Facioscapulohumeral Muscular Dystrophy
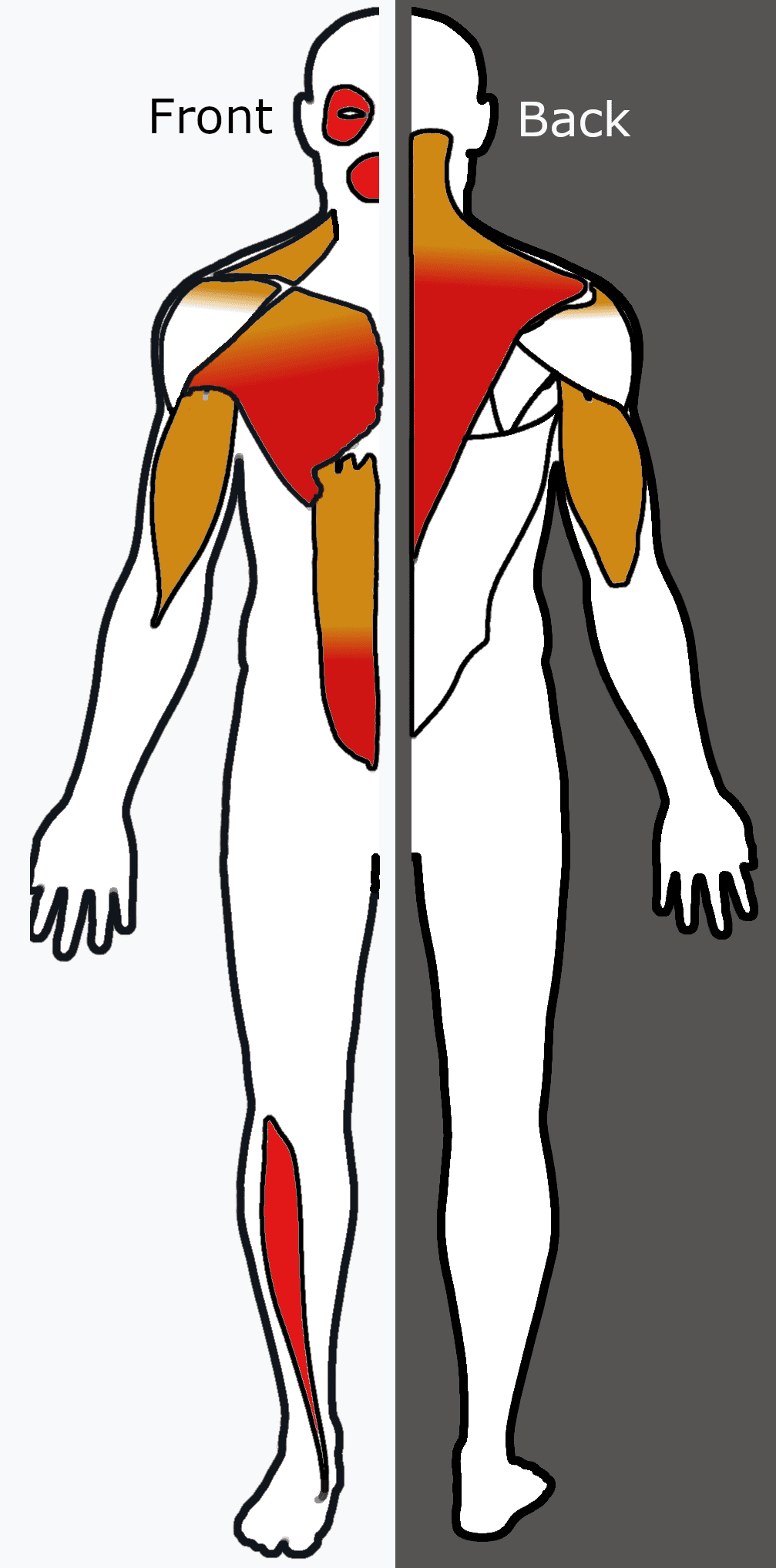
- FSHD is one of the most common muscular dystrophies (estimated prevalence around 1 in 15,000) and produces a characteristic DESCENDING, often ASYMMETRIC pattern of weakness - FACE first (difficulty whistling, drinking through a straw, burying the eyelashes on eye closure), then the SHOULDER GIRDLE / periscapular muscles (scapular winging), then the HUMERAL muscles (biceps/triceps wasting with relative forearm sparing, the 'Popeye arm'), with later trunk, abdominal (a positive Beevor's sign) and lower-limb (foot-drop) involvement.
- The genetic basis of the common form (FSHD1, around 95%) is a CONTRACTION of the D4Z4 macrosatellite repeat array on chromosome 4q35 on a 'permissive' (polyadenylation-enabling) haplotype, which relaxes the chromatin and allows aberrant expression of the normally silenced DUX4 gene; DUX4 protein is toxic to skeletal muscle. Inheritance is AUTOSOMAL DOMINANT (with variable penetrance); FSHD2 is a rarer digenic form usually involving SMCHD1.
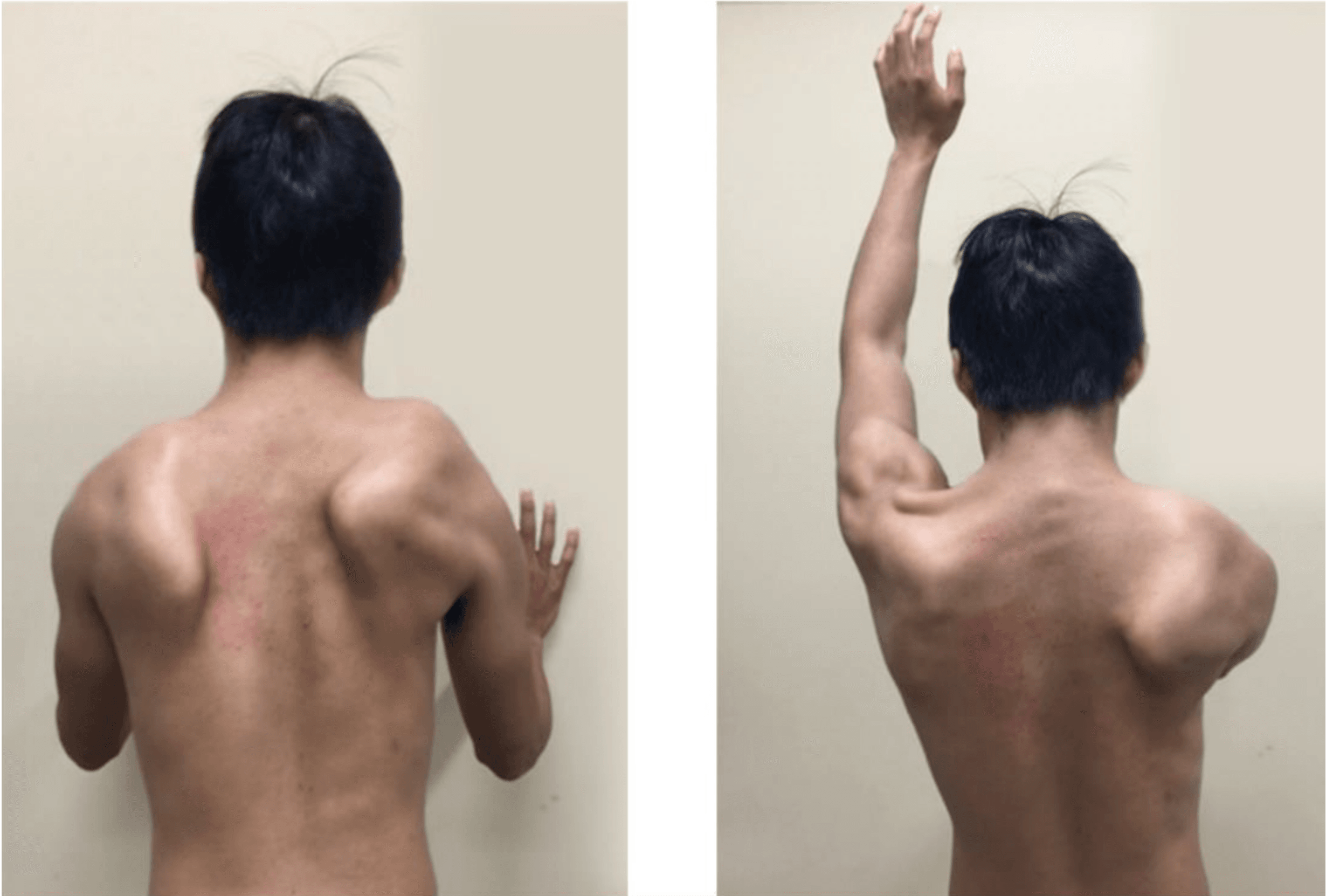
- The principal ORTHOPAEDIC problem is SCAPULAR WINGING: weakness of the scapular stabilisers (serratus anterior, trapezius, rhomboids) lets the scapula ride up and wing, so glenohumeral abduction/flexion is wasted because the scapula is not stabilised on the chest wall - patients often have surprisingly preserved DELTOID power that cannot be used effectively.
- SCAPULOTHORACIC ARTHRODESIS (STA) is the established surgical treatment for severe symptomatic winging when the DELTOID is preserved: fusing the scapula to the ribs gives the deltoid a stable platform, and regardless of the specific fixation technique (multifilament cables alone, or cables/cerclage combined with plates, ideally with autograft) it reliably improves active shoulder elevation and quality of life.
- STA has recognised COMPLICATIONS: PULMONARY complications (pleural effusion, pneumothorax, atelectasis) are common because of the thoracic dissection but usually resolve spontaneously, and there are fixation-related scapular complications (related to the surgeon's learning curve); meticulous technique, careful positioning of the fusion (around 20-30 degrees of scapular abduction), and good postoperative analgesia reduce these.
- There is no disease-modifying cure yet, so care is SUPPORTIVE and MULTIDISCIPLINARY (neurology, genetics, orthopaedics, physiotherapy, respiratory, ophthalmology for the rare retinal vasculopathy/Coats disease and audiology for sensorineural hearing loss); patient selection - preserved deltoid, realistic goals, acceptable respiratory reserve - is the key determinant of a good surgical outcome.
- “FSHD = DESCENDING facio-scapulo-humeral weakness, often ASYMMETRIC; face -> periscapular (winging) -> biceps (Popeye arm, forearm spared); FSHD1 = 4q35 D4Z4 contraction -> DUX4, autosomal dominant.
- “Winging is from weak scapular stabilisers; DELTOID is often PRESERVED but unusable without a stable scapula.
- “Scapulothoracic arthrodesis (STA) is indicated for severe winging with PRESERVED deltoid; improves elevation; pulmonary complications common but usually self-limiting.
Descending, asymmetric weakness: face -> periscapular (winging) -> biceps (Popeye arm, forearm spared) -> trunk/lower limb (foot-drop). FSHD1 = 4q35 D4Z4 contraction -> DUX4.
Scapulothoracic arthrodesis for severe winging when the deltoid is preserved - it gives the deltoid a stable base and restores active elevation.
Pattern of Weakness & Genetics
FSHD is one of the most common muscular dystrophies (estimated prevalence around 1 in 15,000) and weakens muscles in a descending facioscapulohumeral pattern that is characteristically asymmetric. It begins in the face (difficulty whistling, drinking through a straw, or burying the eyelashes), moves to the shoulder girdle / periscapular muscles (producing scapular winging), then the humeral muscles (biceps and triceps wasting with relative sparing of the forearm - the 'Popeye arm'), and later involves the trunk (a positive Beevor's sign, where the umbilicus moves upward on neck flexion) and the lower limb (foot-drop). The common form, FSHD1 (around 95%), is caused by a contraction of the D4Z4 macrosatellite repeats on chromosome 4q35 on a permissive haplotype, which relaxes the chromatin and allows aberrant expression of the normally silenced DUX4 gene; DUX4 protein is toxic to muscle. Inheritance is autosomal dominant, and a rarer digenic FSHD2 (usually SMCHD1) shares the phenotype.
Scapular Winging & Scapulothoracic Arthrodesis
The principal orthopaedic problem is scapular winging. Weakness of the scapular stabilisers (serratus anterior, trapezius, rhomboids) means the scapula is not anchored to the chest wall, so when the deltoid contracts the scapula simply rotates and wings rather than acting as a stable base for glenohumeral elevation - the result is severely limited active abduction and flexion despite a frequently well-preserved deltoid. Scapulothoracic arthrodesis (STA) addresses exactly this: by fusing the scapula to the ribs it converts the unstable scapula into a fixed platform, allowing the preserved deltoid to elevate the arm. Regardless of the specific fixation (multifilament cables alone, or cables/cerclage wires combined with plates, ideally with autograft), STA reliably improves active elevation and quality of life - so the operation hinges on selecting patients with severe symptomatic winging and a preserved deltoid.
Two points govern scapulothoracic arthrodesis. First, the deltoid must be PRESERVED - STA gives the deltoid a stable platform, so if the deltoid itself is weak the operation will not restore useful elevation, making careful assessment of deltoid power an essential part of patient selection. Second, STA involves thoracic dissection and rib fixation, so PULMONARY complications (pleural effusion, pneumothorax, atelectasis) are common - they usually resolve spontaneously, but the patient's respiratory reserve should be assessed beforehand and good postoperative analgesia and chest physiotherapy provided. Because FSHD is a systemic neuromuscular disorder, surgery should always sit within multidisciplinary care with realistic, shared goals.
Predicting the result before you commit to it
"Assess the deltoid" is only useful if you know how. The manoeuvre below does at the bedside exactly what the operation does surgically, so the arc achieved with the scapula held is a direct rehearsal of the arc the patient can expect afterwards - which makes it worth more than any imaging in the selection decision.
- 1Observe unaided
Stand behind the seated patient and watch active elevation in the scapular plane.
Record the arc reached and the degree of winging as the baseline.
- 2Stabilise the scapula
Press the scapula firmly against the chest wall, holding the medial border and inferior angle down - this reproduces by hand what the arthrodesis does surgically.
- 3Re-test elevation
With the scapula still held, ask the patient to elevate again, and grade deltoid power against resistance.
Compare the two arcs directly.
- 4Interpret
A substantial improvement - often from below shoulder height to at or above it - means a preserved deltoid working against an unstable base.
IMPROVES: arthrodesis should convert that power into useful elevation. NO CHANGE: the deltoid itself is the problem, and fusing the scapula converts a mobile useless shoulder into a stiff useless one.
This is what "preserved deltoid" actually means in practice, and it is the single most useful part of the assessment - a patient who fails it should be counselled away from the operation regardless of how dramatic the winging looks.
What arthrodesis delivers - and what it does not
The operation is worth doing and the results are genuinely good, but the counselling has to be specific, because the trade is a real one.
- It does not make anything stronger. It converts existing deltoid power into useful motion by removing the wasted scapular excursion. No muscle is improved.
- It caps the arc. Scapulohumeral rhythm normally contributes roughly a third of elevation, and fusion deliberately abolishes the scapulothoracic component. The realistic endpoint is therefore useful function around or a little above shoulder height rather than full overhead elevation - in the best-documented bilateral series, active forward elevation improved from 62 to 102 degrees and abduction from 58 to 89.
- It does not alter the disease. FSHD continues to progress, and a deltoid that weakens later will erode the gain, which is an argument for operating while deltoid power is good rather than waiting until function is desperate.
- What it does do well is abolish the painful, prominent, cosmetically distressing winging and restore hand-to-face and hand-to-table function - in that same series the Subjective Shoulder Value rose from 25% to 72%, and every patient said they would recommend it.
The respiratory question, read honestly
The concern that fusing the scapula to the ribs splints the chest wall is theoretical but reasonable, particularly in a disease that itself causes restrictive impairment and when both sides are done. The best available data are reassuring - with bilateral, sequentially performed fusions there was no significant change in vital capacity - but two caveats belong with that reassurance. The series comprised five patients, which is far too small to exclude a clinically meaningful effect, and within it the forced vital capacity fell numerically from 86% to 77% of predicted. The practical position is therefore not "respiratory function is unaffected" but: obtain baseline pulmonary function tests, treat poor reserve as a genuine selection issue, stage the two sides rather than doing them together, and plan analgesia and chest physiotherapy that let the patient breathe deeply afterwards.
The Rest of the Orthopaedic Care
The shoulder dominates the exam, but it is not the whole of what an orthopaedic surgeon contributes.
- Foot drop from tibialis anterior weakness is managed with an ankle-foot orthosis. Tendon transfer is generally inappropriate: the donor is itself dystrophic and will weaken, so a transfer that works initially fails as the disease advances - the same logic that rules out tendon transfers around the scapula and sends those patients to fusion instead.
- Contractures, particularly of the Achilles tendon, are managed with stretching and orthoses, with surgical release reserved for a contracture that is genuinely blocking function.
- Lumbar hyperlordosis is characteristic and follows abdominal and paraspinal weakness; scoliosis occurs but is far less prominent than in the dystrophinopathies. Bracing is poorly tolerated where respiratory function is already reduced.
- Exercise is safe and beneficial, and this corrects older advice. Moderate aerobic activity and submaximal strength training improve function without accelerating muscle damage; what genuinely harms these patients is deconditioning and prolonged immobilisation, so post-operative and post-injury plans should minimise time immobilised.
- Anaesthesia: FSHD carries no established association with malignant hyperthermia, unlike some other myopathies, so it is not a reason to avoid volatile agents on that basis - but respiratory reserve, positioning and post-operative pulmonary care do require planning.
How FSHD Is Diagnosed
Diagnosis is the clinical pattern - descending, asymmetric facioscapulohumeral weakness - confirmed by genetic testing. For FSHD1 the test must show a contracted D4Z4 repeat array on chromosome 4q35 and that it sits on a permissive (4qA) haplotype - the haplotype that supplies the polyadenylation signal stabilising the DUX4 transcript. Both the contraction and the permissive haplotype are required: a contraction on a non-permissive haplotype does not cause disease. FSHD2 (D4Z4 hypomethylation without a contraction, usually SMCHD1) needs methylation and SMCHD1 analysis.
Supporting tests place FSHD among the dystrophies but do not make the diagnosis:
- Creatine kinase (CK) is normal or only mildly raised - unlike the very high CK of dystrophinopathies - so a normal CK does not exclude FSHD.
- EMG is myopathic; muscle biopsy is non-specific and usually unnecessary now that genetic testing is available.
- Muscle MRI shows the characteristic selective, asymmetric pattern of fatty muscle replacement (and can guide a biopsy if one is ever needed).
There is a specific trap in biopsying these patients. FSHD muscle frequently contains an inflammatory infiltrate, so a biopsy taken without the clinical pattern in mind is readily reported as an inflammatory myopathy - and the patient is then committed to immunosuppression that cannot work and carries real harm. The face is the safeguard: an inflammatory myopathy does not produce the facial weakness, the asymmetry or the family history, so look for lagophthalmos and a transverse smile before accepting a diagnosis of polymyositis in someone whose real problem is a scapular dystrophy.
Diagnose by the clinical pattern plus genetics: a contracted D4Z4 array on a permissive 4qA haplotype (FSHD1). CK is normal or only mildly raised (does not exclude it), EMG myopathic, biopsy usually unnecessary, and MRI shows selective asymmetric involvement.
Beyond Muscle: Extra-Muscular Features & Severity
- Retinal vasculopathy - peripheral retinal telangiectasia, occasionally progressing to an exudative Coats-like retinopathy that can threaten vision (ophthalmology screening, especially in severe/early disease).
- Sensorineural hearing loss - notably in infantile-onset disease; screen children so it does not impair speech and development.
- Restrictive respiratory involvement in advanced disease - the reason to assess respiratory reserve before scapulothoracic arthrodesis.
- Cardiac involvement/atrial arrhythmia is uncommon (far less than in dystrophinopathies or myotonic dystrophy), so routine intensive cardiac surveillance is not generally required.
There is a genotype-severity correlation: a shorter residual D4Z4 array (fewer repeats) generally means earlier onset and more severe disease, including the severe infantile-onset form in which the extra-muscular features (Coats retinopathy, hearing loss) and rapid progression are most common - so repeat size guides surveillance and counselling (tempered by the variable penetrance and somatic mosaicism noted above).
FSHD has extra-muscular features: retinal vasculopathy / Coats-like retinopathy, sensorineural hearing loss (especially infantile-onset), restrictive respiratory disease (assess before STA), and uncommon cardiac involvement. A shorter D4Z4 repeat means earlier onset and more severe disease - so screen the eyes and hearing in early/severe cases.
Mnemonics & Memory Aids
FSHD
Hook:FSHD: Face, Scapula (winging), Humeral (Popeye arm), DUX4 - descending, asymmetric, dominant.
STA
Hook:STA: Severe winging, Thoracic fixation (pulmonary risk), Active elevation restored (deltoid preserved).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young adult presents with scapular winging and difficulty lifting the arms, with facial weakness. What is the likely diagnosis and what is the underlying genetics?”
“When would you offer scapulothoracic arthrodesis in FSHD, and what would you warn the patient about?”
Pattern
- Descending, asymmetric: face -> periscapular (winging) -> humeral (Popeye arm, forearm spared)
- Later: trunk (Beevor's sign), lower limb (foot-drop)
- Prevalence ~1/15,000; onset commonly facial then shoulder-girdle
Genetics
- FSHD1 (~95%): D4Z4 contraction on 4q35 (permissive haplotype) -> DUX4 de-repression
- DUX4 protein is toxic to muscle; autosomal dominant (variable penetrance)
- FSHD2: rarer, digenic (usually SMCHD1)
Orthopaedic problem
- Scapular winging from weak serratus anterior/trapezius/rhomboids
- Deltoid often preserved but unusable without a stable scapula
- Limited active abduction/flexion
Scapulothoracic arthrodesis
- Indication: severe symptomatic winging with PRESERVED deltoid
- Fuse scapula to ribs (~20-30 deg abduction); cables +/- plates, autograft
- Improves elevation/QoL; pulmonary complications common but usually self-limiting; MDT care
Evidence & Key Studies
Management of scapular dysfunction in FSHD: biomechanics of winging, arthrodesis indications, techniques and outcomes
- FSHD typically causes scapular winging due to wasting of the periscapular muscles; scapulothoracic arthrodesis (STA) is the current surgical treatment for severe winging with a preserved deltoid.
- Several fixation techniques exist (multifilament cables alone, or cables/cerclage wires combined with single or multiple plates); the authors prefer cables without plates and strongly recommend autograft. Regardless of technique, shoulder elevation and quality of life improve on outcome scores.
- Pulmonary complications are common but usually resolve spontaneously; scapular fixation complications relate to the surgeon's learning curve. Success strongly depends on patient selection and a multidisciplinary team (neurologists, geneticists, orthopaedic surgeons).
The UK FSHD patient registry: prevalence, genetics and presenting features
- FSHD is estimated to affect about 1 in 15,000 people; in the UK registry most patients (91.7%) had FSHD type 1.
- Facial weakness was the most prevalent symptom at onset (59.2%), followed by shoulder-girdle weakness (53.3%), then distal (22.4%) or proximal lower-limb (14.8%) weakness.
- Most patients (85.6%) were ambulant or ambulant with assistance, and 7.9% reported respiratory insufficiency.
Bilateral scapulothoracic arthrodesis for FSHD: function, fusion and respiratory consequences
- 10 sequentially performed scapulothoracic arthrodeses in 5 FSHD patients (semitubular plate and wire construct with iliac crest autograft), mean follow-up 141 months: bony union in 90% (9 of 10), with one pneumothorax and one pleural effusion as the only early complications and no reoperations.
- Active forward elevation improved from 62 to 102 degrees and abduction from 58 to 89 degrees, with the Subjective Shoulder Value rising from 25% to 72%; all patients would recommend the procedure.
- Pulmonary function showed no significant change in vital capacity (87% to 85% predicted), though forced vital capacity fell numerically from 86% to 77% predicted.
The orthopaedic facts - scapular winging from periscapular wasting, scapulothoracic arthrodesis as the treatment for severe winging with a preserved deltoid, the fixation techniques and use of autograft, the improvement in elevation/quality of life, and the common (usually self-limiting) pulmonary complications - come from the cited Eren EFORT review; the prevalence (~1/15,000), the predominance of FSHD1, and the onset pattern (face then shoulder-girdle then lower limb) with the respiratory-insufficiency figure from the cited Evangelista registry. The 4q35 D4Z4/DUX4 genetics, the descending asymmetric phenotype (Popeye arm, Beevor's sign, foot-drop) and the supportive multidisciplinary framework are standard, well- established teaching. The fusion rate, the elevation and Subjective Shoulder Value gains, and the pulmonary function results come from the cited Boileau series. (See also Scapular Winging, which sets FSHD against the nerve-palsy causes and their tendon transfers, and Long Thoracic Nerve Anatomy.)