CDR, ACDF and Posterior Foraminotomy
- Anterior cervical discectomy and fusion (ACDF) is the long-standing BENCHMARK operation for cervical radiculopathy and myelopathy from anterior compression; it is reliable and effective, but because it ELIMINATES segmental motion it has been theorised to accelerate ADJACENT-SEGMENT degeneration, which is the rationale for motion-preserving alternatives.
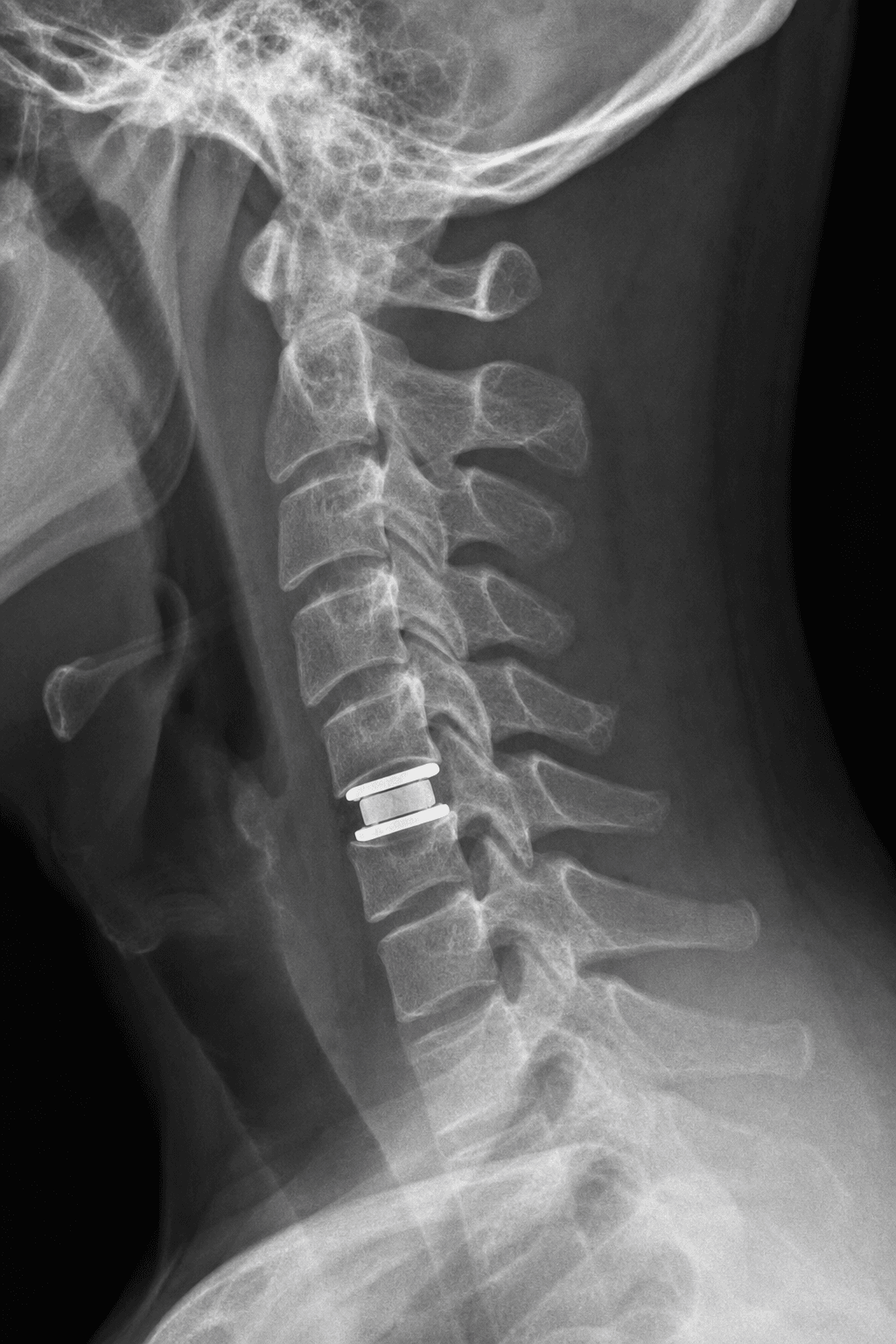
- Cervical total disc replacement (CDR/arthroplasty) preserves segmental MOTION at the operated level, aiming to reduce adjacent-segment disease; the ideal candidate has SOFT-disc radiculopathy or myelopathy at one or two levels with PRESERVED segmental motion and good bone quality, and WITHOUT the contraindications below.
- The CONTRAINDICATIONS to CDR are important: segmental INSTABILITY, significant FACET (or uncovertebral) ARTHROSIS, fixed KYPHOSIS or significant deformity, OSTEOPOROSIS, ossification of the posterior longitudinal ligament (OPLL) or marked spondylosis/ankylosis, infection, and significant axial-neck-pain-predominant disease - in these, fusion (ACDF) is preferred.
- The EVIDENCE shows CDR is at LEAST EQUIVALENT (non-inferior, often slightly better) to ACDF: large randomised IDE trials and long-term data show comparable or superior clinical outcomes with motion preservation and generally lower rates of adjacent-segment reoperation, and CDR has been found to be cost-effective; however, a national REGISTRY (propensity-matched) found NO clinically important difference in patient-reported outcomes between CDR and ACDF at 5 years - so the real-world advantage is modest.
- POSTERIOR CERVICAL FORAMINOTOMY is the other fusion-sparing option: for a LATERAL (foraminal) SOFT-DISC herniation or a foraminal osteophyte causing predominantly radicular symptoms, a posterior keyhole foraminotomy decompresses the exiting nerve root WITHOUT a fusion or an anterior approach (avoiding the small risks of dysphagia, recurrent laryngeal nerve injury and pseudarthrosis), preserving motion - but it does not address central/anterior compression or kyphosis and is less suited to soft central discs.
- The practical decision is therefore individualised: ACDF remains the versatile benchmark (especially for multilevel disease, instability, deformity, OPLL or where fusion is otherwise indicated); CDR is offered to the well-selected motion-preservation candidate; and posterior foraminotomy is chosen for foraminal radiculopathy from a lateral soft disc/osteophyte - matching the operation to the pathology and the patient.
- “ACDF = the benchmark (reliable, but eliminates motion -> adjacent-segment theory). CDR preserves MOTION; for SOFT-disc radiculopathy/myelopathy with preserved motion and no instability/facet arthrosis/kyphosis/OPLL/osteoporosis.
- “RCT/IDE evidence: CDR at least EQUIVALENT to ACDF (often slightly better, fewer adjacent-segment reoperations, cost-effective); registry shows NO clinically important difference at 5 years.
- “Posterior cervical FORAMINOTOMY = fusion-sparing option for LATERAL (foraminal) soft-disc/osteophyte radiculopathy (not central/anterior or kyphosis).
CDR for soft-disc radiculopathy/myelopathy with preserved motion and no instability, facet arthrosis, kyphosis, OPLL or osteoporosis - at least equivalent to ACDF.
ACDF for multilevel disease, instability, deformity, OPLL. Posterior foraminotomy for lateral (foraminal) soft-disc/osteophyte radiculopathy.
The Three Operations & Their Indications
ACDF (anterior cervical discectomy and fusion) is the versatile benchmark for cervical radiculopathy/ myelopathy from anterior compression - reliable, but it eliminates segmental motion and is theorised to accelerate adjacent-segment degeneration. CDR (cervical total disc replacement) preserves segmental motion to reduce adjacent-segment disease, and is offered to the well-selected patient with soft-disc radiculopathy/myelopathy, preserved motion and good bone quality, and without instability, significant facet/uncovertebral arthrosis, kyphosis/deformity, osteoporosis or OPLL. Posterior cervical foraminotomy is a fusion-sparing posterior option for a lateral (foraminal) soft-disc herniation or osteophyte causing radiculopathy, decompressing the root without fusion or an anterior approach - but it does not address central/ anterior compression or kyphosis.
| Feature | ACDF | CDR | Posterior foraminotomy |
|---|---|---|---|
| Motion | Eliminated (fusion) | Preserved (arthroplasty) | Preserved (no fusion) |
| Best for | Anterior/central compression, multilevel, instability, deformity, OPLL | Soft-disc radiculopathy/myelopathy, preserved motion, no arthrosis/kyphosis | Lateral (foraminal) soft disc/osteophyte radiculopathy |
| Key drawback | Loss of motion; adjacent-segment theory; pseudarthrosis | Strict patient selection; contraindicated with instability/arthrosis/OPLL | Not for central/anterior compression or kyphosis |
| Evidence | Long-standing benchmark | At least equivalent to ACDF; fewer adjacent-segment reoperations; cost-effective | Effective, fusion-sparing for selected foraminal radiculopathy |
What the Evidence Shows
- Randomised/IDE trials: CDR is at least equivalent (non-inferior) to ACDF, often with slightly better outcomes and generally fewer adjacent-segment reoperations at long term, and CDR has been found cost-effective over a multi-year horizon.
- Registry (real-world): a propensity-matched national registry found no clinically important difference
in patient-reported outcomes (Neck Disability Index, pain, quality of life) between CDR and ACDF at 5 years
- so the real-world advantage is modest and patient selection is what matters.
- Selection drives success: offer CDR to the motion-preservation candidate (soft disc, preserved motion, no contraindications); choose ACDF for multilevel disease, instability, deformity or OPLL.
- Posterior foraminotomy is a strong fusion-sparing choice for foraminal radiculopathy from a lateral soft disc/osteophyte, avoiding fusion, anterior-approach risks and motion loss."
The decisive factor in cervical degenerative surgery is not which device is theoretically superior but matching the operation to the pathology and the patient. CDR's motion preservation only helps the right patient: it is contraindicated by instability, significant facet or uncovertebral arthrosis, fixed kyphosis or deformity, osteoporosis and OPLL, in which fusion is safer and more durable. The evidence supports CDR as at least equivalent to ACDF and cost-effective, but a real-world registry shows no clinically important difference at five years - so do not over-sell motion preservation. For a lateral foraminal soft disc or osteophyte causing radiculopathy, posterior foraminotomy decompresses the root without any fusion or anterior-approach risks. Choose deliberately, and reserve ACDF as the versatile benchmark for the cases the alternatives cannot serve.
Evidence & Key Studies
Artificial disc replacement vs fusion for cervical radiculopathy: 5-year registry outcomes (Swespine)
- In a propensity-matched national registry (185 per group) of cervical degenerative disc disease with radiculopathy, Neck Disability Index scores roughly halved in both arthroplasty and fusion groups by 5 years.
- There was no significant difference in NDI between CDR and ACDF, and no difference in quality of life (EQ-5D) or neck/arm pain.
- Decompression plus arthroplasty did not produce a clinically important difference in outcomes versus decompression and fusion at 5 years.
Cost-effectiveness of ACDF versus cervical disc replacement at 7 years (Markov analysis)
- Both ACDF and CDR are cost-effective strategies for single-level cervical disc degeneration; past large randomised IDE studies show at least equal effectiveness of CDR versus ACDF.
- Over a 7-year horizon, CDR generated more quality-adjusted life-years than ACDF and was the more cost-effective procedure (incremental cost-effectiveness ratio favouring CDR, well below standard willingness-to-pay).
- Adjacent-segment disease and other complications occurring after 5 years are relevant to the longer-term comparison.
According to PubMed, the real-world finding of no clinically important difference between CDR and ACDF at 5 years in patient-reported outcomes comes from the cited MacDowall (Swespine) registry study; the at-least-equal effectiveness of CDR in randomised IDE studies and the 7-year cost-effectiveness favouring CDR (with adjacent- segment disease relevant at longer term) from the cited Kim analysis. The indications/contraindications for CDR, the adjacent-segment rationale, and the role of posterior cervical foraminotomy for foraminal radiculopathy are standard, well-established teaching. (See also our Cervical Radiculopathy and Cervical Spondylotic Myelopathy topics.)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“When would you choose cervical disc replacement over ACDF, and what does the evidence show?”
“Where does posterior cervical foraminotomy fit?”
Mnemonics & Memory Aids
MOTION
Hook:MOTION: Motion preserved by CDR, OPLL/Osteoporosis contraindicate, Two levels soft disc OK, Instability contraindicates, Outcomes at least equal, Nerve-root foraminal -> foraminotomy.
The operations
- ACDF: fusion - versatile benchmark; eliminates motion (adjacent-segment theory)
- CDR: arthroplasty - preserves motion; reduce adjacent-segment disease
- Posterior foraminotomy: fusion-sparing posterior option (foraminal soft disc/osteophyte)
CDR selection
- Soft-disc radiculopathy/myelopathy, 1-2 levels, preserved motion, good bone
- Contraindications: instability, facet/uncovertebral arthrosis, kyphosis/deformity, osteoporosis, OPLL
- Predominant axial neck pain is a poor indication
Evidence
- RCT/IDE: CDR at least equivalent (often slightly better), fewer adjacent-segment reoperations
- Cost-effective over multi-year horizon
- Registry: no clinically important difference vs ACDF at 5 years
Posterior foraminotomy
- For lateral (foraminal) soft disc/osteophyte radiculopathy
- Decompresses root without fusion/anterior approach (preserves motion)
- Not for central/anterior compression, kyphosis or instability