline), remains unsettled.
Because AFB culture takes 2-6 weeks, clinicians must decide whether to start empiric multidrug therapy on clinical/histological suspicion or wait for confirmation. Premature single-agent or steroid use can worsen disease and obscure diagnosis; over-eager empiric therapy risks toxicity and culture suppression.
Evidence Base
Sixty-Three Cases of M. marinum Infection (Landmark Series)
- National French survey of 63 culture-confirmed M. marinum infections (1996-1998)
- Fish-tank exposure in 53 of 63 patients (84%); upper limb involved in 60 (95%)
- Infection spread to deeper structures (tendon/joint/bone) in 18 patients (29%)
- Cure achieved in 55 patients (87%); median antibiotic duration 3.5 months; surgery in 48%
- Failure related to deep-structure involvement, NOT to any particular antibiotic regimen; all isolates susceptible to clarithromycin, cyclines and rifampin without acquired resistance
Extrapulmonary NTM in Immunocompetent Hosts (Review)
- Prevalence of human NTM disease has risen over the past decade (true increase vs improved recognition unclear)
- Skin, soft-tissue and tenosynovial infection is a leading extrapulmonary syndrome in immunocompetent people
- Pathogenic isolates can be indistinguishable from environmental contaminants - clinician-laboratory communication is essential
- Lack of standardised susceptibility testing and treatment guidelines exposes patients to toxic drugs and poor outcomes
- Multicentre controlled trials are needed to improve diagnosis and therapy
Rice Bodies / Loose Bodies in Mycobacterial Tenosynovitis
- Six patients with tuberculous tenosynovitis of the hand/wrist with rice bodies, millet seeds or melon seeds at surgery
- Diagnosis frequently missed; presentation interval ranged from 1 week to 2 years
- Complications included median nerve irritation (n=2), osteomyelitis (n=3) and flexor tendon rupture (n=1)
- Culture positive in 4, AFB stain/PCR positive in 1, both negative in 1 (prior pulmonary TB)
- All managed with combination chemotherapy PLUS at least one debulking tenosynovectomy; no recurrences at mean 4-year follow-up
M. abscessus vs M. massiliense - erm(41) Drives Treatment Failure
- 64 M. abscessus vs 81 M. massiliense lung-disease patients, identical clarithromycin-based regimens (cefoxitin + amikacin induction)
- Sputum conversion / durable culture-negativity: 25% with M. abscessus vs 88% with M. massiliense (P less than 0.001)
- Inducible clarithromycin resistance (MIC 32 or more) in ALL tested M. abscessus isolates (19/19) and NONE of M. massiliense (0/28)
- Functional erm(41) gene in M. abscessus sensu stricto explains macrolide failure despite in-vitro susceptibility
- Subspecies identification therefore predicts outcome and must guide therapy
Fish-Tank M. marinum - Treatment Duration and Prevention
- Eight patients with soft-tissue M. marinum; all had cutaneous fish-tank exposure and 7 had sporotrichoid lesions
- Six skin-limited cases cured with 2-drug combinations (clarithromycin, ethambutol, rifampin)
- Recommended treatment: 2 drugs continued for 1-2 months after lesions resolve - typically 3-4 months total
- Deeper (tenosynovial/osseous) infection may need longer therapy plus surgical debridement
- Positive tuberculin skin reactions (10 mm or more in all 7 tested) may reflect M. marinum infection
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old aquarium shop owner presents with 3 months of progressive swelling and stiffness of the right index and middle fingers. He has difficulty making a fist. Previous treatment with oral flucloxacillin and then augmentin for 'infection' showed no improvement. Routine bacterial cultures have been negative. Examination shows swelling along the flexor tendons of digits 2-3 extending to the palm, reduced AROM, and positive Tinel's over the carpal tunnel. How would you approach this case?”
“A 58-year-old woman with type 2 diabetes had knee arthroscopy for degenerative meniscal tear 6 weeks ago. She now presents with persistent wound discharge from the portal sites. She received two courses of oral antibiotics (cephalexin, then augmentin) from her GP with no improvement. Swabs have grown 'skin flora' only. The wounds show minimal erythema but have serous discharge. Inflammatory markers are mildly elevated (CRP 28). What are your differential diagnoses and management plan?”
“A 62-year-old man presents with 8 weeks of progressive right wrist pain and swelling. He is immunocompetent with no significant medical history. He had a cortisone injection by his GP 3 months ago for presumed 'arthritis' which gave temporary relief. Joint aspiration shows WCC 18,000 with 75% neutrophils, but Gram stain is negative and cultures show no growth at 5 days. CRP is 35. X-ray shows periarticular osteopenia. How would you proceed?”
Guidelines, Registries & Global Practice
Global Epidemiology
NTM disease incidence has risen worldwide over recent decades, attributed to genuine increase, improved molecular recognition, an ageing population and expanding use of immunosuppressive/biologic therapy. NTM are environmental (soil and water) organisms; there is no human-to-human transmission and no isolation requirement (unlike M. tuberculosis). Species distribution is geographically patterned:
- MAC dominates slow-grower disease in North America, Western Europe and East Asia.
- M. kansasii clusters around specific urban/industrial water supplies (historically central USA, UK, parts of Europe and mining regions).
- M. abscessus and other rapid growers are proportionally more common in East/Southeast Asia and are the leading healthcare-associated NTM globally.
- M. ulcerans (Buruli ulcer) is endemic in West/Central Africa, coastal south-eastern Australia and parts of South America and the Western Pacific - consider it in any traveller or resident from an endemic zone with a painless, progressive skin ulcer.
Side-by-Side Guideline Comparison
| Body / Guideline | Scope & Emphasis | Key Recommendation |
|---|---|---|
| ATS/ERS/ESCMID/IDSA (2020, Daley) | International, GRADE-based; primarily pulmonary | Subspecies + susceptibility-guided multidrug therapy; macrolide-susceptibility (erm(41)) testing mandatory for M. abscessus; treat MAC at least 12 months after culture conversion |
| ATS/IDSA (2007, Griffith) | Foundational statement covering skin/soft-tissue and bone NTM | Defines diagnostic criteria and species-specific regimens; never monotherapy; surgery for localized/implant disease |
| WHO (Buruli ulcer / M. ulcerans) | Endemic tropical and sub-tropical regions | Rifampicin + clarithromycin for 8 weeks (oral, replacing older injectable streptomycin); surgery for large/complicated lesions |
| British / European ID & hand-surgery practice | Extrapulmonary, hand and wrist NTM | Excise rice bodies + tenosynovectomy with prolonged combination antibiotics; clarithromycin-based for M. marinum 3-6 months, longer for deep disease |
There is broad cross-society consensus on the fundamentals: confirm the species, test susceptibility (especially inducible macrolide resistance in rapid growers), never use monotherapy, combine prolonged multidrug antibiotics with surgical debridement, and continue treatment well beyond clinical or microbiological resolution. Genuine differences are mostly in pulmonary regimen detail rather than musculoskeletal management.
Laboratory and Registry Notes
- NTM is not a notifiable disease in most jurisdictions (in contrast to TB), so true incidence is under-captured and surveillance relies on voluntary laboratory reporting and national reference-laboratory networks.
- Definitive species/subspecies identification and susceptibility testing are concentrated in reference laboratories worldwide (e.g. national mycobacterial reference centres in the UK, France, Germany, USA, Korea, Australia). Always flag clinical suspicion - including the need for 30-32°C incubation when M. marinum is suspected.
- There is no dedicated implant/arthroplasty-style registry for NTM; the evidence base is case series, reference-laboratory cohorts and the society guidelines above.
High- vs Limited-Resource Practice Variation
- High-resource settings: molecular species/subspecies identification (line-probe assays, 16S/hsp65 sequencing, MALDI-TOF), erm(41) testing, drug-level monitoring, outpatient/home IV therapy and multidisciplinary ID input enable tailored, susceptibility-guided regimens.
- Limited-resource settings: prolonged AFB culture and molecular testing may be unavailable, so diagnosis leans on clinical pattern plus granulomatous histology, and empiric clarithromycin-based combinations are common. For Buruli ulcer, WHO-endorsed oral rifampicin + clarithromycin has shifted care from inpatient injectable regimens and extensive surgery toward community-based oral therapy, markedly improving access in endemic regions.
When to Suspect NTM
- Chronic indolent tenosynovitis/arthritis not responding to standard antibiotics
- Culture-negative infection with granulomatous histology
- Aquarium, fish, or water exposure + hand/wrist infection
- Rice bodies found at surgery
- Post-surgical wound infection 3-6 weeks after procedure (rapid growers)
- Immunocompromised host with atypical presentation
Key Organisms and Associations
- M. marinum: Aquarium, fish tank, swimming pool - hand tenosynovitis, sporotrichoid spread
- MAC: Disseminated in AIDS (CD4 less than 50), pulmonary in elderly
- M. kansasii: TB-like, responds to rifampicin-based regimens
- M. fortuitum: Post-surgical wounds, most susceptible rapid grower
- M. chelonae: Post-injection abscess, aminoglycoside-resistant
- M. abscessus: Post-surgical, most resistant, inducible macrolide resistance
Diagnosis Essentials
- AFB culture takes 2-6 weeks - must specifically request
- M. marinum requires 30-32C incubation (not 37C)
- AFB smear often negative (low organism burden)
- Histology: granulomas with or without caseation
- PCR for rapid species identification if available
- Multiple tissue samples (4-6) increase yield
Treatment Principles
- NEVER monotherapy - always multi-drug regimens
- Clarithromycin is cornerstone of most regimens
- Surgical debridement usually required
- Duration: 3-6 months skin/soft tissue, 6-12+ months bone/joint
- Susceptibility testing guides therapy especially for rapid growers
- Monitor toxicity: LFTs (rifampicin), vision (ethambutol), hearing (aminoglycosides)
M. marinum Specifics
- Classic: aquarium exposure + chronic hand tenosynovitis + negative routine cultures
- Incubation 2-4 weeks (up to 9 months)
- Optimal growth at 30-32C - specify on culture request
- Treatment: clarithromycin + rifampicin for 3-6 months
- Tenosynovectomy + carpal tunnel release if CTS
- Continue treatment 1-2 months after clinical resolution
Viva Red Flags
- Steroid injection for presumed inflammatory tenosynovitis - will worsen NTM
- Stopping antibiotics early based on symptom improvement
- Not requesting AFB culture specifically
- Using single-agent therapy
- Missing inducible macrolide resistance in M. abscessus
- Forgetting surgical debridement is usually required
References
-
Aubry A, Chosidow O, Caumes E, et al. Sixty-three cases of Mycobacterium marinum infection: clinical features, treatment, and antibiotic susceptibility of causative isolates. Arch Intern Med. 2002;162(15):1746-52. PMID 12153378.
-
Piersimoni C, Scarparo C. Extrapulmonary infections associated with nontuberculous mycobacteria in immunocompetent persons. Emerg Infect Dis. 2009;15(9):1351-8. PMID 19788801.
-
Daley CL, Iaccarino JM, Lange C, et al. Treatment of nontuberculous mycobacterial pulmonary disease: an official ATS/ERS/ESCMID/IDSA clinical practice guideline. Eur Respir J. 2020;56(1):2000535. PMID 32636299. (Co-published Clin Infect Dis. 2020;71(4):905-913. PMID 32797222.)
-
Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416. PMID 17277290.
-
Lewis FM, Marsh BJ, von Reyn CF. Fish tank exposure and cutaneous infections due to Mycobacterium marinum: tuberculin skin testing, treatment, and prevention. Clin Infect Dis. 2003;37(3):390-7. PMID 12884164.
-
Koh WJ, Jeon K, Lee NY, et al. Clinical significance of differentiation of Mycobacterium massiliense from Mycobacterium abscessus. Am J Respir Crit Care Med. 2011;183(3):405-10. PMID 20833823.
-
Woon CY, Phoon ES, Lee JY, et al. Rice bodies, millet seeds, and melon seeds in tuberculous tenosynovitis of the hand and wrist. Ann Plast Surg. 2011;66(6):610-7. PMID 20948407.