Systematic Pattern Recognition in Skeletal Scintigraphy
Hot spots (increased uptake): Metastases, fractures, infection, arthritis, Paget disease, healing bone
Cold spots (decreased uptake): Myeloma, AVN, aggressive tumour, radiation therapy, metal artefact
Diffuse uptake (superscan): Widespread metastases, metabolic bone disease, myelofibrosis
Linear uptake: Fracture line, stress reaction, shin splints
Periarticular uptake: Arthritis (inflammatory or degenerative), CRPS
Key: Pattern recognition combined with clinical context is the key to accurate bone scan interpretation
- Bone scan detects OSTEOBLASTIC ACTIVITY — any process increasing bone turnover produces increased uptake (hot spot).
- Systematic interpretation: (1) Technical adequacy, (2) Normal variant identification, (3) Focal abnormalities, (4) Pattern recognition, (5) Clinical correlation.
- Multiple asymmetric focal hot spots in a cancer patient = metastatic disease until proven otherwise.
- A solitary hot spot in a cancer patient has only a 50% chance of being metastatic — always correlate with anatomical imaging.
- Photopenic (cold) lesions suggest: myeloma, AVN, aggressive tumour, or prior irradiation.
- “The 'superscan' (intense diffuse skeletal uptake, absent kidney/soft tissue) = widespread metastases or metabolic bone disease.
- “Flare phenomenon: bone scan may transiently worsen 2-3 months after starting effective chemotherapy due to healing response — NOT disease progression.
- “Sternal uptake alone: consider sternotomy, metastasis, or myeloma. Focal rib uptake: consider fracture (trauma or insufficiency) first.
- “Shin splints (medial tibial stress syndrome) appear as longitudinal linear uptake along the posteromedial tibia — different from a stress fracture (focal intense uptake).
- “Paget disease produces INTENSELY increased uptake, typically in the skull, pelvis, or long bones — the most intense uptake seen on bone scan.
Bone scan interpretation is frequently examined using clinical scenarios where you must identify the uptake pattern and provide a differential diagnosis. You must know: the systematic approach to interpretation, the significance of solitary vs multiple hot spots, the superscan pattern, flare phenomenon, causes of cold spots, and which malignancies produce false-negative bone scans (myeloma, renal cell carcinoma). A classic trap is diagnosing a solitary hot spot as metastasis when it has only a 50% probability.
ABCDESystematic Interpretation
Hook:ABCDE: a systematic approach that ensures nothing is missed on bone scan interpretation.
SLAPClassic Bone Scan Patterns
Hook:SLAP: Superscan, Linear fracture, Asymmetric metastases, Periarticular arthritis — the four key patterns.
MARLFalse-Negative Bone Scan (Cold Lesions)
Hook:MARL: these lesions are COLD on bone scan — a critical pitfall that can lead to missed diagnoses.
Overview
Bone scan interpretation is a fundamental skill for the orthopaedic surgery trainee, tested in both written and viva examination formats. The key to accurate interpretation is a combination of systematic reading technique, pattern recognition, and clinical correlation. A bone scan should never be interpreted in isolation — it must always be correlated with the clinical history, examination findings, laboratory results, and anatomical imaging (radiographs, CT, or MRI).
The foundation of bone scan interpretation is understanding what the scan actually measures: osteoblastic activity and local blood flow. Anything that increases either of these parameters will produce increased uptake. Conversely, processes that reduce blood flow or suppress osteoblastic activity will produce decreased uptake (photopenic or cold lesions). This is why bone scan is exquisitely sensitive but poorly specific — many different pathological (and physiological) processes can produce identical-looking hot spots.
Normal physiological uptake is seen at: (1) Growth plates in children and adolescents (intense symmetric uptake). (2) Kidneys and bladder (tracer excretion). (3) Sternoclavicular joints (commonly focally increased — normal variant). (4) Acromioclavicular joints (degenerative uptake in adults). (5) Sacroiliac joints (mild symmetric uptake). (6) Costochondral junctions (mild uptake). (7) Nasopharyngeal uptake (normal variant). Understanding these normal variants prevents false-positive interpretations.
A solitary hot spot on bone scan in a patient with known malignancy has only approximately 50% probability of representing metastasis. The differential includes: benign lesion (fibrous dysplasia, enchondroma, haemangioma), infection, degenerative change, old fracture, or Paget disease. This is why anatomical correlation (radiograph, CT, or MRI of the region) is ESSENTIAL for any solitary hot spot. Multiple asymmetric hot spots have a much higher probability (approximately 90%) of representing metastatic disease.
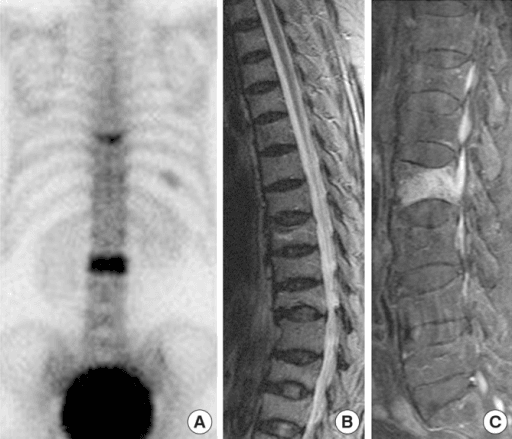
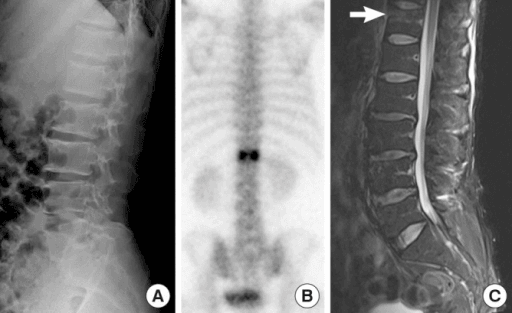
Clinical Imaging
Imaging Atlas
Systematic Approach
Structured Bone Scan Reporting
| Step | Assessment | Significance |
|---|---|---|
| 1. Technical quality | Injection site, image symmetry, artefacts, kidney visibility | Injection site extravasation invalidates quantitative assessment. Absent kidneys may indicate superscan |
| 2. Axial skeleton | Skull, mandible, spine (cervical/thoracic/lumbar/sacral), sternum, ribs | Most common sites for metastatic disease. Wedge compression fractures in spine |
| 3. Pelvis | Sacroiliac joints, iliac wings, acetabuli, pubic rami, ischial tuberosities | SI joints: sacroiliitis (bilateral) vs fracture (unilateral). Pubic rami: insufficiency fractures |
| 4. Upper limbs | Shoulders, humeri, elbows, forearms, wrists, hands | Shoulder uptake: rotator cuff disease, OA. Hand/wrist: CRPS (diffuse periarticular uptake) |
| 5. Lower limbs | Hips, femora, knees, tibiae/fibulae, ankles, feet | Knee uptake: OA, meniscal injury. Tibia: stress fracture (focal) vs shin splints (linear) |
| 6. Pattern and clinical correlation | Number, distribution, symmetry of abnormalities in context of clinical history | Single vs multiple, axial vs peripheral, symmetric vs asymmetric — determines differential |
Uptake Patterns and Differential Diagnosis
Metastatic Disease Patterns on Bone Scan
Multiple asymmetric foci (classic metastatic pattern): Random focal hot spots distributed through the axial skeleton, proximal appendicular skeleton, and ribs. Key features: (1) asymmetric, (2) variable intensity, (3) predominantly axial, (4) ribs and spine most commonly involved. In a patient with known malignancy, this pattern has a greater than 90% specificity for metastatic disease.
Solitary hot spot: Only approximately 50% represent metastasis in a cancer patient. Must correlate with anatomical imaging. The most common sites for solitary metastases: vertebral body (rather than posterior elements), ribs, and pelvis.
Superscan: Diffuse intense skeletal uptake with absent/faint kidney and soft tissue activity. Seen with: (1) widespread osteoblastic metastases (prostate, breast cancer), (2) metabolic bone disease (renal osteodystrophy, hyperparathyroidism). The key diagnostic clue is the ABSENT KIDNEYS — the skeleton extracts nearly all tracer.
Flare phenomenon: A transient increase in bone scan uptake 2-6 months after starting effective chemotherapy or hormonal therapy. This represents healing of metastatic lesions — increased osteoblastic activity is a sign of repair, NOT disease progression. The flare phenomenon resolves by 6-12 months. It is a common exam question because misinterpretation leads to incorrect treatment changes.
Cancers with false-negative bone scans (predominantly lytic): Multiple myeloma, renal cell carcinoma, thyroid cancer (follicular), and some lung cancers. These tumours produce osteoclastic lesions without sufficient osteoblastic response to be detected.
Differential Diagnosis of the Solitary Hot Spot
The single most common interpretation challenge is the solitary focus of increased uptake. The pattern, intensity, anatomical site and clinical context narrow a broad differential. Use this table to reason through it systematically rather than defaulting to "metastasis".
| Diagnosis | Typical site / pattern | Discriminating features |
|---|---|---|
| Metastasis | Vertebral body, pelvis, proximal long bone; round, asymmetric | Known primary, posterior element sparing favours benign; vertebral body involvement raises concern; correlate with CT/MRI |
| Fracture (traumatic/insufficiency/stress) | Rib (linear, aligned), pubic ramus, sacrum, tibia | History of trauma or osteoporosis; linear or aligned uptake; ribs in a row strongly favour fracture over metastasis |
| Degenerative / osteoarthritis | Facet joints, AC joint, knee, first CMC, hips | Periarticular, often symmetric, matches radiographic OA; very common incidental cause |
| Paget disease | Pelvis, skull, vertebra, long bone | Intense uptake involving the WHOLE bone end-to-end, bone expansion; the most intense uptake seen |
| Infection (osteomyelitis) | Metaphysis (children), spine, diabetic foot | Three-phase positivity (flow + pool + delayed); clinical sepsis, raised inflammatory markers; SPECT/CT or labelled WCC for confirmation |
| Benign tumour (osteoid osteoma, fibrous dysplasia, enchondroma) | Long bone, varies | Osteoid osteoma: intense focal 'double-density' nidus; correlate with characteristic CT/MRI features and age |
Controversies & Areas of Uncertainty
The role of planar bone scan is contracting as PSMA PET (prostate), FDG PET-CT (breast, lung, lymphoma) and whole-body diffusion MRI demonstrate higher specificity and detect marrow and extra-skeletal disease. There is no global consensus on when bone scan is still first-line versus replaced; availability and cost drive much of the variation, and guidelines lag behind the evidence.
SPECT/CT improves localisation and specificity (e.g. distinguishing facet OA from a vertebral body metastasis), but it adds radiation, cost and time. The threshold for adding SPECT/CT to a planar study, and whether it should be routine for spinal lesions, remains debated.
No single imaging criterion reliably separates a 3-month healing flare from true progression. Reliance on serial scanning, symptom trajectory and bone-turnover or tumour markers means a degree of clinical uncertainty is unavoidable in this window — a recognised limitation rather than a solved problem.
Three-phase bone scan is sensitive but poorly specific for infection in the presence of recent surgery, fracture, neuropathic joint or prosthesis. Whether to use labelled-leucocyte imaging, SPECT/CT or MRI next is institution-dependent and not fully standardised across guidelines.
Evidence Base
Diagnostic Accuracy of Bone Scintigraphy for Skeletal Metastases
- Across 11 studies (753 breast cancer patients), planar/SPECT bone scintigraphy had a pooled patient-based sensitivity of 90% (95% CI 86-93) and specificity of 91% (95% CI 87-94), with an SROC area under the curve of 0.93.
- FDG PET/CT showed comparable sensitivity (92%) but markedly higher specificity (99%); Na-18F PET/CT had the highest sensitivity (96%) but lower specificity (81%).
- Bone scintigraphy retained good overall accuracy but was outperformed on specificity by FDG PET/CT, which also detects extra-skeletal disease.
Solitary Rib Hot Spots Are Usually Benign in Cancer Patients
- Review of 2,851 bone scans at a cancer centre identified 41 patients whose first abnormal finding was a solitary rib lesion.
- Only 4 of 41 (9.8%) were due to malignancy; 39% were associated with benign fractures, 27% with prior or postoperative radiotherapy, and 24% were assigned a benign aetiology with normal radiographs.
- Overall, approximately 90% of solitary rib hot spots in cancer patients were benign.
Solitary hot spots require careful anatomical correlation before making management decisions; site matters, with ribs being the least likely to be malignant.
Guidelines, Registries & Global Practice
Technetium-99m diphosphonate (MDP/HDP) bone scintigraphy is one of the most frequently performed nuclear medicine studies worldwide, used across every health system for metastatic screening, evaluation of bone pain, occult and stress fracture detection, prosthetic loosening/infection assessment, and characterisation of metabolic bone disease. The whole-body planar study is inexpensive, available in virtually every nuclear medicine department, and has a high sensitivity for osteoblastic disease — properties that keep it relevant globally despite the rise of PET.
EANM (European Association of Nuclear Medicine) and SNMMI (US Society of Nuclear Medicine and Molecular Imaging) publish procedure standards for planar/SPECT bone scintigraphy and recommend SPECT or SPECT/CT to localise and characterise equivocal lesions (especially in the spine). For prostate cancer, EAU and NCCN reserve bone scan for higher-risk disease (e.g. PSA over 20, Gleason/ISUP high grade, or T3-T4), increasingly favouring PSMA PET where available. For breast cancer, ESMO and NCCN recommend bone scan or FDG PET-CT for staging when metastasis is suspected. In suspected diabetic foot osteomyelitis, IWGDF/IDSA favour MRI or labelled-leucocyte/SPECT-CT over three-phase bone scan alone because of limited specificity.
The International Myeloma Working Group (IMWG) explicitly recommends AGAINST conventional bone scan for myeloma, because lytic lesions are frequently false-negative. Whole-body low-dose CT, whole-body MRI, or FDG PET-CT are the recommended modalities — a high-yield distinction that every candidate must know.
Registry and outcome data feed back into how the scan is used: arthroplasty registries (NJR, AOANJRR, AJRR, Swedish/Norwegian) track revision for periprosthetic infection and loosening, conditions in which three-phase bone scan and SPECT/CT contribute to the diagnostic pathway alongside aspiration and inflammatory markers. The Bone Scan Index, validated in androgen-independent prostate cancer, quantifies skeletal tumour burden and prognosis and illustrates how a qualitative scan can be made quantitative for trials.
High- versus limited-resource practice variation: In well-resourced systems, PET-CT (FDG, Na-18F, or PSMA) and whole-body MRI increasingly replace planar bone scan for staging and treatment-response assessment, offering higher specificity and extra-skeletal evaluation. In limited-resource settings, planar Tc-99m bone scintigraphy remains the workhorse for metastatic screening because of low cost, wide availability of generator-produced technetium, and robust sensitivity; SPECT/CT and PET may be regionally centralised or unavailable. Sound interpretation of the planar scan — the focus of this topic — therefore remains a globally essential skill.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“You are shown a bone scan of a 55-year-old woman with breast cancer who was recently started on chemotherapy. The scan shows more hot spots than her baseline scan 3 months ago.”
“A 70-year-old woman presents with acute low back pain after bending to pick up groceries. Her bone scan shows H-shaped uptake in the sacrum.”
“An examiner asks you to explain why a patient with known multiple myeloma has a normal bone scan despite widespread skeletal disease on CT.”
Systematic Approach (ABCDE)
- Adequacy: image quality, injection site, artefacts
- Background: overall uptake, kidney visibility (absent = superscan)
- Compare sides: asymmetry is significant
- Describe: location, intensity, pattern, number
- Explain: correlate with clinical history and anatomical imaging
Classic Patterns (SLAP)
- Superscan: diffuse intense uptake, absent kidneys — metastases or metabolic bone disease
- Linear uptake: fracture (stress, insufficiency, traumatic)
- Asymmetric random foci: metastatic disease (more than 90% probability if multiple)
- Periarticular uptake: arthritis (bilateral) or CRPS (unilateral)
False Negatives (MARL)
- Myeloma (lytic, no osteoblastic response — DKK1 suppression)
- AVN (early, before revascularisation)
- Rapidly destructive tumour (outpaces repair)
- irradiated Lesions (suppressed vascularity and turnover)
Special Patterns
- Honda sign: H-shaped sacral uptake = insufficiency fractures
- Flare phenomenon: scan worsens at 2-3 months on effective treatment — NOT progression
- Train-track sign (HPOA): bilateral cortical uptake in long bones
- Doughnut sign (AVN): cold centre with ring of peripheral uptake
Hot Spot Statistics
- Solitary hot spot in cancer patient: only 50% probability of metastasis
- Multiple asymmetric hot spots: more than 90% probability of metastases
- Solitary rib hot spot: most likely fracture (not metastases)
- Always correlate with anatomical imaging for any hot spot