Progressive Varus Deformity of Childhood | Physeal Growth Suppression | Medial Tibial Plateau Depression
- Blount disease is a disorder of the medial proximal tibial physis with secondary varus, internal torsion, and depression of the medial tibial plateau
- The metaphyseal-diaphyseal angle (MDA) of Levine and Drennan greater than 11° strongly predicts Blount disease and helps distinguish it from physiological varus
- Infantile disease is typically bilateral and symmetric; adolescent disease is more often unilateral and associated with obesity
- Langenskiold stages I and II in children under 3 may respond to knee-ankle-foot orthosis (KAFO) bracing; stages III and above require surgery
- Modern treatment favours guided growth (lateral tension-band plating) in mild-to-moderate adolescent deformity, with high tibial valgus osteotomy reserved for severe or end-stage disease
- “Physiological genu varum resolves by age 2-3; persistent or progressive varus after age 3 should raise suspicion for Blount disease
- “Langenskiold stage VI is the end-stage physeal bar pattern; the medial physis is essentially closed and requires complex reconstruction
- “Guided growth is contraindicated in end-stage physeal arrest (Langenskiold V-VI) because remaining growth is insufficient to correct the deformity
- “Bowing in Blount disease is sharply angulated at the proximal tibia, whereas physiological varum is a smooth bow throughout the limb
Medial proximal tibial physis is suppressed, leading to a triangular epiphysis, varus deformity, internal tibial torsion, and progressive depression of the medial tibial plateau.
Levine and Drennan angle greater than 11° indicates Blount disease. The angle is formed by a line through the medial and lateral tibial metaphyseal beaks and a line perpendicular to the long axis of the tibial diaphysis.
Six radiographic stages (I-VI) progress from irregularity of the medial physis with beaking (I) to medial physeal bar formation and epiphyseal depression (VI). Each stage worsens prognosis.
Stage I-II in children under 3 may respond to a knee-ankle-foot orthosis worn for 1-2 years. Stage III and above, or older children, require surgery (high tibial valgus osteotomy or guided growth).
- Key Diagnostic Feature
- MDA greater than 11°, no physeal bar
- Primary Treatment
- KAFO bracing, full-time, 1-2 years
- Key Pearl
- 70-90% success if started under age 3
- Key Diagnostic Feature
- Medial plateau step, physeal bar
- Primary Treatment
- Valgus high tibial osteotomy
- Key Pearl
- Overcorrection to 5-10° valgus reduces recurrence
- Key Diagnostic Feature
- Open physis, mechanical axis medial
- Primary Treatment
- Lateral tension-band (8-plate) hemiepiphysiodesis
- Key Pearl
- Reversible, favoured in patients with growth remaining
- Key Diagnostic Feature
- Mechanical axis zone III, physeal closure
- Primary Treatment
- Valgus tibial osteotomy ± hemiepiphysiodesis of contralateral side
- Key Pearl
- External fixation or plate fixation both acceptable
BLOUNTBLOUNT Mnemonic - Features of the Disease
Hook:BLOUNT = Bowing, Lateral thrust, Obesity, Unloading, No resolution, Torsion - six features of Blount disease.
STAGESLangenskiold Stages I to VI
Hook:STAGES walks you from Sloping physis to Stopped physis - the natural history of untreated Blount.
SURGERYIndications for Surgery in Blount Disease
Hook:SURGERY - seven triggers for surgical referral in Blount disease.
Overview and Epidemiology
Blount disease is a growth disorder of the medial proximal tibial physis that produces a sharply angulated tibia vara with internal torsion, lateral thrust, and progressive deformity. It must be distinguished from physiological genu varum of infancy, which is a smooth, symmetric, age-appropriate bow that resolves spontaneously. Missing the distinction leads either to unnecessary surgery in physiological varus or to delayed treatment and permanent deformity in Blount disease.
- Infantile form: onset 1-4 years, often bilateral, common in children of African descent, strong link with early walking and obesity
- Adolescent form: onset over 8-10 years, often unilateral, often male, marked obesity
- Risk factors: obesity (body mass index greater than 95th percentile), early ambulation (under 11 months), and family history in some series
- Geographic variation: higher incidence in populations with higher childhood obesity and earlier walking age
- Progressive deformity: varus worsens with growth if untreated
- Lateral thrust: dynamic knee instability in stance phase
- Limb-length discrepancy: may develop, especially in unilateral cases
- Premature medial compartment osteoarthritis: long-term sequelae of untreated disease
Pathophysiology
The medial proximal tibial physis is exposed to abnormal compressive load during weight-bearing in early childhood. Genetic, mechanical, and developmental factors combine to suppress the medial physis while the lateral physis continues to grow. The result is a triangular medial epiphysis, a beaked medial metaphysis, a depressed medial tibial plateau, and a varus angulation of the tibia accompanied by internal tibial torsion. The disease is progressive and does not self-correct, in contrast to physiological varum.
- Blount Disease
- Sharp, angulated at proximal tibia
- Physiological Genu Varum
- Smooth bow throughout femur and tibia
- Blount Disease
- Infant under 4 years or adolescent over 8 years
- Physiological Genu Varum
- Infant 6 months to 2 years
- Blount Disease
- Progressive; does not resolve
- Physiological Genu Varum
- Self-correcting by age 2-3 years
- Blount Disease
- Beaking, irregularity, possible bar (Langenskiold)
- Physiological Genu Varum
- Normal physis, no beaking
- Blount Disease
- Greater than 11° (Blount)
- Physiological Genu Varum
- Less than 11° (physiological)
- Blount Disease
- Infantile: often bilateral; adolescent: often unilateral
- Physiological Genu Varum
- Bilateral and symmetric
Heuter-Volkmann principle: increased compressive load suppresses physeal growth
Hueter-Volkmann mechanism drives the medial proximal tibia in Blount disease
Compressive overload on the medial physis reduces chondrocyte proliferation
Asymmetric growth produces a triangular epiphysis and varus angulation
Varus increases medial load - a positive-feedback loop of progressive deformity
Infantile: physis is highly susceptible to compression; obesity + early walking trigger suppression; often bilateral
Juvenile (4-8 years): rare overlap group with mixed features
Adolescent: physis is more resistant; deformity only manifests after years of mechanical overload; typically obese adolescents with unilateral varus
Late-onset form has less severe radiographic change at presentation but a narrower growth window for correction
Classification and Types
Classification by Age of Onset
- Age of Onset
- 1-4 years (peak 2-4)
- Laterality
- Often bilateral
- Severity at Presentation
- Langenskiold I-VI, severe
- Treatment Approach
- Brace first; osteotomy if advanced
- Age of Onset
- 4-10 years
- Laterality
- Variable
- Severity at Presentation
- Intermediate
- Treatment Approach
- High tibial osteotomy or guided growth
- Age of Onset
- Over 8-10 years, often near skeletal maturity
- Laterality
- Often unilateral
- Severity at Presentation
- Langenskiold II-IV, less severe
- Treatment Approach
- Lateral hemiepiphysiodesis primary
The age of onset is the strongest predictor of treatment choice and prognosis.
Clinical Assessment
- Age of onset: infantile (1-4 years) versus adolescent (over 8 years)
- Walking age: walked before 11 months is a risk factor
- Body habitus: obesity is a major risk factor in both forms
- Family history: rare familial cases have been described
- Progression: deformity has worsened rather than improved with growth
- Pain: usually absent in infantile form; knee or medial joint line pain in adolescent form
- Gait: lateral thrust in stance phase, often with intoeing
- Standing alignment: tibia vara, often with internal tibial torsion
- Intercondylar (knee) distance: increased in standing, reduced on lying
- Range of motion: usually full; flexion contracture is rare
- Limb length: check for discrepancy in unilateral cases
- Body mass index: record and plot on growth chart
Physiological genu varum is symmetric, smooth, and resolves by age 2-3. Blount disease is sharply angulated at the proximal tibia, often unilateral (in adolescent form) or asymmetric, and is associated with lateral thrust on stance. Standing full-length AP radiographs showing a metaphyseal-diaphyseal angle greater than 11° and a beaked medial metaphysis confirm Blount disease. A child with persistent or progressive varus after age 3 should be referred to a paediatric orthopaedic surgeon.
- Blount Disease
- Worsens
- Physiological Genu Varum
- Resolves
- Blount Disease
- Sharply angulated at proximal tibia
- Physiological Genu Varum
- Smooth, gradual
- Blount Disease
- Greater than 11° (often greater than 16°)
- Physiological Genu Varum
- Less than 11°
- Blount Disease
- Present
- Physiological Genu Varum
- Absent
- Blount Disease
- Common
- Physiological Genu Varum
- Absent
- Blount Disease
- Common in both infantile and adolescent forms
- Physiological Genu Varum
- Variable
A simple bedside clue is the apex of the deformity. In Blount disease, run a straight edge along the lateral border of the tibia - the apex of angulation is at the proximal tibia. In physiological varum, the limb bows smoothly with no single focal apex. This single test, combined with the metaphyseal-diaphyseal angle on a standing radiograph, reliably separates the two diagnoses in a 3-year-old.
The discrimination above is Blount versus physiological varum, but a child with pathological tibia vara has a wider differential that an examiner will probe - especially when the varus is atypical, the metaphyseal changes are at multiple sites, or the child is unusually short:
- Rickets (nutritional or hypophosphataemic): bilateral, symmetric varus (or valgus) with widened, frayed, cupped physes at multiple sites (wrists, knees, ankles), not just the medial proximal tibia. Trigger a metabolic screen - calcium, phosphate, alkaline phosphatase, vitamin D, PTH, renal function - whenever the radiographic changes are generalised rather than focal to the medial proximal tibia.
- Skeletal dysplasia (achondroplasia, metaphyseal chondrodysplasia, others): disproportionate short stature, multi-level metaphyseal change, family history - varus is one feature of a generalised bone disorder.
- Focal fibrocartilaginous dysplasia (FFCD): a key Blount mimic - an abrupt medial proximal tibial varus with a radiolucent cortical defect/sclerotic margin at the pes anserinus insertion, but it characteristically resolves spontaneously, so recognising it avoids unnecessary osteotomy.
- Post-traumatic or post-infective medial physeal arrest: a unilateral varus from a previous Salter-Harris injury or osteomyelitis - history and a focal bony bar distinguish it.
Exam point: before labelling tibia vara as Blount, exclude rickets (metabolic screen + generalised physeal change), skeletal dysplasia (short stature/multilevel), focal fibrocartilaginous dysplasia (self-resolving pes-anserinus lesion), and post-traumatic/post-infective physeal arrest - Blount is a diagnosis with a differential, not a default.
Investigations
Imaging and Workup Protocol
Views: standing AP pelvis-to-ankle (long-cassette) films, patellae forward
Look for: medial metaphyseal beaking, metaphyseal-diaphyseal angle, mechanical axis deviation, joint line orientation, contralateral comparison
Threshold: MDA greater than 11° suggests Blount disease; greater than 16° is highly predictive
Indication: assess tibial tubercle position, posterior tibial slope, and any sagittal plane deformity
Look for: posterior slope of the proximal tibia, any knee flexion deformity, proximal tibial anatomy for osteotomy planning
Indication: suspected medial physeal bar, preoperative planning of complex or recurrent deformity, atypical presentation
Look for: physeal bar (Langenskiold VI), meniscal pathology, osteochondral changes of the medial femoral condyle
Modality: coronal, sagittal, and 3-D volumetric gradient-echo sequences are preferred for bar identification
Indication: limb-length discrepancy assessment in unilateral cases
Threshold: discrepancy greater than 2 cm at maturity may need epiphysiodesis of the contralateral side

The metaphyseal-diaphyseal angle of Levine and Drennan is the most useful single measurement for confirming Blount disease. The angle is formed by a line through the medial and lateral beaks of the proximal tibial metaphysis and a line perpendicular to the long axis of the tibial diaphysis. Greater than 11° is abnormal, and greater than 16° is highly specific for Blount disease. An MDA of less than 11° with symmetric, smooth bowing and no metaphyseal irregularity supports physiological varum and clinical observation.
- Indication
- All cases of suspected tibia vara
- Key Finding
- Medial beaking, MDA, mechanical axis
- Threshold or Interpretation
- MDA greater than 11° suggests Blount
- Indication
- Sagittal alignment and tubercle assessment
- Key Finding
- Posterior tibial slope, tubercle position
- Threshold or Interpretation
- Posterior slope greater than 15° suggests correction must restore slope
- Indication
- Physeal bar, atypical, or recurrent disease
- Key Finding
- Focal physeal bridge, cartilage status
- Threshold or Interpretation
- Any bar greater than 50% of physeal width usually needs resection or salvage
- Indication
- Limb-length assessment in unilateral cases
- Key Finding
- Length of femur and tibia
- Threshold or Interpretation
- Discrepancy greater than 2 cm at maturity needs epiphysiodesis or lengthening
- Indication
- Adolescent treatment planning
- Key Finding
- Remaining growth prediction
- Threshold or Interpretation
- Guided growth requires at least 12-18 months of growth remaining
Management Algorithm
The decision tables above repeatedly refer to "mechanical axis in zone I/II/III", but the zone system and the CORA principle are never defined - and they are exactly what an examiner asks when you say you would "correct the mechanical axis":
- Mechanical axis (and the malalignment test): draw the mechanical axis of the limb from the centre of the femoral head to the centre of the ankle. In a normal limb it passes just medial to the knee centre (Mikulicz line). Where it crosses the knee defines the varus severity: zone 0/1 = within the central part of the tibial plateau (mild), zone 2 = over the medial tibial spine/plateau region, zone 3 = at or beyond the medial cortex/edge of the joint (severe). Greater medial deviation (higher zone) is what tips the topic's tables from observation/guided growth toward osteotomy.
- Mechanical axis deviation (MAD) is the perpendicular distance from that axis to the knee centre - the quantitative version of the zone.
- CORA (centre of rotation of angulation): the point where the proximal and distal mechanical/anatomic axis lines intersect - i.e. the true apex of the deformity. In Blount it sits at the proximal tibial metaphysis. An osteotomy performed at the CORA corrects angulation without creating a translation (zig-zag) deformity; an osteotomy away from the CORA needs added translation to keep the axis straight.
Exam point: quantify the deformity with the mechanical axis zone (and MAD) - higher zone = more severe = stronger osteotomy indication - and plan correction at the CORA (proximal tibial apex) so the realigned limb is straight, not zig-zagged.
Infantile Blount - Bracing Protocol
Goal: correct early deformity and prevent progression to advanced Langenskiold stages
Patient selection: Langenskiold stages I-II, age under 3 years, compliant family
Knee-Ankle-Foot Orthosis Bracing Protocol
Age: under 3 years at start of bracing
Stage: Langenskiold I or II (no medial plateau step)
Body habitus: brace fit must be feasible; severe obesity reduces efficacy
Family commitment: 23 hours per day wear for 1-2 years
Standard: knee-ankle-foot orthosis (KAFO) with valgus-producing force at the knee
Mechanism: valgus moment unloads the medial physis and allows lateral growth to catch up
Wear schedule: full-time (23 hours) for the first 12 months, then night-only after clinical and radiographic correction
Frequency: every 4 months with standing radiographs
Outcome measures: MDA, mechanical axis, Langenskiold stage
If no improvement at 6-12 months: abandon brace and proceed to surgery
Best: Langenskiold I, age under 2, no medial plateau step, family compliance
Worst: Langenskiold II or above, age over 3, obesity, partial wear
Realistic success rate: 70-90% in optimal candidates, falling to 30-50% in older or stage II children
Bracing works only in the youngest patients with the earliest radiographic changes. The window of opportunity is the first 3 years of life at Langenskiold stages I and II. Once the medial plateau develops a step (stage III) or a physeal bar forms (stage VI), bracing cannot reverse the structural change. Delayed referral is the most common cause of bracing failure.
Complications
- Incidence or Risk
- 20-30%, higher in Langenskiold IV or above
- Risk Factors
- Undercorrection, advanced stage, obesity
- Management
- Repeat osteotomy or hemiepiphysiodesis of contralateral side
- Incidence or Risk
- 1-5% after opening-wedge osteotomy
- Risk Factors
- Large correction, prolonged surgery, obesity
- Management
- Emergent fasciotomy; monitor closely for 48 hours
- Incidence or Risk
- Up to 10%, usually neurapraxia
- Risk Factors
- Closing-wedge or large correction
- Management
- Expectant; recovery in 3-6 months in most cases
- Incidence or Risk
- Long-term sequela of untreated disease
- Risk Factors
- Untreated or recurrent varus into adulthood
- Management
- High tibial osteotomy in adulthood or unicompartmental knee replacement
- Incidence or Risk
- Up to 50% in unilateral disease
- Risk Factors
- Asymmetric physeal involvement, hemiepiphysiodesis
- Management
- Epiphysiodesis of contralateral side or lengthening
- Incidence or Risk
- Higher in obese adolescents
- Risk Factors
- Body mass index greater than 35, diabetes
- Management
- Meticulous soft tissue handling, possible staged closure
- Incidence or Risk
- Rare after guided growth if technique is extraperiosteal
- Risk Factors
- Improper screw placement, periosteal stripping
- Management
- Bar resection if focal, otherwise accept and plan later reconstruction
The most important complication to prevent is progressive medial compartment osteoarthritis from persistent varus. Every effort should be made to align the mechanical axis by skeletal maturity. Undercorrection of the osteotomy and failure to recognise the Langenskiold stage at presentation are the two most common causes of poor outcome. The BrACE principle (Brace early, Align mechanically, Correct over, Educate family) summarises the management philosophy.
Outcomes and Prognosis
- Patient Selection
- Langenskiold I-II, age under 3
- Expected Outcome
- 70-90% full correction in optimal candidates
- Long-Term Function
- Normal knee alignment and gait if successful
- Patient Selection
- Adolescent, open physis, mild-moderate varus
- Expected Outcome
- 80% reach neutral mechanical axis
- Long-Term Function
- Good function, low recurrence if plate removed at correct time
- Patient Selection
- Langenskiold III-VI, severe varus
- Expected Outcome
- Mechanical axis restored, 70-80% maintained at 5 years
- Long-Term Function
- Pain relief, function improved; 20-30% recurrence risk
- Patient Selection
- Focal medial bar, open physis, less than 50% physeal involvement
- Expected Outcome
- Resumption of growth in 70-80%, often with adjuvant osteotomy
- Long-Term Function
- Variable; dependent on bar size and remaining growth
- Patient Selection
- Severe multiplanar or recurrent deformity
- Expected Outcome
- Accurate gradual correction, low recurrence in experienced hands
- Long-Term Function
- Excellent mechanical axis restoration; pin-site care needed
Best prognosis: infantile Langenskiold I-II, age under 3 at start of bracing, compliant family, no medial plateau step, no obesity
Intermediate prognosis: adolescent mild-moderate varus, open physis, well-aligned mechanical axis at end of guided growth
Guarded prognosis: Langenskiold IV or above, severe varus, obesity, near-skeletal maturity, recurrent disease
Key threshold: alignment of the mechanical axis by skeletal maturity is the strongest predictor of long-term knee health
Guidelines, Registries & Global Practice
- Infantile Blount disease is more common in populations of African descent, with reported higher prevalence in the Caribbean, sub-Saharan Africa, and African American populations in North America
- Adolescent Blount disease is strongly linked with childhood obesity, with rising incidence mirroring the global obesity epidemic in North America, Europe, the Middle East, and the Asia-Pacific
- Boys are affected more than girls in both forms, with a ratio of approximately 2-4 to 1
- Bilateral disease is more common in the infantile form (about 60%); unilateral disease is more common in the adolescent form
- High-resource settings: KAFO bracing, guided growth with locking plates, hexapod external fixation, and complex physeal bar resection are all available
- Limited-resource settings: bracing may be unaffordable or unavailable; closing-wedge osteotomy with cast immobilization remains an effective and inexpensive option
- Universal principle: outcome depends far more on early diagnosis, correct staging, and family compliance than on the precise surgical implant
- Multidisciplinary care: weight management, paediatric endocrinology for workup of syndromic associations, and physiotherapy are essential adjuncts in both forms
- Diagnosis emphasis
- Standing full-length radiographs, MDA, mechanical axis
- Bracing indication
- KAFO under 3 years with Langenskiöld I-II
- Surgical guidance
- Lateral hemiepiphysiodesis for adolescent; valgus osteotomy for advanced infantile
- Diagnosis emphasis
- MDA, Langenskiöld staging, and family education
- Bracing indication
- KAFO bracing with full-time wear
- Surgical guidance
- Tension-band plating for adolescent; dome or opening-wedge osteotomy for severe
- Diagnosis emphasis
- MDA threshold 11°, mechanical axis deviation
- Bracing indication
- Bracing under 3 years with stage I-II
- Surgical guidance
- Guided growth preferred in adolescent with growth remaining; osteotomy for end-stage
- Diagnosis emphasis
- Standardised radiographs and MDA measurement
- Bracing indication
- Bracing for early stage; weight management adjunct
- Surgical guidance
- Gradual correction with hexapod for severe or recurrent deformity
There is no dedicated international registry for Blount disease, unlike arthroplasty registries (NJR, AJRR, AOANJRR). The evidence base is dominated by single-centre retrospective series, technique papers on guided growth, and classic descriptive studies (Langenskiöld, Schoenecker). The MOVE paediatric registry and the multicentre paediatric deformity studies are emerging sources of higher-level evidence. Until registries mature, management is principle-based: early diagnosis, correct staging, brace under 3 years with stage I-II, guided growth in adolescent with open physis, and valgus osteotomy with overcorrection for end-stage disease.
Record in every child with tibia vara:
- Standing full-length AP radiograph with MDA and mechanical axis measurement
- Langenskiöld stage (I-VI) and laterality (bilateral vs unilateral)
- Body mass index plotted on age-appropriate growth chart
- Brace or surgical plan with family education documented
- Plan for serial monitoring and threshold for surgical referral
A missed Blount diagnosis in a child over 3 years with progressive varus and an MDA greater than 11° is a recurring source of complaints and claims worldwide. Always perform and document a standing full-length AP radiograph with MDA measurement on any child with persistent or progressive bow leg.
Controversies & Areas of Uncertainty
Bracing is widely accepted for stage I disease but its value in stage II is debated. Some series report 50-70% success in stage II children under 3; others show rapid progression to stage III despite bracing. The 6-month rule is pragmatic: if the MDA has not improved at 6 months, the brace is unlikely to work and surgery is the next step.
In moderate varus (MDA 14-16°) with an open physis, the choice between guided growth and osteotomy is debated. Guided growth is reversible and avoids the morbidity of osteotomy but requires growth remaining and does not correct internal torsion. Osteotomy produces an immediate, durable correction but carries risks of compartment syndrome, neurovascular injury, and recurrence. Surgeon preference and family counselling drive the choice.
In Langenskiöld stages IV-VI with a depressed medial plateau, the need for medial plateau elevation at the time of osteotomy is debated. Some surgeons prefer simple valgus osteotomy with overcorrection; others advocate intra-articular elevation of the depressed plateau with bone graft. The decision is based on the size of the step-off and the patient's age.
In unilateral disease, the role of prophylactic hemiepiphysiodesis of the contralateral (normal) limb to prevent limb-length discrepancy is debated. Some surgeons perform it routinely; others wait for the discrepancy to exceed 1.5-2 cm at maturity before intervening. The decision is influenced by predicted growth remaining and family preference.
MCQ Practice Points
Q: What is the metaphyseal-diaphyseal angle, and what value distinguishes Blount disease from physiological genu varum? A: The metaphyseal-diaphyseal angle of Levine and Drennan is the angle between a line through the medial and lateral beaks of the proximal tibial metaphysis and a line perpendicular to the long axis of the tibial diaphysis. A value greater than 11° distinguishes Blount disease from physiological genu varum, and a value greater than 16° is highly specific for Blount disease. The angle is measured on a standing AP radiograph of the tibia.
Q: Describe the Langenskiöld stages of Blount disease. A: The Langenskiöld classification comprises six radiographic stages. Stage I is irregularity of the medial physis with mild beaking. Stage II is a prominent medial metaphyseal beak with a cartilaginous step. Stage III shows deeper depression with less than 50% of the medial plateau involved. Stage IV has greater than 50% of the medial plateau depressed with the epiphysis beginning to form under the beak. Stage V shows a double epiphysis appearance. Stage VI is medial physeal bar formation with epiphyseal ossification over the beak - the end-stage disease.
Q: What is the first-line treatment for a 2-year-old with Langenskiöld stage I infantile Blount disease? A: The first-line treatment is knee-ankle-foot orthosis (KAFO) bracing with a valgus-producing force at the knee, worn full-time (23 hours per day) for 12 months, then night-only if correction is achieved. Success rates of 70-90% are reported in optimal candidates (age under 3, stage I or early II, compliant family). Bracing is ineffective in stage III or above, or in children over 3 years of age.
Q: A 13-year-old obese boy has adolescent Blount disease with an MDA of 15° and an open proximal tibial physis. What is the most appropriate surgical treatment? A: The most appropriate surgical treatment is lateral tension-band (8-plate) hemiepiphysiodesis of the proximal tibia, sometimes combined with a lateral distal femoral plate if there is a femoral contribution to varus. The implant is removed once the mechanical axis reaches neutral or slight valgus, typically 12-18 months after insertion. Guided growth is reversible and is preferred over osteotomy when there is at least 12-18 months of growth remaining.
Q: What is the principle of overcorrection in high tibial valgus osteotomy for Blount disease? A: The principle of overcorrection is to overcorrect the osteotomy to 5-10° of anatomic valgus at the time of surgery. This pre-empts the tendency of the medial physis to drive recurrent varus, particularly in Langenskiöld stages IV and above. Undercorrection is the most common cause of recurrence after high tibial valgus osteotomy. The principle was established in the classic Schoenecker series and remains a cornerstone of surgical planning.
Q: How do you distinguish physiological genu varum from Blount disease? A: Physiological genu varum is symmetric, smooth, and self-corrects by age 2-3, with a metaphyseal-diaphyseal angle of less than 11° and no medial metaphyseal beaking. Blount disease is sharply angulated at the proximal tibia, often unilateral (in adolescent form) or asymmetric, and is associated with lateral thrust on stance. Radiographic findings of medial beaking, an MDA greater than 11°, and a depressed medial plateau confirm Blount disease. Persistent or progressive varus after age 3 should raise suspicion for Blount disease.
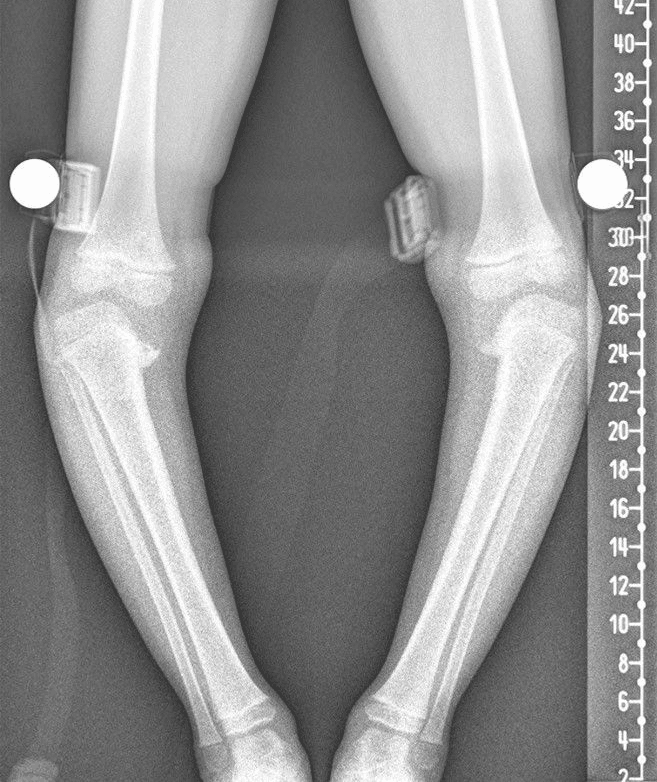
Clinical Imaging
Bilateral standing full-length anteroposterior (AP) radiographs of the lower extremities are the cornerstone of diagnosis and monitoring. The metaphyseal-diaphyseal angle and the mechanical axis deviation are measured on these films. Magnetic resonance imaging is reserved for early physeal bar detection, preoperative planning of complex deformity, and adolescent cases in which the growth plate status is uncertain.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-year-old obese boy of African descent is brought to your clinic because his parents have noticed progressive bowing of both legs. He walked at 10 months. Examination shows symmetric bilateral tibia vara with mild lateral thrust on stance. Standing full-length AP radiographs show medial metaphyseal beaking of both proximal tibiae, with a metaphyseal-diaphyseal angle of 14° on the right and 13° on the left. The medial plateau is not depressed. There is no physeal bar. How do you diagnose and manage this child?”
“A 13-year-old obese boy presents with a 6-month history of progressive left knee varus and medial joint line pain. Examination shows unilateral tibia vara with lateral thrust and intoeing. Standing radiographs demonstrate an open proximal tibial physis, a metaphyseal-diaphyseal angle of 15°, and a mechanical axis through the medial compartment (zone II). The medial plateau is not depressed. The Langenskiöld stage is II. He is otherwise healthy and active. What is the most appropriate management?”
Key Pathology
- Disorder of the medial proximal tibial physis with progressive varus, internal torsion, and medial plateau depression
- Two main forms: infantile (1-4 years, often bilateral, obese) and adolescent (over 8 years, often unilateral, obese)
- Mechanical overload of the medial physis (Hueter-Volkmann principle) drives the deformity
Diagnosis
- Standing full-length AP radiograph with MDA and mechanical axis measurement
- Metaphyseal-diaphyseal angle greater than 11° distinguishes Blount disease from physiological varum
- Langenskiöld staging (I-VI) on plain radiographs guides treatment
- MRI for suspected physeal bar or atypical or recurrent cases
Treatment Algorithm
- Infantile Langenskiöld I-II under age 3: KAFO bracing full-time for 1-2 years
- Adolescent with open physis: lateral tension-band (8-plate) hemiepiphysiodesis
- Langenskiöld III or above: high tibial valgus osteotomy with overcorrection to 5-10° valgus
- Severe multiplanar or recurrent deformity: hexapod external fixation for gradual correction
Bracing Pearls
- KAFO with valgus-producing force worn 23 hours per day for the first 12 months
- Bracing only effective in Langenskiöld I-II disease in children under 3 years
- Compliance is the single strongest predictor of success
- Failure of improvement at 6 months is the threshold to abandon the brace
Surgical Pearls
- Overcorrect valgus osteotomy to 5-10° of anatomic valgus to reduce recurrence
- Extraperiosteal plate placement in guided growth avoids iatrogenic physeal arrest
- Implant removal in guided growth is essential once mechanical axis reaches neutral
- Concomitant derotational osteotomy is needed for symptomatic internal tibial torsion
Complications
- Recurrent varus after osteotomy in 20-30% of severe cases
- Compartment syndrome in 1-5% after opening-wedge osteotomy
- Peroneal nerve neurapraxia in up to 10% after closing-wedge osteotomy
- Premature medial compartment osteoarthritis is the long-term sequela of untreated disease
Evidence Base and Key Trials
Tibia vara: osteochondrosis deformans tibiae. Blount's disease
- Original description of the six-stage radiographic classification of progressive tibia vara in children
- Stage I shows medial metaphyseal irregularity, with stages progressing to medial physeal closure and plateau depression
- Langenskiöld demonstrated that early valgus osteotomy could reverse the deformity and restore growth in stages I-III
- Established the principle that correction before skeletal maturity is essential to prevent recurrence
Physiological bowing and tibia vara. The metaphyseal-diaphyseal angle in the measurement of bowleg deformities
- Original description of the metaphyseal-diaphyseal angle of the proximal tibia
- Angle greater than 11 degrees distinguishes Blount disease from physiological genu varum in children under 4 years
- Angle greater than 16 degrees is highly specific for Blount disease
- Inter-observer reliability of the measurement is good in the hands of experienced radiologists
Guided growth for angular correction: a preliminary series using a tension band plate
- Extraperiosteal tension-band plating produces gradual correction of angular deformity about the knee in skeletally immature patients
- Mean correction of mechanical axis achieved over 12-18 months with minimal morbidity
- Reversible on implant removal; no permanent physeal injury with proper extraperiosteal technique
- Effective in obese adolescents in whom bracing and osteotomy carry higher complication rates
Orthotic treatment of infantile tibia vara
- Knee-ankle-foot orthosis bracing in Langenskiold stage I disease produced correction in the majority of children under 3 years
- Bracing success dropped sharply in stage II disease and in children over 3 years of age
- Compliance with full-time wear was the single strongest predictor of success
- Failed bracing was associated with rapid progression to higher Langenskiold stages
Elevation of the medial plateau of the tibia in the treatment of Blount disease
- Valgus high tibial osteotomy combined with medial plateau elevation produces durable correction of tibia vara
- Overcorrection to 5-10 degrees of anatomic valgus reduces recurrence
- Recurrence was common when the osteotomy was left in neutral alignment or in varus
- Best long-term outcomes were achieved in children operated on before skeletal maturity