Common, Superficial & Deep Peroneal (Fibular) Nerve Anatomy
Weak dorsiflexion and eversion; sensory loss over the dorsum of the foot / first web space. Inversion (tibialis posterior, tibial nerve) and ankle plantarflexion are PRESERVED. A positive Tinel sign at the fibular neck supports a peripheral lesion.
Also causes foot drop, but inversion is ALSO weak (tibialis posterior is L5 via the tibial nerve), as is hip abduction (gluteus medius). Back/radicular pain and a wider myotomal pattern point to the root rather than the peroneal nerve.
DEEPPeroneal Branches
Hook:Deep = Dorsiflexion + first-web sensation; Superficial = Eversion + dorsum of foot; the parent nerve is Perilous at the fibular neck.
Overview
The common peroneal nerve is examined more than any other lower-limb nerve because it is the cause of foot drop and because it is so easily injured — it sits subcutaneously on the fibular neck with no protection. The clean way to hold the topic is a two-branch split: the deep peroneal nerve lifts the foot and toes (and owns the first web space), while the superficial peroneal nerve turns the foot out (and owns the dorsum of the foot). Everything clinical flows from that — foot drop, the sensory map, the distinction from an L5 root lesion (which adds inversion and hip-abduction weakness), and the entrapment/surgical danger points down the leg.
Origin & Course
Origin
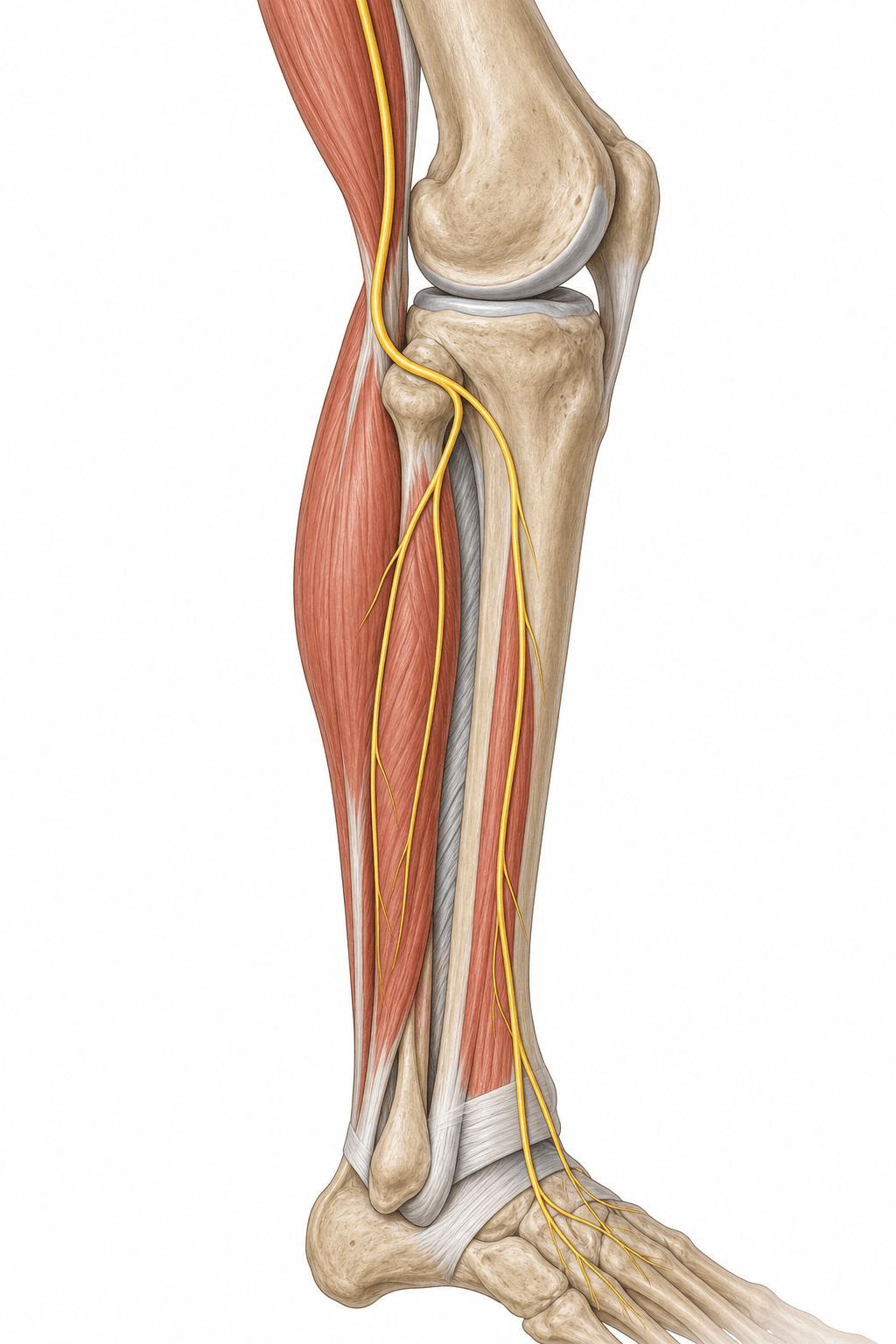
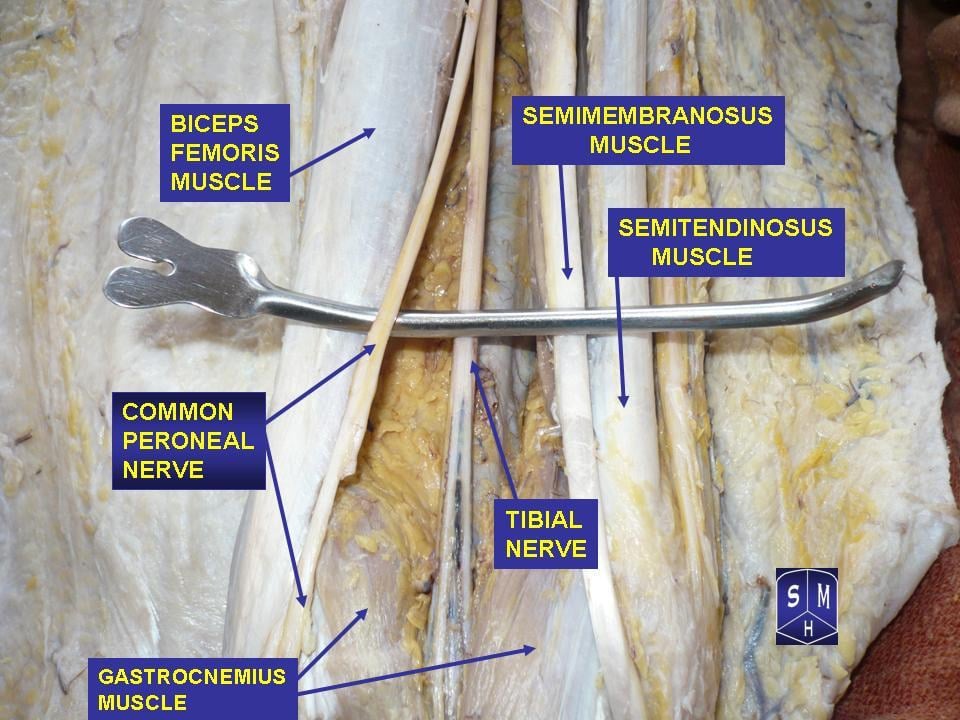
- The common peroneal (fibular) nerve is the smaller terminal branch of the sciatic nerve, carrying fibres from the posterior divisions of L4-S2.
- It separates from the tibial nerve at (or above) the apex of the popliteal fossa and runs along the medial border of biceps femoris toward the fibular head.
Innervation: Motor & Sensory Supply
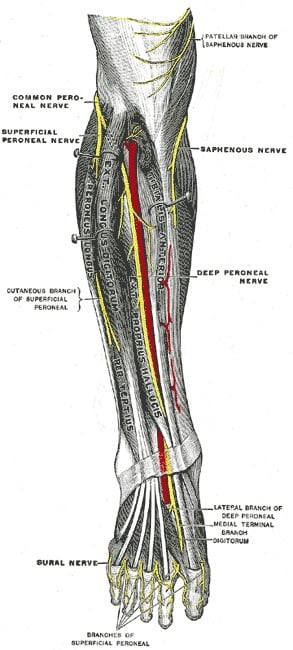
The deep peroneal nerve supplies the anterior compartment - tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius (and extensor digitorum brevis in the foot) - producing ankle dorsiflexion and toe extension. The superficial peroneal nerve supplies the lateral compartment - peroneus longus and brevis - producing foot eversion.
- Sensory (deep peroneal): a small but clinically vital zone in the first dorsal web space.
- Sensory (superficial peroneal): most of the dorsum of the foot (sparing the first web space and the lateral border, which is sural territory).
- Lateral sural cutaneous nerve: upper lateral leg, contributing to the sural nerve.
Inversion is the discriminatorFoot drop: is it peroneal or L5?
Hook:If the foot still inverts, it's the peroneal nerve; if inversion (and hip abduction) are also weak, it's the L5 root.
Clinical Correlations
Common Peroneal Palsy
- Foot drop - loss of dorsiflexion - with a compensatory high-steppage gait and weak eversion.
- Sensory loss over the dorsum of the foot and first web space.
- Plantarflexion and inversion are preserved (tibial nerve).
Distal Entrapments and Surgical Risk
Beyond the classic fibular-neck palsy, two distal entrapments and a set of operative danger points complete the examiner's picture.
- Superficial peroneal nerve entrapment. The superficial peroneal nerve becomes subcutaneous by piercing the deep fascia of the anterolateral leg about 10–12 cm above the lateral malleolus. It can be entrapped at this fascial exit (or by a fascial defect/muscle herniation, or after inversion ankle sprains), causing lateral leg / dorsal foot pain and altered sensation worse on activity — a cause of chronic exertional leg pain and a pitfall at lateral ankle arthroscopy portals.
- Deep peroneal nerve entrapment (anterior tarsal tunnel syndrome). The deep peroneal nerve can be compressed beneath the inferior extensor retinaculum at the ankle (tight footwear, osteophytes, ganglia), producing first-web-space numbness and, if the motor branch is involved, weakness/wasting of extensor digitorum brevis.
- Surgical danger at the fibular neck and proximal fibula. The subcutaneous course makes the nerve vulnerable in lateral approaches to the knee, proximal fibula resection/biopsy, high tibial osteotomy, multiligament knee reconstruction (PLC), and knee dislocation. It is also the graft/donor consideration site and the location of an intraneural ganglion arising from the superior tibiofibular joint (a recognised, recurrent cause of palsy).
- The peroneal nerves in the ankle block. Both terminal branches are anaesthetised as part of the five-nerve ankle block for foot surgery (the deep peroneal and superficial peroneal are two of the five, with the posterior tibial, sural and saphenous). The deep peroneal nerve is blocked at the front of the ankle between the tendons of tibialis anterior and extensor hallucis longus, just lateral to the dorsalis pedis (anterior tibial) artery, to anaesthetise the first web space; the superficial peroneal nerve is blocked by a subcutaneous ring across the dorsum of the ankle to cover the dorsum of the foot. Knowing which branch covers which territory tells you which to supplement when a block is patchy.
In roughly a fifth to a quarter of limbs an accessory deep peroneal nerve arises from the superficial peroneal nerve, runs down the lateral compartment and behind the lateral malleolus to supply part (or all) of extensor digitorum brevis (EDB). The consequences examiners probe:
- On nerve conduction studies the EDB response evoked by stimulating the deep peroneal nerve at the ankle is smaller than the response from stimulating below the fibular head (a paradoxical larger proximal CMAP) — the giveaway of an accessory deep peroneal nerve, not a technical error or conduction block.
- EDB may be partly preserved despite a deep peroneal lesion, so EDB wasting/function is an unreliable sole indicator of a deep peroneal palsy.
- It is the lower-limb counterpart of the hand's Martin-Gruber anastomosis as a classic innervation variant that confounds electrodiagnostic localisation — know it before you over-call or under-call a peroneal lesion.
For an irrecoverable foot drop the standard reconstruction is a tibialis posterior tendon transfer (rerouted through the interosseous membrane to the dorsum, often as a Bridle procedure incorporating tibialis anterior and peroneus longus) to restore active dorsiflexion — the classic "what if it doesn't recover?" follow-up.
Guidelines, Registries & Global Practice
Global Practice Picture
Common peroneal neuropathy is a universal clinical problem - the leading lower-limb compressive neuropathy and the prototypical cause of foot drop. Internationally consistent teaching: protect the fibular neck (positioning, casts), localise the lesion clinically (deep vs superficial branch; peroneal vs L5), confirm with electrodiagnostics, and manage with cause removal, an AFO, and decompression or tendon transfer when indicated.
Side-by-Side Synthesis
- Compartment / muscles
- Anterior (TA, EHL, EDL, per. tertius)
- Action
- Dorsiflexion, toe extension
- Sensory
- First web space
- Compartment / muscles
- Lateral (peroneus longus/brevis)
- Action
- Eversion
- Sensory
- Dorsum of foot (spares 1st web)
- Compartment / muscles
- (parent at fibular neck)
- Action
- Both of the above
- Sensory
- Lateral leg (sural contribution)
Evidence Base
Both references (checked against PubMed) are anatomical/clinical rather than outcome trials. McCool's cadaveric study confirms the entrapment mechanism — the deep fascia of peroneus longus compressing the nerve at the fibular neck, with release extended to the deep/superficial bifurcation — which is exactly the surgical anatomy you decompress. Bowley & Doughty situates common peroneal neuropathy within the foot-drop differential, reinforcing clinical localisation plus electrodiagnosis. For a viva the reproducible fibular-neck anatomy and the peroneal-versus-L5 discrimination matter more than either single paper.
Thread common peroneal nerve release-a cadaveric validation study
- Cadaveric validation (15 specimens) of an ultrasound-guided percutaneous 'thread' common peroneal nerve release at the fibular neck
- Confirms the nerve is compressed by the deep fascia of peroneus longus overlying it at the fibular neck
- Release extended to the bifurcation into the superficial and deep peroneal nerves
- No iatrogenic neurovascular or tendon injury; demonstrates the surgically relevant anatomy
Entrapment Neuropathies of the Lower Extremity
- Reviews lower-limb entrapment neuropathies including common peroneal neuropathy causing foot drop
- Emphasises accurate localisation to prevent pain, sensory loss and weakness affecting mobility
- Diagnosis combines clinical examination with electrodiagnosis and imaging
- Distinguishes peripheral peroneal palsy from other causes of foot drop