Cerebellar tonsils herniate below the foramen magnum | Drives a syrinx | The syrinx causes atypical scoliosis and neuropathic joints | MRI the whole spine, decompress before you fuse
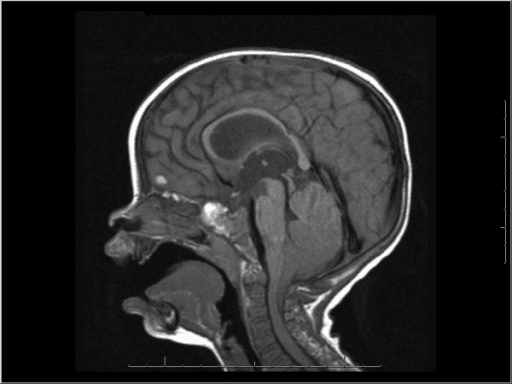
- What it is: in Chiari I the cerebellar tonsils sit too low, herniating 5mm or more below the foramen magnum and crowding the cervicomedullary junction - this is a structural problem at the bottom of the skull, not a primary bone problem
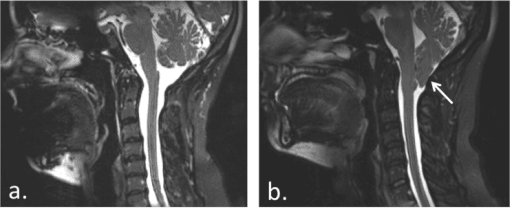
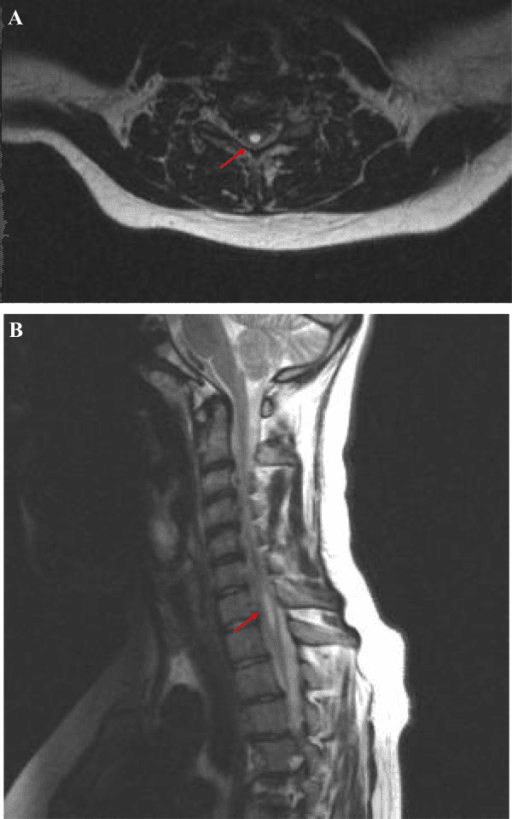
- Why orthopaedics cares: the herniation disturbs cerebrospinal fluid flow and drives a fluid cavity in the cord (a syrinx / syringomyelia). The syrinx - not the tonsil position itself - is what produces the orthopaedic problems
- Scoliosis is the headline link: Chiari I (especially with a syrinx) causes scoliosis with atypical features - left-sided thoracic curves, pain, neurological signs, and rapid progression, often in a younger child
- Neuropathic (Charcot) joints: a cervical syrinx destroys pain and temperature sensation in the arms (cape distribution), so the shoulder or elbow can be destroyed painlessly - a classic upper-limb neuropathic joint
- The exam rule: any scoliosis with atypical features needs a whole-spine MRI including the craniocervical junction. If you find Chiari plus a syrinx, the neurosurgeon usually does a posterior fossa decompression first, then you address the curve
- “A LEFT thoracic curve in idiopathic-looking scoliosis is a red flag - image the neuraxis to exclude Chiari and a syrinx
- “It is the SYRINX, not the tonsillar descent alone, that correlates with scoliosis and neuropathic joints
- “Decompress the Chiari/syrinx BEFORE fusing the spine - it can stabilise or improve smaller, younger curves and protects the cord during deformity surgery
- “A painlessly destroyed shoulder with absent pain/temperature sensation in the arms is neuropathic arthropathy from a cervical syrinx until proven otherwise
Scoliosis with any of: a left thoracic curve, pain, neurological signs, an abnormal abdominal reflex, rapid progression, or a young age is not safely "idiopathic". Order a whole-spine MRI including the craniocervical junction to look for Chiari and a syrinx before you treat the curve.
Tonsillar descent alone correlates poorly with the spine problem. The syringomyelia is what drives scoliosis and neuropathic joints. A larger syrinx is more likely to be associated with scoliosis, and the side of the syrinx tends to match the convexity of the curve.
In a child with Chiari, a syrinx, and scoliosis, the usual sequence is posterior fossa decompression first, then reassess the curve. Decompression can halt or improve smaller curves in younger children and shrinks the syrinx, reducing the risk to the cord during any later deformity surgery.
A cervical syrinx wipes out pain and temperature sensation in the arms (a "cape" distribution) while leaving other senses. The result is a neuropathic (Charcot) shoulder or elbow - a swollen, unstable, grossly destroyed joint that does not hurt. Suspect a syrinx and image the neuraxis.
Overview
A Chiari malformation is a structural problem at the junction of the skull and the spine, where part of the cerebellum - the cerebellar tonsils - sits too low and herniates down through the foramen magnum (the large hole at the base of the skull where the brainstem becomes the spinal cord). The type the orthopaedic surgeon meets is Chiari I, defined on MRI as tonsils lying 5mm or more below the foramen magnum.
On its own, a low tonsil might seem like a neurosurgical curiosity. The reason it lands on the orthopaedic radar is what it does downstream. The crowded foramen magnum disturbs the normal pulsatile flow of cerebrospinal fluid (CSF) around the cord, and over time this drives the formation of a fluid-filled cavity inside the spinal cord itself - a syrinx, the condition called syringomyelia. That syrinx is the real troublemaker. It produces two classic orthopaedic problems: an atypical scoliosis and a neuropathic (Charcot) joint in the upper limb.
For the exam, the whole topic reduces to a simple chain of reasoning: Chiari low tonsils, then blocked CSF flow, then a syrinx in the cord, then scoliosis and/or neuropathic joints. Your job is to recognise when a "routine" scoliosis is hiding this chain, to image the right thing (the whole neuraxis), and to know the order of operations - decompress the Chiari before you fuse the spine.
Pathophysiology
The anatomy. The cerebellum sits in the posterior fossa, the lowest compartment of the skull, just above the foramen magnum. Its lowest parts, the tonsils, normally rest at or above the level of the foramen magnum. In Chiari I the posterior fossa is often small or shallow, so the tonsils are pushed down and herniate below the foramen magnum, crowding the cervicomedullary junction where the brainstem becomes the spinal cord.
How the syrinx forms. CSF normally pulses freely up and down across the foramen magnum with each heartbeat and breath. The herniated tonsils act like a plug, obstructing CSF flow and creating abnormal pressure waves at the craniocervical junction. The leading explanation is that these disturbed pressure dynamics drive fluid into and along the spinal cord, hollowing out a central cavity over months to years - the syrinx. The exact mechanism is debated, but the practical point is fixed: relieving the obstruction (decompression) is what allows the syrinx to shrink.
Why the syrinx causes scoliosis. A syrinx expands within the central cord and damages the crossing fibres and motor pathways asymmetrically. This is thought to cause uneven activity in the paraspinal muscles on the two sides of the spine, pulling the spine into a curve. Because the cause is neurological and often asymmetric, the resulting scoliosis behaves differently from ordinary idiopathic scoliosis - the curve is frequently left-sided in the thoracic spine and may progress fast.
Why the syrinx causes neuropathic joints. The fibres carrying pain and temperature sensation cross in the very centre of the cord, right where the syrinx expands. A cervical syrinx therefore knocks out pain and temperature sensation in the arms while light touch and position sense are relatively preserved - a "dissociated" sensory loss in a cape distribution across the shoulders and arms. Without protective pain sensation, repeated micro-trauma destroys the joint painlessly: a neuropathic (Charcot) joint, classically of the shoulder or elbow.
The single most useful concept to carry into the viva: it is the syrinx, not the tonsil position, that links Chiari to the spine and joints. Studies repeatedly show that the presence and size of the syrinx - not how far the tonsils descend - track with scoliosis and with neuropathic joints.
Classification
The Chiari types are a favourite quick-fire question. For orthopaedics, you mostly care about type I, but you should be able to separate it cleanly from type II.
- What herniates / key feature
- Cerebellar tonsils 5mm or more below the foramen magnum; small posterior fossa; often a syrinx
- Orthopaedic relevance
- The one you meet - linked to atypical scoliosis and upper-limb neuropathic joints
- What herniates / key feature
- Tonsils plus brainstem and vermis herniate; almost always with a myelomeningocele (open spina bifida)
- Orthopaedic relevance
- Seen in spina bifida; complex spinal deformity but a different patient group
- What herniates / key feature
- Herniation of posterior fossa contents into a high cervical/occipital encephalocele
- Orthopaedic relevance
- Rare and severe; neonatal neurosurgical problem
- What herniates / key feature
- Cerebellar hypoplasia/aplasia without herniation (terminology now disputed)
- Orthopaedic relevance
- Rare; of academic interest only
"Arnold-Chiari" strictly refers to type II, the one bound up with spina bifida. In everyday speech people loosely call any Chiari "Arnold-Chiari", but in a viva, reserve the eponym for type II and call the common adult/orthopaedic form Chiari I.
Associated Craniovertebral Junction Anomalies
Chiari I sits at the craniovertebral junction (CVJ), and the orthopaedic surgeon must remember it frequently coexists with bony CVJ anomalies that can cause instability and change the operation from a simple decompression to an occipitocervical fusion.
Anomalies to look for on MRI/CT:
- Basilar invagination - the odontoid peg projects up through the foramen magnum into the posterior fossa, further crowding the cervicomedullary junction; a reason a simple posterior decompression alone may fail.
- Atlas (C1) assimilation / occipitalisation - congenital fusion of C1 to the occiput, which reduces space at the foramen magnum and shifts stress to C1-2.
- Atlanto-axial instability - may need reduction and occipitocervical or C1-2 fusion rather than decompression alone.
- Klippel-Feil syndrome (congenitally fused cervical vertebrae, short webbed neck, low hairline) and Sprengel deformity are recognised associations to screen for.
- Platybasia (flattening of the skull base) often accompanies these.
The classic CVJ measurement lines (high-yield):

- How it is drawn
- Posterior hard palate to the posterior margin of the foramen magnum (opisthion)
- What it assesses
- Basilar invagination if the odontoid tip is more than about 3-5 mm above it
- How it is drawn
- Posterior hard palate to the lowest point of the occiput (easy on plain films)
- What it assesses
- Basilar invagination if the odontoid tip is more than about 4.5 mm above it
- How it is drawn
- Across the foramen magnum (basion to opisthion)
- What it assesses
- The odontoid tip should lie below it; a functional measure of foramen magnum compromise
- How it is drawn
- Drawn down the clivus
- What it assesses
- Should be tangential to the odontoid tip; the tip crossing it suggests basilar invagination / instability
Do not treat Chiari I purely as a soft-tissue tonsil problem. Screen the bony craniovertebral junction for basilar invagination, C1 assimilation, atlanto-axial instability and Klippel-Feil, using Chamberlain's, McGregor's, McRae's and Wackenheim's lines. If there is instability or irreducible bony compression, management shifts toward reduction and occipitocervical fusion, not decompression alone.
Clinical Presentation
Chiari I reaches the orthopaedic clinic in a few recognisable ways. Most often it is discovered when an MRI is done for scoliosis; sometimes it presents through the neurological features of the malformation or the syrinx, and occasionally through a dramatic neuropathic joint.
Often the first presentation. The curve may look "idiopathic" but carries atypical features - left thoracic apex, pain, neurological signs, fast progression, young age. These are exactly the features that should trigger neuraxis imaging.
A classic cough/strain headache at the back of the head and neck (worse on coughing, sneezing, or straining), neck pain, dizziness, and balance or swallowing problems from brainstem and cerebellar crowding.
Dissociated sensory loss (lost pain and temperature, preserved touch) in a cape distribution, wasting and weakness of the hands, painless burns or cuts on the fingers, and upper-limb reflex changes.
A swollen, unstable, grossly destroyed shoulder or elbow that is strikingly painless. This dramatic upper-limb arthropathy should prompt a hunt for a cervical syrinx and Chiari.
Examination clues that change your plan
- Abdominal reflexes: asymmetric or absent superficial abdominal reflexes are a well-known soft sign of an underlying cord problem in a child with scoliosis - check them.
- Upper motor neurone signs in the legs (brisk reflexes, clonus, upgoing plantars) with lower motor neurone signs in the hands (wasting) suggest a cervical cord lesion such as a syrinx.
- Dissociated sensory loss - test pain/temperature versus light touch separately; loss of one with preservation of the other points squarely at a central cord cavity.
Investigations
The investigation that matters is MRI, and the exam point is what to scan and when.
The key investigation. Image the entire neuraxis including the craniocervical junction so you capture both the tonsillar herniation and any syrinx running down the cord. A scoliosis film alone will miss the cause.
Measure tonsillar descent below the foramen magnum (5mm or more defines Chiari I) and note the posterior fossa morphology. Remember descent alone correlates poorly with the spine problem.
Record the syrinx length, width, and level, because syrinx size and side track with scoliosis. The side of the syrinx tends to match the convexity of the curve.
Full-length standing PA and lateral films to measure the Cobb angle, characterise the curve, and follow progression - the curve shape (for example a left thoracic apex) is itself a clue.
Do not treat "atypical" scoliosis as idiopathic. Image the neuraxis if there is a left thoracic curve, pain, any neurological sign, an abnormal abdominal reflex, rapid progression, or onset at a young age. Finding a Chiari and syrinx changes the entire management plan - and missing it risks neurological injury during deformity surgery.
If asked "what is the single best investigation for atypical scoliosis?", answer whole-spine MRI including the craniocervical junction - and say why: it shows both the Chiari (tonsillar descent) and the syrinx (the actual driver), which together dictate the order of surgery.
Differential: Other Causes of a Syrinx and of Atypical Scoliosis
A whole-neuraxis MRI for atypical scoliosis is not just "looking for a Chiari." It screens for the whole family of intraspinal causes of a non-idiopathic curve, and a syrinx itself has causes other than Chiari.
Other causes of syringomyelia (a syrinx is not always Chiari):
- Post-traumatic - a delayed, ascending syrinx after spinal cord injury causing late neurological decline.
- Post-infective / post-inflammatory arachnoiditis (e.g. after meningitis or tuberculosis) tethering the cord and blocking CSF flow.
- Intramedullary spinal cord tumour (e.g. ependymoma, haemangioblastoma) with an associated tumoural syrinx - a key one not to miss.
- Tethered cord and other closed dysraphism.
Other intraspinal causes of atypical / non-idiopathic scoliosis the MRI must exclude:
- Tethered cord syndrome (low conus, thickened filum) - look for cutaneous stigmata (hairy patch, dimple, lipoma).
- Diastematomyelia / split cord malformation - a bony or fibrous septum splitting the cord, which must be addressed before deformity correction.
- Intraspinal / intramedullary tumour.
- Neurofibromatosis type 1 (short sharp dystrophic curves, café-au-lait spots) and other syndromic causes.
"Atypical scoliosis, so MRI the neuraxis" is not only a Chiari hunt. The same scan screens for a tethered cord, diastematomyelia (split cord), an intramedullary tumour and a non-Chiari syrinx (post-traumatic, post-inflammatory or tumoural). Any of these can drive the curve, and several (a split cord, a tethered cord, a tumour) must be addressed before the deformity is corrected.
Management
Management is multidisciplinary - the neurosurgeon deals with the Chiari and syrinx, the orthopaedic spine surgeon deals with the curve - and the sequence is the high-yield point.
Whole-neuraxis MRI to confirm Chiari I, measure tonsillar descent, and map the syrinx. Standing films to size the curve. Full neurological examination.
If there is a symptomatic Chiari and/or a syrinx, the neurosurgeon typically performs posterior fossa decompression (removing a little occipital bone and the back of C1, often with a duraplasty to enlarge the space). This restores CSF flow and usually shrinks the syrinx.
After decompression, watch the scoliosis. In younger children with smaller curves, decompression can halt or even improve the curve, sometimes avoiding fusion. Brace small flexible curves as you would otherwise.
If the scoliosis continues to progress or is already large, proceed to posterior spinal fusion. Doing the decompression first reduces the neurological risk of correcting the deformity on a cord that contains a syrinx.
Why decompress before fusing?
Two reasons, both examinable. First, the curve may respond - relieving the obstruction and shrinking the syrinx can stop a young curve from worsening, so you may avoid or delay a big fusion. Second, safety: correcting a deformity stretches and manipulates the cord. A cord that contains a syrinx and sits under an obstructed craniocervical junction is more vulnerable to a neurological injury, so it is safer to decompress and let the syrinx settle before applying corrective forces.
The order of operations is the marks-winning answer: MRI the neuraxis, then posterior fossa decompression first, then reassess the curve, then fuse only if it progresses. Decompression both protects the cord and may improve smaller, younger curves.
Complications
- Why it happens
- Syrinx damages crossing fibres and unbalances paraspinal muscles
- Key point
- Left thoracic, painful, neurological, fast - image the neuraxis
- Why it happens
- Cervical syrinx removes pain and temperature sensation in the arms
- Key point
- Painless, swollen, destroyed joint - high failure rate if operated
- Why it happens
- Syrinx damages anterior horn cells in the cervical cord
- Key point
- Lower motor neurone signs in the hands with upper motor neurone signs in the legs
- Why it happens
- Correcting a curve stresses a cord already compromised by a syrinx
- Key point
- Decompress first; monitor the cord during correction
- Why it happens
- Decompression does not help every curve, especially larger/older
- Key point
- About 38% still need fusion; older age and larger curve predict progression
- Why it happens
- Dissociated sensory loss in a cape distribution
- Key point
- A soft sign that should trigger neuraxis imaging
Neuropathic (Charcot) joint - the upper-limb classic
The destroyed shoulder of syringomyelia is a favourite exam image. Because the cervical syrinx abolishes pain and temperature sensation in the arms, the joint is repeatedly injured without the patient noticing, leading to a grossly swollen, unstable, painless joint with massive bony destruction and debris on radiographs. The crucial lessons are: (1) a painless destroyed upper-limb joint is a syrinx until proven otherwise - image the neuraxis; and (2) operating on a neuropathic joint is hazardous - arthroplasty and fusion fail at high rates because protective sensation is gone, so management is usually supportive plus treatment of the underlying syrinx.
Neuropathic joints have a memorable distribution by cause: syringomyelia goes to the upper limb (shoulder, elbow); diabetes goes to the foot; tabes dorsalis goes to the knee and hip. A painless destroyed shoulder should make you say "syringomyelia, exclude a Chiari".
Clinical Relevance
For the orthopaedic exam, Chiari I is really a scoliosis-screening and spinal-cord-safety topic dressed up as a brain malformation. It appears in paediatric and adult spine vivas (atypical scoliosis, "when do you MRI the neuraxis?", "what order do you operate in?"), in upper-limb vivas (the painless destroyed shoulder), and in basic-science discussions of CSF dynamics and syrinx formation. The whole topic hangs on one chain - low tonsils, then obstructed CSF, then a syrinx, then scoliosis and neuropathic joints - and on two practical rules: image the whole neuraxis in atypical scoliosis, and decompress the Chiari before you fuse the spine. Get those across and you have the marks.
Guidelines, Registries and Global Practice
- Neuraxis imaging in atypical scoliosis is a globally consistent message: scoliosis with a left thoracic apex, pain, neurological signs, abnormal abdominal reflexes, rapid progression, or young onset should prompt a whole-spine MRI including the craniocervical junction rather than being treated as idiopathic. This recommendation is echoed across scoliosis research society teaching and national paediatric spine guidance worldwide.
- Decompress before fusing is the widely accepted sequence for a symptomatic Chiari with a syrinx and scoliosis. The supporting evidence is largely multicentre registry and meta-analysis level (for example the Park-Reeves Syringomyelia Research Consortium and a 2025 meta-analysis of 380 children) rather than randomised trials, so practice is guided by large observational series.
- Best candidates for a decompression-first strategy are younger children (under about 10) with smaller curves (35 to 40 degrees or less), who are most likely to stabilise or regress; older children and larger curves more often progress and need fusion regardless.
- It is the syrinx, not the tonsil descent, that predicts the spine problem - a point reinforced by data showing Chiari without a syrinx behaves largely like ordinary scoliosis. This shapes counselling and the threshold for intervention across centres globally.
- Neuropathic joints are managed cautiously everywhere: diagnose and treat the underlying syrinx, and avoid arthroplasty or arthrodesis where possible because of the high failure rate in an insensate joint.
Memory aids
LEFT PANAtypical Scoliosis Red Flags (image the neuraxis)
Hook:Turn LEFT and look for the PAN-neuraxis problem: a left curve with PAN (pathological reflexes, abnormal neurology, needs MRI) means scan the whole cord.
SCANWhy Orthopaedics Cares About Chiari
Hook:When you find Chiari, SCAN for the consequences: Syrinx, Curve, Arthropathy, Neurology.
DROPSurgical Sequence When Chiari + Syrinx + Scoliosis
Hook:DROP the tonsil pressure before you straighten the spine - Decompress, Reassess, Operate on the curve if needed, Protect the cord.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 11-year-old girl is referred with scoliosis. The radiograph shows a 35-degree LEFT thoracic curve. The examiner asks how you would assess and manage her.”
“A 45-year-old man presents with a grossly swollen, unstable right shoulder. Radiographs show severe bony destruction, but he reports almost no pain. How do you approach this?”
The Core Chain
- Chiari I = cerebellar tonsils 5mm or more below the foramen magnum
- Low tonsils obstruct CSF flow, so a syrinx forms in the cord
- The SYRINX (not tonsil descent) drives the orthopaedic problems
- Arnold-Chiari = type II, the one with spina bifida
Scoliosis Red Flags (image the neuraxis)
- LEFT thoracic curve
- Pain, neurological signs, abnormal abdominal reflexes
- Rapid progression and young age at onset
- Whole-spine MRI INCLUDING the craniocervical junction
Management Sequence
- Confirm with whole-neuraxis MRI; size the curve
- Posterior fossa decompression FIRST (often with duraplasty)
- Reassess: young/small curves may stabilise or improve; syrinx shrinks
- Posterior spinal fusion if the curve still progresses (about 38% do)
Neuropathic (Charcot) Joint
- Cervical syrinx removes pain/temperature in the arms (cape, dissociated)
- Painless, swollen, destroyed shoulder or elbow
- Syringomyelia: upper limb; diabetes: foot; tabes: knee/hip
- Treat the syrinx; avoid joint surgery (high failure rate)
Evidence
According to PubMed, the modern literature on Chiari and the spine is dominated by large paediatric series and a recent meta-analysis. The recurring themes are that the syrinx drives scoliosis, that younger age and smaller curves do best after decompression, and that Chiari without a syrinx behaves much more benignly.
Decompression Improves or Stabilises Scoliosis in Nearly Half of Children (Meta-Analysis)
- Systematic review and meta-analysis of 11 studies and 380 paediatric Chiari I patients with scoliosis who had posterior fossa decompression first; syringomyelia present in 92.6%
- After decompression, 55% of curves improved or stabilised while 45% progressed; the syrinx improved in 94%
- Younger age at surgery and a smaller baseline Cobb angle independently predicted a better curve outcome
- Ultimately 37.8% of patients still required spinal fusion
Younger Age and Smaller Curves Regress After Decompression (Park-Reeves Consortium)
- Large multicentre registry of children with Chiari I and a syrinx; 30.4% had scoliosis at diagnosis
- Among those decompressed with follow-up imaging, 39% improved, 22% stayed stable, and 39% progressed
- For curves of 35 degrees or less, only 17% of children under 10 progressed versus 64% of those aged 10 or older
- Tonsil position, baseline syrinx size, and craniocervical alignment did not predict the change in curve magnitude
Syrinx Side Matches Curve Convexity and Shrinks After Decompression
- Retrospective cohort of 42 patients with Chiari I, syringomyelia, and scoliosis treated with posterior fossa decompression
- Curves were atypical in 83% of cases, unlike idiopathic scoliosis
- The side of the syrinx significantly correlated with the convexity of the scoliosis, and the syrinx-to-cord ratio fell significantly after decompression
- Decompression alone stabilised curves of 40 degrees or less but not curves greater than 40 degrees
Chiari WITHOUT a Syrinx Has Minimal Effect on Scoliosis
- Retrospective review of 32 patients with scoliosis and Chiari I but NO syringomyelia
- In the non-surgical group the curve progressed by an average of only 1.0 degree
- Only 3 of 32 (9%) underwent posterior fossa decompression and only about a third went on to fusion
- No association was found between decompression and either curve progression or the need for fusion