Patient Blood Management
- Spine surgery - particularly DEFORMITY (scoliosis) correction, multilevel fusion and revision - causes substantial blood loss because of large exposures, bleeding from cancellous (decorticated/osteotomised) bone, long operative times, and the EPIDURAL VENOUS PLEXUS, and it has the HIGHEST blood-transfusion rate among the major orthopaedic procedures (reported around 15%, versus a few percent for hip/knee arthroplasty).
- The modern approach is PATIENT BLOOD MANAGEMENT (PBM) - a MULTIMODAL, multidisciplinary bundle applied across the preoperative, intraoperative and postoperative phases - because no single measure suffices and the goal is to minimise both blood loss and the need for (and risks of) allogeneic transfusion.
- PREOPERATIVELY, the key modifiable factor is ANAEMIA: a low preoperative haemoglobin is the strongest independent predictor of transfusion, so iron-deficiency/anaemia should be identified and treated (oral or intravenous iron, with erythropoiesis-stimulating agents in selected cases) before major elective spine surgery, and antiplatelet/anticoagulant agents managed appropriately.
- INTRAOPERATIVELY, TRANEXAMIC ACID (an antifibrinolytic) is the cornerstone pharmacological measure - it significantly reduces intraoperative bleeding, cell-saver volume and operative time (with higher weight-based dosing more effective in adolescent deformity surgery) and is not associated with a clear increase in complications; the ABSENCE of TXA is itself an independent predictor of transfusion.
- Other INTRAOPERATIVE measures are PRONE POSITIONING with a FREE ABDOMEN (using a Wilson frame/Jackson table/chest rolls to keep the abdomen hanging free), which lowers intra-abdominal/caval pressure and reduces epidural venous engorgement and bleeding; controlled HYPOTENSIVE anaesthesia; meticulous surgical HAEMOSTASIS (bipolar, bone wax, topical haemostatic agents); intra-operative CELL SALVAGE for high-volume cases; and STAGING very large reconstructions.
- POSTOPERATIVELY, a RESTRICTIVE transfusion strategy (transfusing for symptomatic anaemia or a lower haemoglobin threshold rather than liberally) is used, with continued iron and monitoring; the overall PBM bundle reduces transfusion exposure and its risks, and risk stratification (low preoperative haemoglobin, high-risk procedure, ASA III-IV, no TXA, older age) identifies patients who most need these measures.
- “Spine (deformity/revision) surgery = HIGH blood loss + the HIGHEST transfusion rate in ortho (~15%); epidural venous plexus + cancellous bleeding.
- “TRANEXAMIC ACID is the cornerstone agent (reduces bleeding/cell-saver volume/op time; higher weight-based dose more effective in deformity); absence of TXA predicts transfusion.
- “Multimodal PBM: preop anaemia/iron optimisation; intraop TXA + free-abdomen prone positioning + hypotensive anaesthesia + cell salvage + staging; postop restrictive transfusion.
Large exposures, cancellous bleeding, long cases and the epidural venous plexus - spine (deformity) surgery has the highest transfusion rate in orthopaedics (~15%).
PBM: optimise anaemia/iron preop; TXA + free-abdomen prone positioning + cell salvage intraop; restrictive transfusion postop.
Why Spine Bleeds & the Multimodal Bundle
Spine surgery - especially deformity correction, multilevel fusion and revision - bleeds heavily because of large exposures, bleeding cancellous bone, long operative times and the epidural venous plexus, and it has the highest transfusion rate of the major orthopaedic procedures (around 15%). The answer is patient blood management (PBM), a multimodal bundle: preoperatively optimise anaemia (treat iron-deficiency, a low preoperative haemoglobin is the strongest transfusion predictor) and manage anticoagulants; intraoperatively use tranexamic acid (the cornerstone antifibrinolytic), prone positioning with a free abdomen (to reduce epidural venous engorgement), controlled hypotensive anaesthesia, meticulous haemostasis, cell salvage for high-volume cases, and staging very large reconstructions; and postoperatively transfuse restrictively. No single measure suffices.
- Measures
- Identify/treat anaemia (iron +/- ESA); manage antiplatelet/anticoagulant; autologous planning
- Goal
- Raise the starting haemoglobin; reduce transfusion need
- Measures
- Tranexamic acid (antifibrinolytic; higher weight-based dose in deformity)
- Goal
- Reduce bleeding, cell-saver volume, operative time
- Measures
- Free-abdomen prone positioning; hypotensive anaesthesia; meticulous haemostasis; cell salvage; staging
- Goal
- Reduce venous engorgement and surgical blood loss; recycle red cells
- Measures
- Restrictive transfusion thresholds; continue iron; monitor
- Goal
- Limit allogeneic transfusion and its risks
Tranexamic Acid & Positioning
- Tranexamic acid (TXA): the cornerstone agent - an antifibrinolytic that reduces intraoperative bleeding, cell-saver volume and operative time; in adolescent deformity surgery, higher weight-based dosing is more effective, without a clear increase in complications. The absence of TXA is an independent predictor of transfusion.
- Free-abdomen prone positioning: position prone on a frame/table (Wilson frame, Jackson table, chest rolls) so the abdomen hangs free, lowering intra-abdominal and caval pressure and reducing epidural venous engorgement and bleeding - a simple, powerful technical measure.
- Supporting measures: controlled hypotensive anaesthesia (within safe limits for cord perfusion), meticulous haemostasis, intra-operative cell salvage for high-volume cases, and staging very large cases.
- Risk-stratify: low preoperative haemoglobin, a high-risk procedure, ASA III-IV, no TXA and older age all raise transfusion risk - target the bundle at those patients.
Three measures carry most of the benefit and should not be omitted. First, OPTIMISE PREOPERATIVE ANAEMIA: a low preoperative haemoglobin is the strongest independent predictor of transfusion, so elective major spine surgery should not proceed without identifying and treating iron-deficiency anaemia. Second, give TRANEXAMIC ACID: it is the cornerstone antifibrinolytic, reduces bleeding and cell-saver volume, and its absence independently predicts transfusion. Third, POSITION PRONE WITH A FREE ABDOMEN, because a compressed abdomen raises caval pressure and engorges the epidural venous plexus, increasing bleeding. Combine these with cell salvage, controlled hypotension (kept safe for spinal cord perfusion) and a restrictive postoperative transfusion threshold, and risk-stratify so the most vulnerable patients receive the fullest bundle.
Hypotension vs Cord Perfusion: The Spine-Specific Tension
- Why hypotension helps the field: lowering the mean arterial pressure (MAP) reduces capillary and venous oozing and gives a drier field, which is why controlled hypotension is a recognised blood-loss measure (general technique in our General Anaesthesia topic).
- Why it is dangerous in spine: spinal cord perfusion pressure = MAP minus the local CSF/venous pressure, so a low MAP directly reduces cord perfusion - and during deformity correction the cord is simultaneously stressed by distraction/correction, so profound hypotension risks cord ischaemia and iatrogenic spinal cord injury (cord blood supply detailed in our Spinal Cord Blood Supply topic).
- The compromise: use only mild/moderate hypotension (if any) during exposure, avoid profound hypotension, and maintain or actively raise the MAP (e.g. toward around 80 mmHg or higher) during and after the correction manoeuvre and whenever neuromonitoring (SSEP/MEP) signals deteriorate - cord protection overrides the bleeding goal. This is exactly why intra-operative neuromonitoring guides the pressure (see our Spinal Cord Monitoring topic), and why patients with poor cord vascular reserve should not be run hypotensive.
Controlled hypotension dries the field, but spinal cord perfusion pressure = MAP minus CSF/venous pressure, so in deformity surgery avoid profound hypotension and raise the MAP during/after correction and on any neuromonitoring change - cord protection beats blood conservation. Hypotension is the measure you abandon first when the cord is at risk.
Why Freeing the Abdomen Works: The Batson Plexus
- The anatomy: the internal vertebral (epidural) venous plexus is part of the vertebral venous plexus of Batson - a valveless network in the epidural space that communicates freely with the inferior vena cava, azygos and pelvic venous systems, so pressure is transmitted bidirectionally with no valves to buffer it.
- The mechanism of bleeding: when the patient is prone, a compressed abdomen raises intra-abdominal and IVC pressure; because the plexus is valveless and caval-connected, this pressure is transmitted straight into the epidural veins, which engorge and bleed briskly in the surgical field (and divert venous return through the plexus).
- The fix: position prone on a Wilson frame, Jackson/open-frame table or chest-and-pelvis bolsters so the abdomen hangs free - this drops IVC and intra-abdominal pressure, decompresses the epidural plexus and reduces bleeding (and lowers airway pressures too). It is one of the simplest, highest-yield technical measures.
- The tension to be aware of: the Wilson frame, which frees the abdomen effectively, is also an independent risk factor for ischaemic optic neuropathy in the case-control data (see the visual-loss section below). The two facts are not contradictory - the frame is implicated largely because it is often used in a head-down attitude, which raises venous pressure in the head. The resolution is to keep the abdomen free and the head neutral, at or above the level of the heart, rather than to abandon the frame.
- Aside: the same valveless Batson plexus is the route by which pelvic/abdominal tumour and infection spread haematogenously to the spine - the anatomy that drives the bleeding is also the metastatic highway.
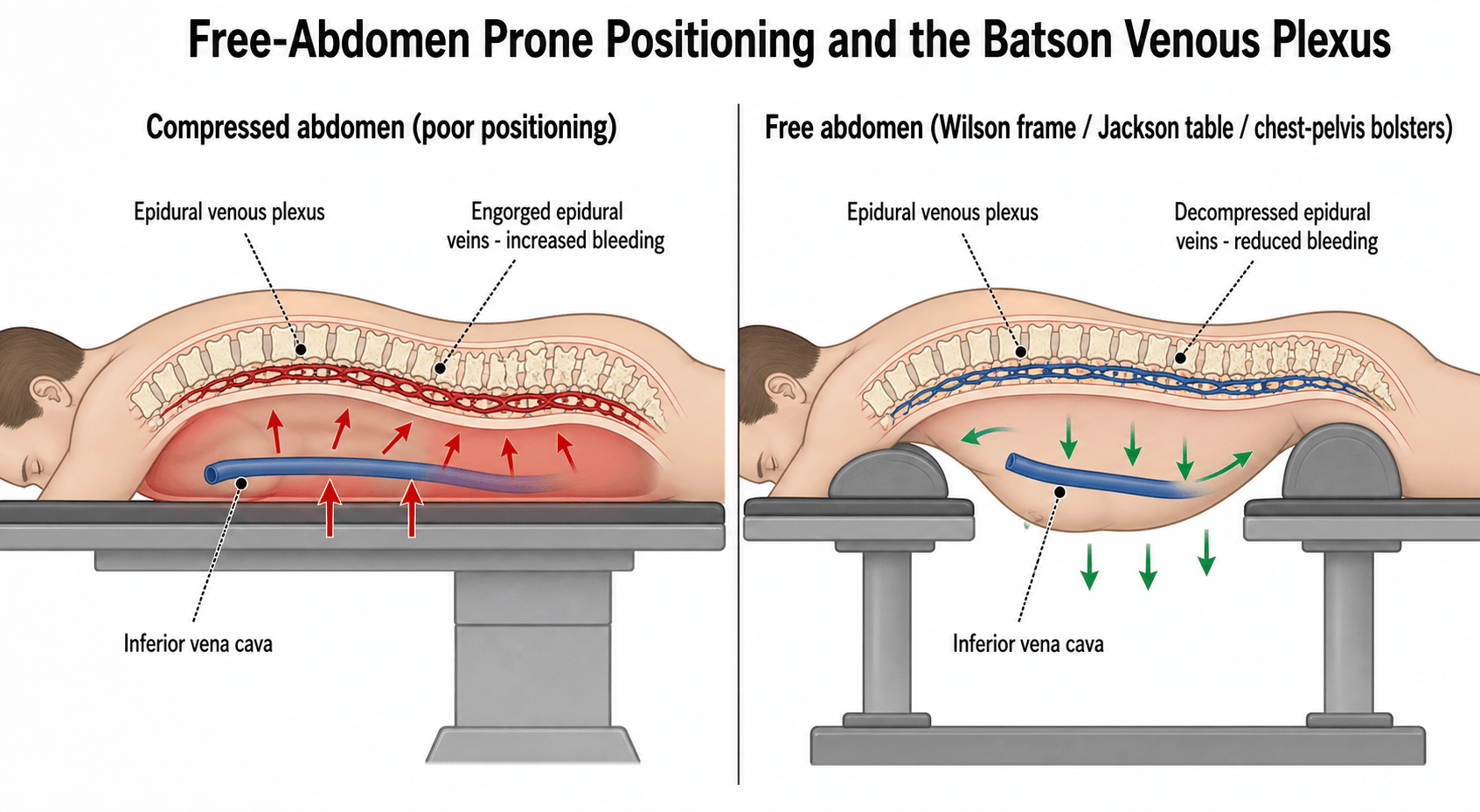
The epidural veins are part of the valveless vertebral venous plexus of Batson, freely connected to the IVC - so a compressed prone abdomen raises caval pressure and engorges them, causing brisk bleeding. Freeing the abdomen (Wilson/Jackson frame, bolsters) decompresses the plexus and cuts blood loss. (The same valveless plexus is the route of spinal metastasis.)
Perioperative Visual Loss: The Complication That Justifies the Whole Bundle
The reason blood loss in prone spine surgery is treated so seriously is not transfusion cost - it is perioperative visual loss (POVL), a rare but devastating and usually irreversible complication that sits at the intersection of blood loss, prone positioning and hypotension.
- The mechanism is usually ischaemic optic neuropathy (ION), not a corneal or retinal problem. Posterior ION - infarction of the retrobulbar optic nerve, which has no collateral supply - is the pattern classically reported after prolonged prone spinal fusion. Central retinal artery occlusion from direct globe pressure is a separate, positioning-specific mechanism and is the one that is genuinely preventable by checking the eyes are free.
- The recognised risk factors from the largest case-control work are male sex, obesity, use of the Wilson frame, longer operative time, greater blood loss, and a lower colloid-to-crystalloid ratio in non-blood fluid replacement. Add the patient factors that compound them: pre-operative anaemia, intra-operative hypotension, diabetes, hypertension and a small cup-to-disc ratio.
- Recognition. Painless visual loss, often noticed on waking, with an afferent pupillary defect. The fundus may look normal in posterior ION, which is why a normal fundoscopy does not exclude it. Urgent ophthalmology involvement is mandatory, but no treatment is reliably effective - which is precisely why the emphasis is on prevention.
- What prevention actually means here. It is the same bundle: keep the operation short, keep blood loss down, avoid prolonged deliberate hypotension, correct anaemia beforehand, use colloid as well as crystalloid in replacement, stage very long deformity procedures where feasible, and position with the head neutral and at or above the level of the heart with the globes demonstrably free of pressure.
- Consent. In prolonged prone deformity surgery with anticipated major blood loss, visual loss is a recognised risk that should be discussed pre-operatively rather than explained afterwards.
Coagulopathy in the Long Construct
Major deformity surgery loses blood over hours rather than in a single event, and the bleeding changes character as it goes on.
- Dilutional coagulopathy develops as red cells and crystalloid replace whole blood without replacing clotting factors or platelets. The surgical field stops producing discrete bleeding points and starts oozing diffusely from raw cancellous bone and muscle - a change worth recognising as a laboratory event, not a technical one, because more diathermy will not fix it.
- Fibrinogen falls first. It is the earliest factor to reach a critical level in dilutional coagulopathy, and it is the one most often overlooked while attention is on platelets and INR.
- Hypothermia and acidosis compound it, both by impairing enzyme function - which is why active warming is a haemostatic measure and not merely a comfort one.
- Monitor rather than guess. Serial full blood count, coagulation screen and fibrinogen, with viscoelastic testing (TEG/ROTEM) where available, allow targeted replacement instead of formulaic ratios.
- Anticipate it in the highest-loss operations - three-column osteotomies (pedicle subtraction osteotomy, vertebral column resection), long multilevel constructs, revision surgery through scar, and tumour resection - and plan cross-matching, cell salvage and blood-product availability before starting rather than during the bleed. (The osteotomies themselves are developed in our Three-Column Osteotomies topic.)
Mnemonics & Memory Aids
BLOOD
Hook:BLOOD: Bundle (PBM), Low Hb optimise, Offer TXA, Open (free) abdomen prone, Diminish need (cell salvage/hypotension/restrictive).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How would you minimise blood loss and transfusion in a major deformity spine operation?”
“What is tranexamic acid and what is the evidence in spine surgery?”
Why spine bleeds
- Large exposures, cancellous bone bleeding, long operative times, epidural venous plexus
- Highest transfusion rate in ortho (~15%; vs ~3-4% hip/knee)
- Deformity, multilevel and revision surgery the highest risk
Preoperative
- Identify/treat anaemia (iron +/- ESA) - low Hb is the strongest predictor
- Manage antiplatelet/anticoagulant agents
- Risk-stratify (Hb, procedure, ASA, age)
Intraoperative
- Tranexamic acid (cornerstone; higher weight-based dose in deformity)
- Free-abdomen prone positioning (reduce epidural venous engorgement)
- Hypotensive anaesthesia (safe for cord), haemostasis, cell salvage, staging
Postoperative
- Restrictive transfusion threshold (symptomatic/low Hb)
- Continue iron; monitor
- Patient blood management reduces transfusion exposure and risk
Evidence & Key Studies
Optimal tranexamic acid dosing for adolescent idiopathic scoliosis surgery (network meta-analysis)
- Tranexamic acid is an antifibrinolytic widely used in spine surgery; in AIS instrumentation, higher weight-based dosing (a 100 mg/kg bolus plus 10 mg/kg/hr infusion) was most effective at reducing intraoperative bleeding, operative time and cell-saver volume.
- Lower doses also helped but less so; there was no difference in complication rates between doses (though not uniformly reported).
- TXA dosing meaningfully affects blood loss in adolescent deformity surgery (network meta-analysis of 1,523 patients across 16 studies).
Independent preoperative predictors of red-cell transfusion in major orthopaedic surgery
- Spine surgery had the highest transfusion rate among major orthopaedic procedures (15%, versus 3.6% hip and 2.7% knee) in a cohort of 7,072 patients.
- Independent predictors of transfusion included low preoperative haemoglobin (under 13 g/dL; relative risk 6.55), high-risk procedure (RR 7.40), ASA III-IV (RR 2.00), ABSENCE of tranexamic acid (RR 2.52) and older age.
- These findings support patient blood management strategies (anaemia optimisation and routine TXA) to reduce transfusion.
The role and dosing of tranexamic acid in adolescent deformity surgery (higher weight-based dosing most effective, without a clear increase in complications) come from the cited Lajczak network meta-analysis; the highest-in-orthopaedics spine transfusion rate (about 15%) and the independent transfusion predictors (low preoperative haemoglobin, high-risk procedure, ASA III-IV, absence of TXA, older age) from the cited Ortiz-Gomez cohort. The broader patient-blood-management bundle - preoperative anaemia/iron optimisation, free-abdomen prone positioning to reduce epidural venous engorgement, hypotensive anaesthesia, cell salvage, staging and restrictive postoperative transfusion - is standard, well-established teaching. (See also our Adolescent Idiopathic Scoliosis and Adult Spinal Deformity topics.)