A Painless Right-Sided Mid-Clavicular Lump
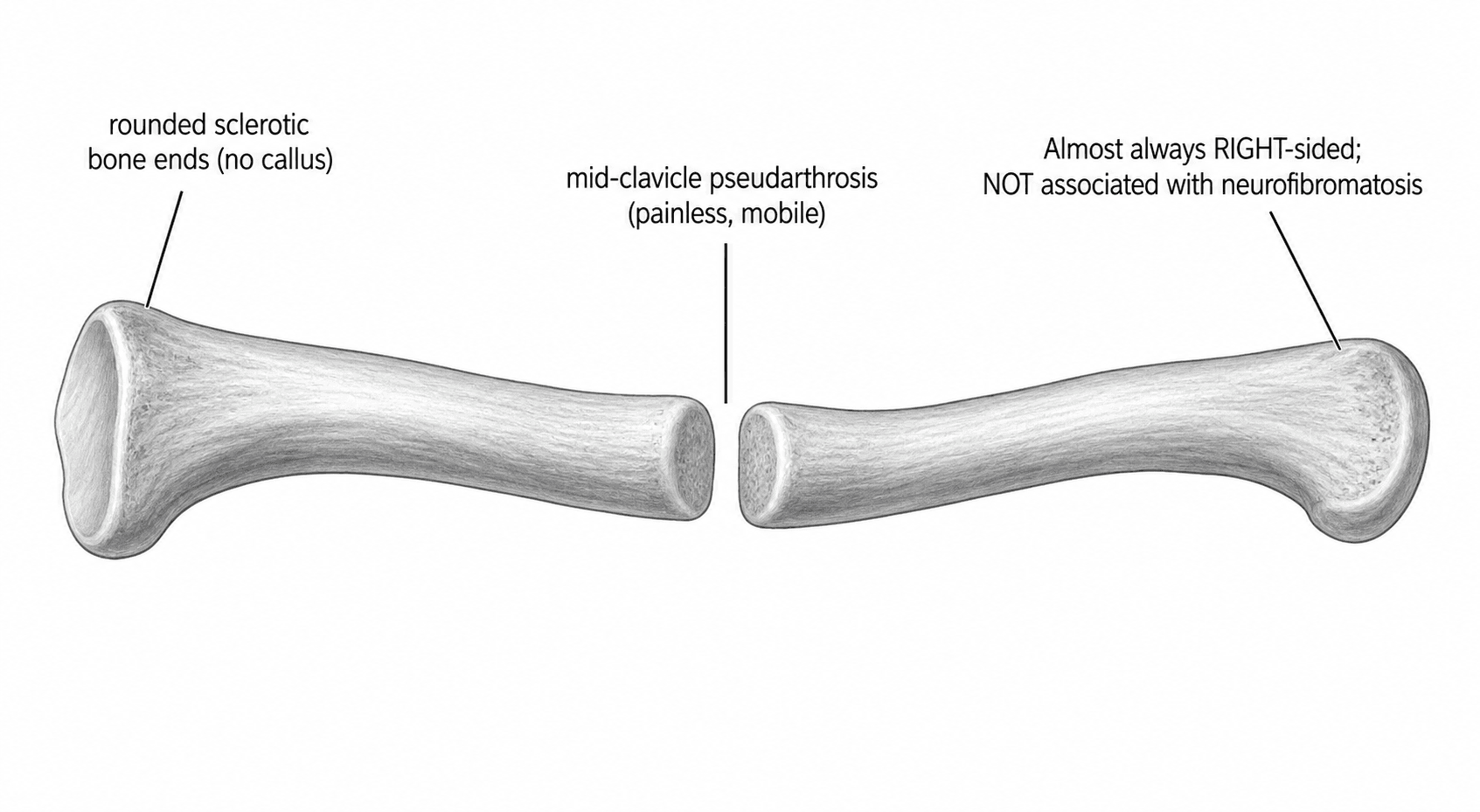
- Congenital pseudarthrosis of the clavicle (CPC) is a RARE disorder in which the medial and lateral ossification centres of the clavicle FAIL TO FUSE, producing a PAINLESS, mobile, non-tender LUMP over the MIDDLE THIRD of the clavicle, usually noticed in infancy/early childhood, with rounded SCLEROTIC non-united bone ends and NO callus on radiographs.
- It is almost ALWAYS RIGHT-SIDED; the rare LEFT-sided cases are associated with DEXTROCARDIA/situs inversus, and bilateral cases are uncommon - the right predominance is attributed to the higher position of the subclavian artery on the right (pulsation theory).
- Crucially, CPC is NOT associated with NEUROFIBROMATOSIS - this contrasts with congenital pseudarthrosis of the TIBIA, which IS strongly associated with NF1 and is far harder to treat; this distinction is a classic exam point.
- The main DIFFERENTIAL is a CLAVICLE BIRTH FRACTURE: a birth fracture follows trauma, is initially PAINFUL and HEALS with abundant CALLUS and simple immobilisation, whereas CPC is painless, present without trauma and does NOT heal spontaneously; the other differential is CLEIDOCRANIAL DYSPLASIA (BILATERAL clavicular defects with cranial/dental features, RUNX2 mutation).
- CPC is usually PAINLESS and NON-PROGRESSIVE with little or no functional deficit, so MANY cases can be simply OBSERVED; the indications for SURGERY are symptoms (pain, fatigue), cosmetic concern about the prominent lump, or functional problems, typically operated from around age 3-6 years.
- SURGICAL treatment is RESECTION of the pseudarthrosis with autologous (ILIAC CREST) bone grafting and internal FIXATION (plate, or elastic stable intramedullary nail/K-wire), which gives high union rates and good functional/cosmetic outcomes; AUTOGRAFT is preferred to allograft (allograft has higher non-union).
- “CPC = painless, mobile MID-clavicular lump from failed fusion of ossification centres; rounded sclerotic ends, no callus; almost always RIGHT-sided.
- “NOT associated with neurofibromatosis (vs congenital pseudarthrosis of the TIBIA, which IS). Left-sided CPC -> think situs inversus/dextrocardia.
- “Differentiate from birth fracture (painful, heals with callus) and cleidocranial dysplasia (bilateral + cranial/dental). Observe if asymptomatic; resection + iliac-crest autograft + fixation if symptomatic/cosmetic.
CPC is painless, present without trauma and does NOT heal; a clavicle birth fracture is initially painful, follows trauma and heals with callus on immobilisation.
CPC is NOT associated with neurofibromatosis and treats well; congenital tibial pseudarthrosis IS strongly NF1-associated and is notoriously difficult.
Presentation & Radiology
CPC results from failure of fusion of the medial and lateral clavicular ossification centres, presenting in infancy or early childhood as a painless, mobile, non-tender LUMP over the middle third of the clavicle. It is almost always RIGHT-sided; left-sided cases should prompt consideration of dextrocardia/situs inversus, and bilateral cases are rare. On radiographs the bone ends are rounded and sclerotic and non-united with NO callus - distinguishing it from a healing fracture. The condition is non-progressive with little functional deficit, and importantly it is NOT associated with neurofibromatosis (in contrast to congenital pseudarthrosis of the tibia).

Differential Diagnosis & Management
- Clavicle birth fracture: the main differential - it follows birth trauma, is initially painful, and HEALS with abundant callus and simple immobilisation; CPC is painless, atraumatic and does not heal.
- Cleidocranial dysplasia: suspect if the clavicular defects are BILATERAL or there are cranial features (delayed closure of fontanelles, Wormian bones), dental anomalies and other skeletal signs (a RUNX2 disorder).
- Neurofibromatosis: CPC is NOT associated with NF - but congenital pseudarthrosis of the tibia IS, so reserve NF concern for tibial (not clavicular) pseudarthrosis. Diagnosis is clinical (painless mid-clavicular mass) plus a radiograph showing the characteristic non-united rounded sclerotic ends.
- Observation: because CPC is usually painless, non-progressive and causes little functional deficit, many children need only reassurance and observation.
- Surgery (indications): symptoms (pain, shoulder fatigue), troublesome cosmetic prominence, or functional limitation - typically performed from around age 3-6 years.
- Technique: RESECTION of the pseudarthrosis with autologous ILIAC CREST bone grafting and internal FIXATION (a plate, or an elastic stable intramedullary nail / K-wire).
- Be honest about the union rate. Published series are small and range from roughly three-quarters to near-universal healing (see Evidence below) - so "it almost always unites" overstates it. Union is more reliable with autograft, and the reported failures cluster where allograft was used. Even where the bone fails to unite radiologically, operated children are typically pain-free with full movement, so the functional result and the radiographic result are not the same endpoint - a distinction worth making explicitly when consenting a family whose concern is usually cosmetic.
- Graft choice: AUTOGRAFT is preferred; allograft has a higher non-union rate. Intramedullary devices may achieve faster union and easier removal than plates.
Why It Happens: Clavicular Ossification and the Right Side
- The clavicle is unique: it is the first bone in the body to begin ossifying (around the fifth to sixth week of gestation) and ossifies largely by intramembranous ossification from two primary centres - a medial and a lateral - that normally coalesce in the mid-shaft (the bony ends then form by endochondral ossification, and the medial physis is the last in the body to fuse, in the early-mid twenties - relevant to medial physeal injuries, covered in our Clavicle Fractures topic).
- CPC is the failure of those two primary centres to coalesce - so the non-union sits in the middle third and is present without any trauma, with rounded sclerotic ends and no callus.
- Why the right: the subclavian artery sits higher on the right, just beneath the clavicle, and its pulsation is thought to disturb coalescence (the pulsation theory); on the left the artery is lower so CPC there occurs with dextrocardia/situs inversus (the mirrored arterial anatomy), and bilateral cases are associated with bilaterally elevated/anomalous subclavian arteries (e.g. cervical ribs). This is distinct from the general process of ossification (in our Intramembranous/Endochondral Ossification topic).
The clavicle is the first bone to ossify and forms by intramembranous ossification from two primary centres that normally coalesce - CPC is their failure to coalesce (mid-third, atraumatic). The right predominance is the subclavian-artery pulsation theory; left-sided → situs inversus; bilateral → anomalous/elevated subclavian arteries.
Operating Safely: What Lies Beneath, and When
Resection of the pseudarthrosis is carried out immediately superficial to the structures below, which is why a series reporting no neurovascular complications is making a substantive claim rather than a routine one:
- The anatomy at risk: directly beneath the middle third of the clavicle run the subclavian/axillary vessels and the brachial plexus (crossing over the first rib between the scalenes), with the lung apex medially - so a mid-clavicular resection is done with careful subperiosteal dissection, staying on bone and protecting these structures (full anatomy in our Brachial Plexus Anatomy topic).
- Why around age 3 to 6: old enough for safe anaesthesia and surgery and to harvest iliac-crest graft, yet young enough for good remodelling and union and before the lump or any functional/cosmetic concern becomes established; some surgeons favour earlier intervention for easier union and remodelling.
- If left untreated, the rare downsides: a prominent cosmetic lump, occasional aching/fatigue with activity or a drooping shoulder, and - rarely - thoracic-outlet-type symptoms from the bony prominence (see our Thoracic Outlet Syndrome topic); most, however, remain asymptomatic, which is why observation is legitimate.
Resecting a mid-clavicular pseudarthrosis means working directly over the subclavian/axillary vessels and brachial plexus - use careful subperiosteal dissection (the benchmark series reported no neurovascular complications). Operate around age 3 to 6 (safe surgery + graft, good remodelling); rarely, an untreated lump causes ache, droop or thoracic-outlet symptoms.
Mnemonics & Memory Aids
CLAVICLE
Hook:CPC of the CLAVICLE: painless right-sided lump, not NF, observe or graft.
NOT NF
Hook:Clavicular pseudarthrosis = NOT NF (that's the tibia).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An infant has a painless, mobile lump over the middle of the right clavicle. What is the likely diagnosis, what are the key differentials, and how would you manage it?”
“How does congenital pseudarthrosis of the clavicle differ from that of the tibia, and what does this mean for treatment and prognosis?”
What it is
- Failure of fusion of the clavicular ossification centres
- Painless, mobile, non-tender mid-clavicular lump from infancy
- Almost always RIGHT-sided (left -> dextrocardia/situs inversus)
Radiology & associations
- Rounded, sclerotic non-united bone ends; NO callus
- NOT associated with neurofibromatosis (vs congenital tibial pseudarthrosis)
- Non-progressive; little functional deficit
Differentials
- Clavicle birth fracture (painful, trauma, heals with callus)
- Cleidocranial dysplasia (bilateral + cranial/dental, RUNX2)
- Diagnosis: clinical + radiograph
Management
- Observe if asymptomatic (usually painless, good function)
- Surgery for symptoms/cosmesis (~age 3-6): resection + iliac-crest autograft + fixation
- Autograft > allograft (lower non-union); IM device gives faster union than plate
Evidence & Key Studies
Comparison of fixation methods in the treatment of congenital pseudarthrosis of the clavicle (multicentre)
- In 15 clavicles (11 children), pseudarthrosis resection with iliac crest bone autograft and fixation (plate vs elastic stable intramedullary nail/K-wires) achieved radiological healing in almost all.
- Elastic stable intramedullary nailing or K-wires achieved a shorter union time and easier implant removal than plates, with no difference in complications or clinical outcome.
- Surgical resection with iliac crest autograft is an effective treatment, and surgery is recommended for symptomatic congenital pseudarthrosis of the clavicle.
Congenital pseudarthrosis of the clavicle: a report on 27 cases
- In 27 cases, operated patients (mostly for cosmetic appearance) were treated by pseudarthrosis resection and K-wire fixation, usually with iliac crest autograft.
- Bone healing was achieved in 74%, all operated patients were pain-free with full range of motion, and no neurovascular complications occurred.
- Use of allograft was associated with a high non-union rate, so autologous iliac crest grafting gave better functional and cosmetic outcomes.
The effectiveness of resection plus iliac crest autograft and the comparison of fixation methods (intramedullary devices giving faster union) come from the cited Li multicentre study, and the good functional/cosmetic outcomes with autograft (and high non-union with allograft) from the cited Di Gennaro series. The painless right-sided presentation, the rounded non-united radiographic appearance, the non-association with neurofibromatosis and the distinction from a birth fracture and cleidocranial dysplasia are standard, well-established paediatric teaching. (See also our Clavicle Fractures, Cleidocranial Dysplasia and Congenital Tibial Pseudarthrosis topics.)