The Unstable Scapula
- Most winging is neurogenic: serratus anterior (medial) or trapezius (lateral).
- The long thoracic nerve comes from roots C5, C6 and C7 (remember Bell - C5/6/7).
- Wall push-up test brings out medial winging; resisted abduction brings out lateral winging.
- Most neurogenic palsy recovers spontaneously - give conservative care for around 12 to 24 months before salvage surgery.
- “Painful onset with patchy shoulder-girdle weakness suggests neuralgic amyotrophy (Parsonage-Turner).
- “Pectoralis major (sternal head) transfer is the salvage of choice for fixed serratus anterior palsy.
- “Eden-Lange transfer (levator scapulae + both rhomboids) is the salvage for fixed trapezius palsy.
Overview
Scapular winging: abnormal protrusion of the scapula away from the chest wall because the muscles that hold it flat and rotate it (mainly serratus anterior and trapezius) are weak, detached, or imbalanced.
The scapula is the stable platform from which the arm works. Normal overhead elevation needs smooth scapulothoracic rhythm - the scapula rotating upward as the arm rises. If a key stabiliser fails, the scapula lifts off the chest wall, the shoulder loses power and elevation, and the patient develops pain and fatigue. The two classic neurogenic patterns are medial winging (serratus anterior) and lateral winging (trapezius). Less commonly, direct muscle avulsion or rhomboid (dorsal scapular nerve) weakness is responsible.
According to PubMed, the most common causes are dysfunction of the serratus anterior from long thoracic nerve injury (medial winging) or dysfunction of the trapezius from spinal accessory nerve injury (lateral winging), but acute traumatic tears of serratus anterior, trapezius and rhomboids are under-recognised causes (Didesch and Tang, 2018; DOI).
Functional Anatomy and Clinical Appearance



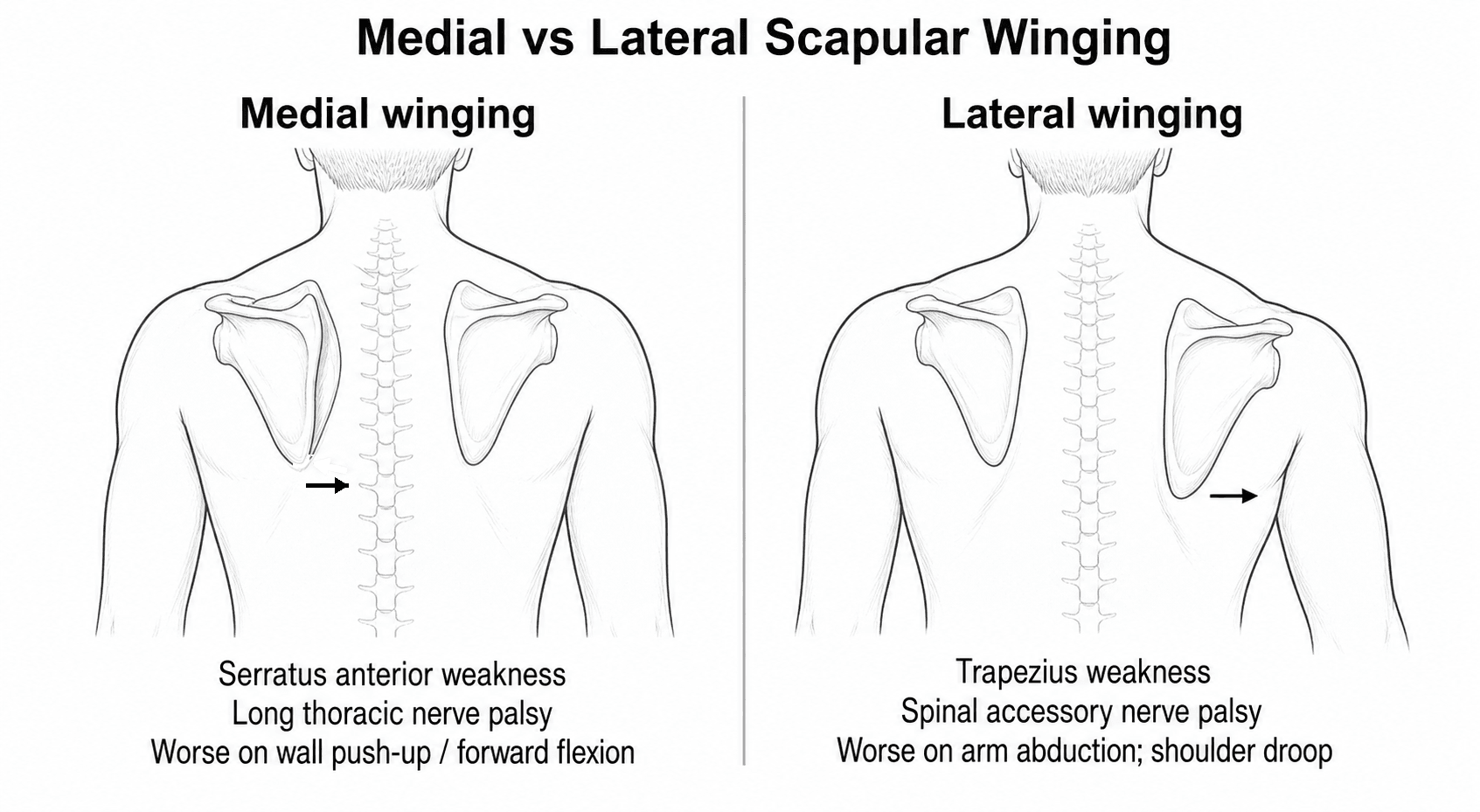
Direction tells you the nerve Medial winging (scapula towards the spine, worse on forward push) = serratus anterior / long thoracic nerve. Lateral winging (scapula slides out and droops, worse on abduction) = trapezius / spinal accessory nerve.
The neck biopsy story A drooping shoulder and winging after a lymph node biopsy or neck dissection is spinal accessory nerve injury until proven otherwise. Examine the posterior triangle scar.
Anatomy
Serratus Anterior and the Long Thoracic Nerve
- Origin/insertion: Arises from the upper 8 or 9 ribs, wraps around the chest wall, and inserts on the deep surface of the medial scapular border.
- Action: Protracts the scapula and, crucially, produces upward rotation so the glenoid faces up for overhead reach. It also holds the medial border flat against the thorax.
- Nerve: Long thoracic nerve (the nerve of Bell), roots C5, C6, C7. It runs superficially on the surface of serratus anterior, making it vulnerable to traction and direct trauma.
- Failure: Loss produces medial winging - the medial border lifts off and drifts towards the spine, and forward elevation is limited and weak.
Pathophysiology
How the Nerves Get Injured
- Traction (sudden depression of the shoulder, sport, heavy lifting) and the long superficial course make it vulnerable.
- Compression by a backpack ("rucksack palsy").
- Often there is no clear injury - an inflammatory neuritis (neuralgic amyotrophy) is increasingly recognised.
- Most commonly iatrogenic - cervical lymph node biopsy, excision in the posterior triangle, or neck dissection.
- Penetrating or blunt trauma to the posterior triangle.
According to PubMed, the spinal accessory nerve's superficial course in the posterior cervical triangle makes it susceptible to injury, and iatrogenic injury after a surgical procedure is one of the most common causes of trapezius palsy (Wiater and Bigliani, 1999).
Classification
Medial vs Lateral (the working classification)
- Medial (dynamic) winging: Serratus anterior palsy. Inferior angle rotates towards the midline; winging worst on forward flexion / wall push-up.
- Lateral winging: Trapezius palsy. Scapula translates laterally, inferior angle rotates outward, shoulder droops; winging worst on abduction.
- This direction-based split is the most useful clinically because it points straight to the nerve.
Scapular Dyskinesis and the Kibler Classification
Not every abnormal scapula is a true (structural or neurogenic) winging. Scapular dyskinesis is altered scapular position and movement - usually a problem of muscle control, timing and overuse rather than a fixed nerve or muscle lesion - and it is the commonest scapular abnormality in overhead athletes. It matters because it contributes to subacromial impingement, rotator cuff overload and instability, and because it is treated with rehabilitation, not surgery.
Kibler described a visual classification by which part of the scapula is most prominent.
- Prominent border
- Inferior angle prominent (tilts dorsally)
- Underlying fault
- Loss of anterior-tilt control (often serratus / lower trapezius)
- Prominent border
- Whole medial border prominent
- Underlying fault
- Excess internal rotation about a vertical axis
- Prominent border
- Superomedial border prominent (shrug pattern)
- Underlying fault
- Early or excess superior translation
- Prominent border
- Symmetric, normal
- Underlying fault
- Reference (normal) pattern
The SICK scapula describes an overuse dyskinesis in throwers - Scapular malposition, Inferior medial border prominence, Coracoid pain and malposition, and dysKinesis. The scapular assistance and scapular retraction tests help judge whether the dyskinesis is driving impingement or instability. Most dyskinesis responds to a graded scapular-stabilisation programme.
Scapular dyskinesis is abnormal scapular motion and control (Kibler types I to III, and the SICK scapula in throwers) and is treated with rehabilitation. Reserve the label "winging" for a structural cause - a serratus or trapezius palsy, or a muscle or bony lesion - confirmed by direction and EMG.
Snapping Scapula Syndrome (Scapulothoracic Bursitis)
Snapping scapula syndrome is painful, audible or palpable crepitus during scapulothoracic motion, sometimes with pseudo-winging, caused by mechanical incongruity between the scapula and the chest wall. It is a key mechanical mimic to separate from neurogenic winging because the nerves and EMG are normal.
The scapulothoracic articulation has two main bursae - the infraserratus bursa (between serratus anterior and the chest wall) and the supraserratus bursa (between subscapularis and serratus anterior) - plus smaller adventitial bursae at the superomedial and inferior angles, any of which can inflame.
- Detail
- Osteochondroma (commonest), Luschka's tubercle at the superomedial angle, scapular or rib malunion
- Action
- CT to define; excise the lesion
- Detail
- Scapulothoracic bursitis, muscle atrophy or fibrosis
- Action
- Physiotherapy, posture correction, NSAIDs, bursal steroid injection
- Detail
- Persistent painful crepitus despite conservative care
- Action
- Bursectomy and superomedial angle resection (open or arthroscopic)
Painful scapulothoracic crepitus with normal nerves is snapping scapula syndrome; look for an osteochondroma or a Luschka's tubercle on CT. Treat most cases with physiotherapy and a bursal injection, reserving bursectomy and superomedial angle resection for refractory disease.
Clinical Assessment
Ask about onset (sudden painful onset suggests neuralgic amyotrophy), recent neck surgery or biopsy (accessory nerve), trauma, backpack use, and sport (archery, tennis, swimming, weightlifting). Ask what the patient cannot do - overhead work and pushing are typically affected.
Look from behind with the patient relaxed and then provoke. Note a drooping shoulder and asymmetric neckline (trapezius) versus a flat-resting scapula that wings on push (serratus).
- Wall push-up test: The patient pushes against a wall - medial winging of serratus palsy is exaggerated.
- Forward flexion / arm raise: Brings out medial (serratus) winging.
- Resisted abduction / shoulder shrug: Brings out lateral (trapezius) winging and reveals trapezius weakness.
- Medial Winging (Serratus)
- Long thoracic (C5-7)
- Lateral Winging (Trapezius)
- Spinal accessory (CN XI)
- Medial Winging (Serratus)
- Medial border up, towards spine
- Lateral Winging (Trapezius)
- Translated lateral, shoulder droops
- Medial Winging (Serratus)
- Forward flexion / wall push-up
- Lateral Winging (Trapezius)
- Abduction / shrug
- Medial Winging (Serratus)
- Traction, sport, neuritis
- Lateral Winging (Trapezius)
- Neck biopsy / dissection (iatrogenic)
Investigations
- EMG / nerve conduction studies confirm the diagnosis, localise the lesion (serratus vs trapezius vs rhomboids), grade severity, and - on serial testing - detect reinnervation, which guides timing of surgery.
- Needle EMG of serratus anterior or trapezius shows denervation in neurogenic palsy.
- Plain radiographs / CT: Exclude bony causes (osteochondroma, malunion) and pseudo-winging.
- MRI: Useful for muscle atrophy, mass lesions, and increasingly for nerve pathology - high-resolution imaging and ultrasound can show hourglass-like constrictions in neuralgic amyotrophy.
- High-resolution ultrasound: Dynamic assessment of the nerve and muscle; identifies constrictions in neuralgic amyotrophy.
According to PubMed, improved MRI and high-resolution ultrasound have identified pathognomonic hourglass-like nerve constrictions in neuralgic amyotrophy, which has shifted the condition from a purely clinical diagnosis towards imaging-guided diagnosis and, in selected cases, surgery (Gstoettner et al., 2020; DOI).
Differential Diagnosis
The classic trap is calling every protruding scapula "serratus palsy". Always decide the direction of winging first, then look for the cause.
- Distinguishing Feature
- Medial winging, worse on push-up, inferior angle to midline
- Key Test
- EMG serratus; long thoracic nerve
- Distinguishing Feature
- Lateral winging, drooping shoulder, neck scar
- Key Test
- EMG trapezius; accessory nerve
- Distinguishing Feature
- Subtle medial winging, inferior angle rotated laterally
- Key Test
- EMG rhomboids
- Distinguishing Feature
- Severe pain first, then patchy weakness, often bilateral/post-viral
- Key Test
- MRI/US nerve constrictions; EMG
- Distinguishing Feature
- Bilateral, facial weakness, family history, young patient
- Key Test
- Genetic testing, CK, EMG
- Distinguishing Feature
- Painful crepitus, pseudo-winging, no denervation
- Key Test
- CT scapula (bony lesion)
- Distinguishing Feature
- Reproducible on demand, painless, normal nerves
- Key Test
- Normal EMG; psychological assessment
Bilateral, symmetric winging with facial weakness in a young patient is FSHD, not a nerve injury. And a painful, sudden-onset palsy that does not respect a single nerve - especially after a viral illness or vaccination - is neuralgic amyotrophy, which is treated very differently from a simple traction palsy.
Management Algorithm
Conservative Management (first line for neurogenic palsy)
- Why: Most neurogenic winging recovers spontaneously - the traditional teaching is recovery within around 2 years for long thoracic nerve palsy.
- What: Physiotherapy (scapular stabiliser strengthening, range of motion to avoid stiffness), activity modification, and analgesia.
- Bracing: Scapulothoracic orthoses are described but are often poorly tolerated.
- Duration: Continue for roughly 12 to 24 months with serial clinical and EMG review for reinnervation before considering salvage.
According to PubMed, most patients with serratus palsy regain function with conservative treatment, although recovery may take up to 2 years, and bracing is often poorly tolerated (Wiater and Flatow, 1999).
Medial winging that will not recover to pectoralis major transfer. Lateral winging that will not recover to Eden-Lange. Dystrophic muscle (FSHD) to scapulothoracic fusion.
Surgical Technique
Pectoralis Major Transfer (for serratus palsy)
- Goal: Replace the lost upward-rotation and stabilising pull of serratus anterior.
- Principle: The sternal head of pectoralis major is mobilised and transferred to the inferior angle of the scapula, usually lengthened with an autograft (fascia lata, hamstring) to reach.
- Steps:
- Two-incision approach (anterior axillary fold and over the inferior scapular angle).
- Harvest the sternal head of pectoralis major.
- Lengthen with fascial/tendon graft if needed.
- Pass deep to the chest wall soft tissue to the inferior angle.
- Fix to the scapula and tension with the arm at the side.
According to PubMed, transfer of the sternal head of pectoralis major to the inferior angle of the scapula reinforced with fascia or tendon autograft consistently improves function, eliminates winging and reduces pain (Wiater and Flatow, 1999; Galano et al., 2008; DOI).
Complications
Missed or Wrong Diagnosis
- Calling lateral (trapezius) winging "serratus palsy" sends the surgeon to the wrong operation.
- Missing FSHD or neuralgic amyotrophy leads to inappropriate early surgery.
Always confirm the direction of winging and back it with EMG.
Postoperative Care
- Sling/abduction support after tendon transfer to protect the repair.
- Gentle passive range of motion to avoid stiffness; no active loading of the transfer.
- Begin active scapular control and assisted elevation.
- Start retraining the transferred muscle to fire in its new role.
- Progressive strengthening and return to function.
- Heavy lifting and sport deferred until the transfer is strong and winging is controlled.
Clinical Relevance and Prognosis
- Spontaneous recovery is common in neurogenic palsy - the natural history justifies patience before salvage surgery.
- But not everyone recovers fully: residual winging, weakness and fatigability persist in a meaningful proportion, which is why a proactive nerve-surgery approach is gaining ground for persistent cases.
- Timing is everything for nerve surgery: the best outcomes for neurolysis or repair come within around 12 months.
- Salvage works: pectoralis transfer (serratus) and Eden-Lange (trapezius) reliably reduce pain and winging and improve function in fixed palsy.
According to PubMed, the older view that almost all long thoracic nerve palsies recover within 2 years is an oversimplification - a significant percentage retain residual winging and weakness, and decompression beyond 12 months can still yield satisfactory results (Wu and Ng, 2023; DOI).
Guidelines, Registries and Global Practice
Global Epidemiology
- Serratus anterior palsy (long thoracic nerve) is the most common cause of true scapular winging, typically affecting active young adults through traction, sport or neuritis.
- Trapezius palsy (spinal accessory nerve) is most often iatrogenic, following posterior triangle neck surgery or lymph node biopsy.
- Neuralgic amyotrophy is now recognised as more common than historically assumed, often post-viral or post-vaccination, and frequently underlies "idiopathic" winging.
Side-by-Side Practice Comparison
- Serratus (Long Thoracic)
- Medial
- Trapezius (Spinal Accessory)
- Lateral
- FSHD (Myopathy)
- Bilateral / mixed
- Serratus (Long Thoracic)
- Conservative ~12 to 24 months
- Trapezius (Spinal Accessory)
- Early nerve repair if recent injury
- FSHD (Myopathy)
- Genetic dx, supportive
- Serratus (Long Thoracic)
- Neurolysis if refractory
- Trapezius (Spinal Accessory)
- Repair/graft within ~12 months
- FSHD (Myopathy)
- Not applicable
- Serratus (Long Thoracic)
- Pectoralis major transfer
- Trapezius (Spinal Accessory)
- Eden-Lange transfer
- FSHD (Myopathy)
- Scapulothoracic arthrodesis
Practice Variation: High vs Limited Resource Settings
- High-resource: Routine EMG, high-resolution ultrasound and MRI for nerve constrictions, microsurgical nerve repair and the full range of tendon transfers and fusion.
- Limited-resource: Diagnosis is often clinical (direction of winging plus provocation tests); conservative rehabilitation is the mainstay, and tendon transfers or fusion deliver high value where microsurgical nerve reconstruction is unavailable.
- Across all settings: Skilled physiotherapy for scapular stabilisation and a watchful period for spontaneous recovery are emphasised before any salvage surgery.
Memory Aids
Bell 567Long Thoracic Nerve Roots
Hook:The nerve of Bell rings at 5-6-7: C5, C6, C7 raise your arm above 7 (heaven).
TRAPCauses of Winging
Hook:A heavy TRAP on the shoulder wings the scapula.
LRREden-Lange Transfer
Hook:LRR rebuilds the three pulls of the lost trapezius for fixed lateral winging.
MCQ Practice Points
Q: What are the root values of the long thoracic nerve? A: C5, C6 and C7 (the nerve of Bell).
Q: Medial winging worse on a wall push-up indicates weakness of which muscle? A: Serratus anterior (long thoracic nerve palsy).
Q: Lateral winging with a drooping shoulder after posterior triangle neck surgery suggests injury to which nerve? A: The spinal accessory nerve (cranial nerve XI), causing trapezius palsy.
Q: What is the salvage tendon transfer for fixed serratus anterior palsy? A: Transfer of the sternal head of pectoralis major to the inferior angle of the scapula (often with a fascial/tendon graft).
Q: Which muscles are transferred in the Eden-Lange procedure? A: Levator scapulae, rhomboid minor and rhomboid major, moved laterally to recreate the trapezius vectors.
Q: What imaging finding is now considered a hallmark of neuralgic amyotrophy? A: Hourglass-like nerve constrictions on high-resolution MRI or ultrasound.
Additional Quiz Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old recreational tennis player has aching and weakness reaching overhead for 3 months. From behind, the right scapula sits flat at rest but the medial border lifts off and drifts towards the spine when he pushes against the wall.”
“A 45-year-old woman has a drooping right shoulder, pain and difficulty abducting the arm six months after an excisional lymph node biopsy in the posterior triangle of the neck. The scapula sits laterally and droops; winging worsens on abduction.”
“A 22-year-old man has slowly progressive bilateral scapular winging and difficulty raising both arms. On closer look he has mild facial weakness and cannot fully close his eyes. His father had similar shoulder problems.”
Pattern Recognition
- Medial winging, worse on push-up = serratus / long thoracic (C5-7)
- Lateral winging, drooping shoulder = trapezius / spinal accessory (XI)
- Subtle medial winging, angle rotated out = rhomboids / dorsal scapular
- Bilateral + facial weakness = FSHD
Causes (TRAP)
- Trauma / Traction
- Rucksack / Repetitive sport
- Amyotrophy (neuralgic / Parsonage-Turner)
- Postsurgical (neck biopsy - accessory nerve)
Investigations
- EMG / NCS - confirm, localise, grade, follow reinnervation
- MRI / ultrasound - muscle atrophy and nerve constrictions
- CT - exclude bony / snapping scapula
Treatment Ladder
- Conservative physio for ~12 to 24 months (neurogenic)
- Nerve surgery (neurolysis / repair) ideally within 12 months
- Serratus salvage: pectoralis major transfer
- Trapezius salvage: Eden-Lange; FSHD: scapulothoracic fusion
Evidence Base
Anatomy, Etiology, and Management of Scapular Winging (Review)
- Comprehensive review of anatomy, etiology, evaluation and treatment of scapular winging
- Most common causes: serratus anterior dysfunction from long thoracic nerve injury (medial winging) and trapezius dysfunction from spinal accessory nerve injury (lateral winging)
- Acute traumatic tears of serratus anterior, trapezius and rhomboids are under-recognised causes
- Distinguishes management of neurogenic winging from traumatic muscular detachment