A COL2A1 Type II Collagenopathy
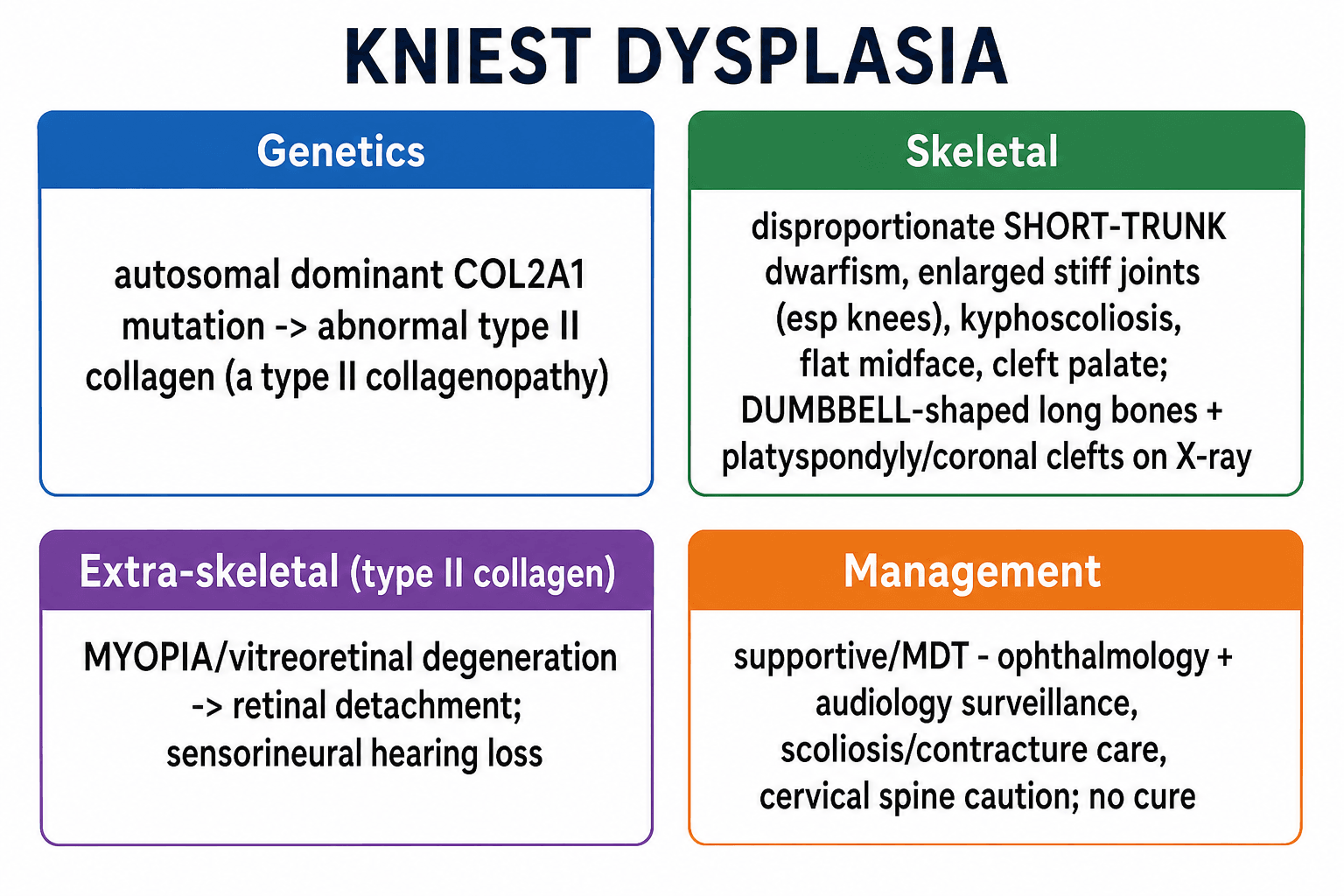
- Kniest dysplasia is an AUTOSOMAL DOMINANT skeletal dysplasia caused by a mutation in COL2A1, making it a TYPE II COLLAGENOPATHY - type II collagen is the principal collagen of cartilage, the vitreous body of the eye, the nucleus pulposus and the inner ear, which explains the combination of skeletal, ocular and auditory features.
- The SKELETAL phenotype is a disproportionate SHORT-TRUNK dwarfism with ENLARGED, STIFF joints (especially the knees) and contractures, kyphoscoliosis, a flat midface with a depressed nasal bridge, and often a CLEFT PALATE; radiographs show 'DUMBBELL'-shaped long bones (broad metaphyses), platyspondyly and coronal clefts of the vertebrae, with the histological 'Swiss-cheese' cartilage of large chondrocyte lacunae.
- The EXTRA-SKELETAL features arise because type II collagen is also in the eye and ear: high MYOPIA with vitreoretinal degeneration carries a significant risk of RETINAL DETACHMENT (requiring ophthalmology surveillance), and there is sensorineural and/or conductive HEARING LOSS - so eye and ear assessment is an essential part of care.
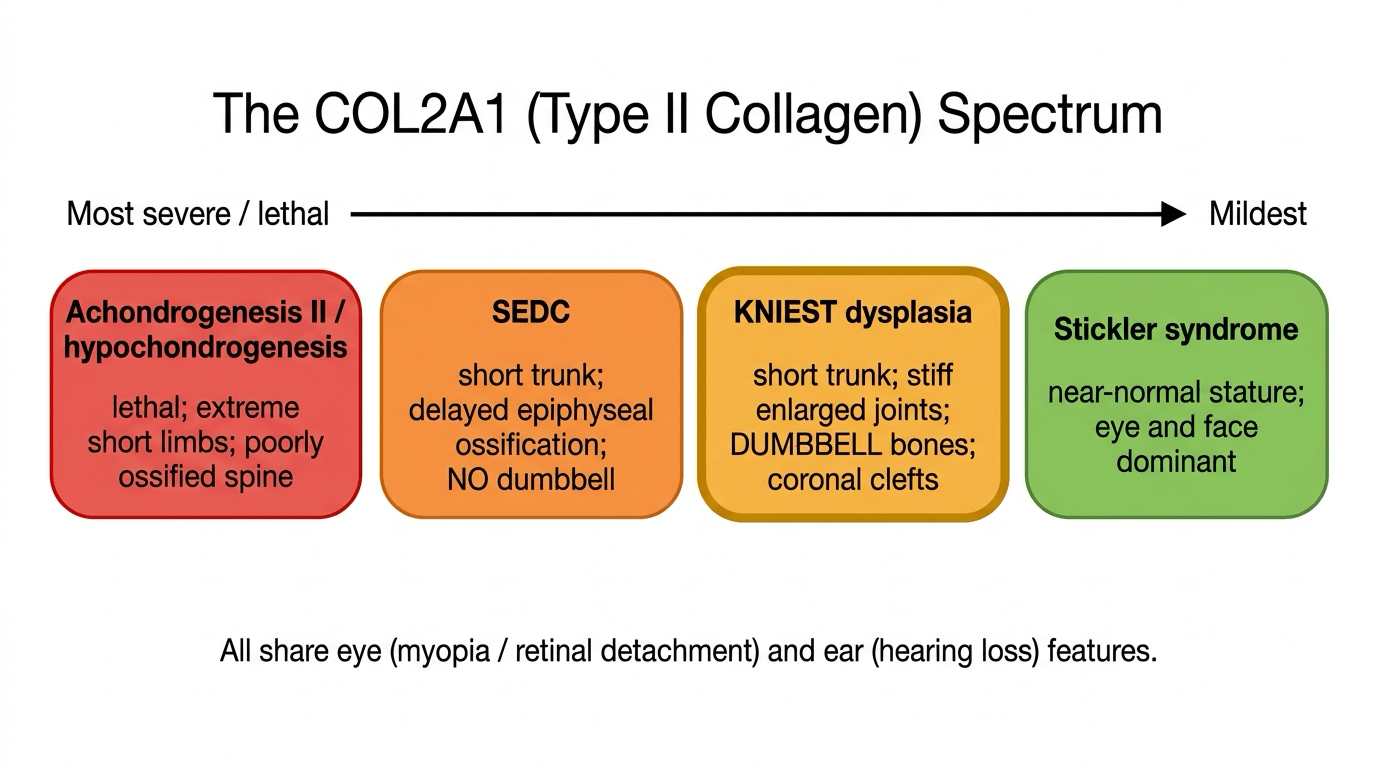
- Kniest dysplasia sits within the COL2A1 SPECTRUM of type II collagenopathies, which ranges (in decreasing severity) from achondrogenesis type II and hypochondrogenesis (often lethal) through spondyloepiphyseal dysplasia congenita (SEDC) and Kniest dysplasia to the milder STICKLER syndrome - radiologically it is in the 'Kniest-Stickler' group characterised by dumbbell tubular-bone deformities.
- Important ORTHOPAEDIC/ANAESTHETIC considerations include progressive kyphoscoliosis and joint contractures, early osteoarthritis, and the possibility of CERVICAL-SPINE instability (odontoid/atlantoaxial issues seen in type II collagenopathies), which - together with the midface/airway features - make anaesthesia hazardous and warrant cervical-spine assessment before any procedure.
- There is NO cure; management is SUPPORTIVE and MULTIDISCIPLINARY - regular OPHTHALMOLOGY surveillance (to prevent/treat retinal detachment), AUDIOLOGY, management of scoliosis and joint contractures, cleft palate repair, respiratory monitoring, cervical-spine assessment, and genetic counselling for the autosomal dominant inheritance.
- “Kniest dysplasia = AD COL2A1 TYPE II collagenopathy: short-trunk dwarfism, enlarged stiff joints, dumbbell long bones, platyspondyly/coronal clefts.
- “Type II collagen is in eye + ear -> high MYOPIA/RETINAL DETACHMENT and hearing loss (surveillance needed).
- “Part of the COL2A1 spectrum (achondrogenesis II -> SEDC -> Kniest -> Stickler). No cure; supportive MDT; beware cervical-spine instability/anaesthesia.
AD COL2A1 disorder: short-trunk dwarfism, enlarged stiff joints, kyphoscoliosis, dumbbell long bones and platyspondyly.
Type II collagen is in the eye and ear -> myopia/vitreoretinal degeneration with RETINAL DETACHMENT and hearing loss - surveillance is essential.
Genetics, Phenotype & Spectrum
Kniest dysplasia results from an autosomal dominant mutation in COL2A1, the gene for type II collagen - the dominant collagen of cartilage, the vitreous of the eye, the nucleus pulposus and the inner ear. This single shared collagen explains why the disorder combines a skeletal phenotype with eye and ear disease. The skeleton shows a disproportionate short-trunk dwarfism with enlarged, stiff joints (especially the knees), contractures, kyphoscoliosis, a flat midface and often a cleft palate; radiographs show 'dumbbell' long bones, platyspondyly and coronal vertebral clefts, with characteristic 'Swiss-cheese' cartilage histology. Kniest dysplasia is part of the COL2A1 spectrum (achondrogenesis type II -> hypochondrogenesis -> SEDC -> Kniest -> Stickler, in decreasing severity), and radiologically belongs to the 'Kniest-Stickler' group with dumbbell tubular-bone deformities.
Molecular Pathophysiology: Why a COL2A1 Defect Does This
Abnormal type II collagen, autosomal dominant inheritance and the 'Swiss-cheese' cartilage are linked by one mechanism - dominant-negative - and it is worth being able to explain it.
- The mutations. Kniest-causing variants cluster in the part of COL2A1 that encodes the triple-helical domain of pro-alpha-1(II) collagen, and are characteristically in-frame - small deletions or splice-site mutations that cause exon skipping. The result is a shortened but still-incorporated mutant alpha chain (not an absent one).
- Why dominant, not recessive. Type II collagen is a homotrimer of three alpha-1(II) chains, so even one mutant chain per molecule corrupts the triple helix - a single abnormal allele poisons the assembly of collagen made from the normal allele as well (a dominant-negative or "protein suicide" effect). This is why a heterozygous mutation produces disease, in contrast to loss-of-function variants that can give the milder, haploinsufficiency-type Stickler phenotype.
- From molecule to histology. Mis-assembled type II collagen disrupts the cartilage fibrillar network, so the growth-plate and epiphyseal cartilage is structurally weak and laden with dilated chondrocyte lacunae - the 'Swiss-cheese' cartilage seen histologically - which translates into the disordered enchondral growth (broad metaphyses/dumbbell bones, platyspondyly) and the soft, enlarged, stiff joints. The same defective type II collagen in the vitreous and inner ear produces the myopia/retinal detachment and hearing loss.
The one-line mechanism: an in-frame COL2A1 mutation makes a shortened alpha-1(II) chain that is built into the homotrimeric triple helix and acts dominant-negatively, wrecking the cartilage matrix ('Swiss-cheese' cartilage) and the type-II-collagen tissues of the eye and ear. Contrast this with loss-of-function COL2A1 variants (haploinsufficiency), which tend toward the milder Stickler end. (Type II collagen biology is developed further in Proteoglycans & Collagen and Skeletal Dysplasias.)
Differential Diagnosis: Placing Kniest in the COL2A1 Spectrum
Kniest sits within the COL2A1 spectrum, and the examinable skill is distinguishing it from the Stickler and SEDC groups. All three are COL2A1 collagenopathies sharing the eye (myopia/retinal detachment) and ear (hearing loss) features; they separate on stature, joints and the radiographic pattern.
- Discriminating features
- Short-trunk dwarfism with ENLARGED, STIFF joints and contractures (esp knees); 'dumbbell' tubular bones, platyspondyly with CORONAL clefts; 'Swiss-cheese' cartilage; cleft palate, flat midface
- What confirms or excludes it
- COL2A1 sequencing with the radiographic triad of dumbbell bones, coronal clefts and stiff enlarged joints
- Discriminating features
- Also short-trunk and COL2A1, but DELAYED epiphyseal ossification (absent or late femoral-head and pubic ossification), 'pear-shaped' vertebrae and NO dumbbell deformity
- What confirms or excludes it
- The skeletal survey separates them; then flexion-extension cervical views, because odontoid hypoplasia and atlantoaxial instability are the danger here
- Discriminating features
- Mildest COL2A1 or COL11 end: near-NORMAL stature with predominantly OCULAR (high myopia, retinal detachment) and orofacial (Pierre Robin sequence, cleft, flat midface) disease, hearing loss and early osteoarthritis
- What confirms or excludes it
- Normal stature with a normal or near-normal skeletal survey; refer for ophthalmology and audiology rather than more radiographs
- Discriminating features
- The severe, often LETHAL end of the COL2A1 spectrum: extreme micromelia, poorly ossified spine and pelvis
- What confirms or excludes it
- Presents perinatally; antenatal ultrasound and postnatal radiographs showing absent vertebral ossification
- Discriminating features
- Not COL2A1: metatropic has a dumbbell look too but with later kyphoscoliosis and a coccygeal tail; Morquio brings corneal clouding with normal intellect
- What confirms or excludes it
- URINARY GLYCOSAMINOGLYCANS - send them if the COL2A1 spectrum does not fit, because a mucopolysaccharidosis is a metabolic diagnosis with its own treatment
Each of these is developed separately in skeletal dysplasias, Stickler syndrome, the mucopolysaccharidoses, diastrophic dysplasia and short-rib thoracic dysplasias including metatropic.
Within COL2A1: Kniest = short trunk + stiff enlarged joints + dumbbell bones + coronal clefts; SEDC = short trunk but pear-shaped vertebrae / delayed ossification, no dumbbell; Stickler = near-normal stature, eye/face dominant. If stature is normal think Stickler; if the joints are big and stiff with dumbbell bones think Kniest; if there is delayed epiphyseal ossification with pear-shaped vertebrae think SEDC.
Clinical Care & Management
There is no cure, so management is supportive and multidisciplinary:
- Ophthalmology surveillance: regular review for high myopia and vitreoretinal degeneration to detect and treat (or prevent) RETINAL DETACHMENT - a major preventable cause of visual loss.
- Audiology: monitor and manage sensorineural/conductive hearing loss.
- Orthopaedic care: manage scoliosis and joint contractures, anticipate early osteoarthritis, and address limb/joint problems; assess and protect the cervical spine (instability/odontoid issues).
- Airway/anaesthesia: midface hypoplasia, cleft palate and possible cervical instability make airway management and anaesthesia hazardous - plan carefully and avoid forced neck manipulation.
- Other: cleft palate repair, respiratory monitoring, and genetic counselling (autosomal dominant).
Screening the cervical spine: what to request and what the numbers mean
"Assess the cervical spine before any procedure" needs a method attached, because this is the one instruction whose omission can cost a cord.
Request lateral cervical radiographs in flexion and extension, supervised and taken actively by the child rather than forced, plus an open-mouth odontoid view. MRI is added where there are neurological symptoms, an abnormal radiographic measurement, or a plan for major surgery, since it shows the cord itself and any signal change. Two measurements matter:
- Atlantodens interval (ADI) - anterior arch of C1 to the front of the dens. Normal is under 3 mm in an adult and under 5 mm in a child; more than 5 mm indicates incompetence of the restraint between C1 and the dens.
- Space available for the cord (SAC, or posterior ADI) - back of the dens to the anterior edge of the posterior C1 arch. Under 14 mm means the cord is at risk, and this is the more important number, because it measures the space the cord actually has. Steel's rule of thirds - a third dens, a third cord, a third spare - is the reason a large ADI is tolerated until the spare third is used up.
Surgical stabilisation is indicated absolutely by neurological symptoms or myelopathy, and relatively by an ADI over 10 mm, a SAC under 14 mm, or documented progressive instability; posterior C1-C2 fusion is the standard operation. The thresholds and technique are set out in Atlantoaxial Instability.
One mechanistic distinction is worth holding. In Down syndrome the instability is ligamentous - a lax transverse ligament with a normal dens. In the skeletal dysplasias it is usually osseous: a hypoplastic or absent odontoid, or an os odontoideum, so the restraint fails because there is nothing for the ligament to hold. That matters because odontoid hypoplasia does not improve with growth and is not excluded by a normal-looking neutral lateral film - it has to be looked for.
Planning the anaesthetic
The airway and the neck are separate problems that arrive together, and the plan follows from that:
- Anticipate a difficult airway from midface hypoplasia, a repaired or unrepaired cleft palate, a short neck and restricted mouth opening - and plan for it rather than discovering it, with a senior anaesthetist and difficult-airway equipment available.
- Protect the neck throughout. Avoid forced extension for laryngoscopy and during positioning and transfer; an awake or videolaryngoscopic technique with manual in-line stabilisation is preferable where instability is documented or unassessed.
- Expect restrictive lung physiology from the short trunk and kyphoscoliosis, which lowers the threshold for post-operative respiratory support and makes prolonged procedures less well tolerated.
- Position carefully. Stiff, enlarged joints with fixed contractures do not tolerate being forced into a standard position, and the same collagen defect makes the skin and soft tissues vulnerable to pressure.
Two points are easy to miss and important: first, because Kniest dysplasia is a type II collagenopathy, the patient has high myopia and vitreoretinal degeneration with a real risk of RETINAL DETACHMENT, so lifelong ophthalmology surveillance is essential to preserve vision; second, like other type II collagenopathies it can involve the upper cervical spine with odontoid/atlantoaxial instability, which - together with the midface and airway features - makes anaesthesia and any forced neck movement hazardous, so the cervical spine should be assessed before procedures. Recognising Kniest as a systemic collagen disorder rather than a purely skeletal one is the key to safe, comprehensive care.
Mnemonics & Memory Aids
KNIEST
Hook:KNIEST: COL2A1 short-trunk dysplasia with stiff joints, eye and ear disease, dumbbell bones.
COL2 SPECTRUM
Hook:COL2A1 spectrum, severe to mild: Achondrogenesis II - SEDC - Kniest - Stickler.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is Kniest dysplasia, and why does it affect the eyes and ears as well as the skeleton?”
“What are the key management and anaesthetic considerations in Kniest dysplasia?”
Genetics
- Autosomal dominant COL2A1 mutation -> abnormal type II collagen
- Type II collagen: cartilage, vitreous, nucleus pulposus, inner ear
- Part of COL2A1 spectrum (achondrogenesis II - SEDC - Kniest - Stickler)
Skeletal phenotype
- Disproportionate short-trunk dwarfism; enlarged stiff joints (knees), contractures
- Kyphoscoliosis, flat midface, cleft palate
- Radiographs: dumbbell long bones, platyspondyly, coronal vertebral clefts; 'Swiss-cheese' cartilage
Extra-skeletal
- High myopia / vitreoretinal degeneration -> RETINAL DETACHMENT (surveillance)
- Sensorineural/conductive hearing loss
- Recognise as a systemic collagen disorder
Management & caution
- No cure; supportive MDT (ophthalmology + audiology surveillance)
- Scoliosis/contracture/early-OA care; cleft repair; respiratory monitoring
- Cervical-spine instability + midface -> hazardous anaesthesia (assess spine); genetic counselling
Evidence & Key Studies
Radiologic features of type II and type XI collagenopathies (Kniest-Stickler group)
- COL2A1 pathogenic variants cause abnormal type II collagen and a group of skeletal dysplasias (type II collagenopathies), commonly associated with vitreoretinal degeneration and hearing impairment.
- These divide radiologically into the SEDC group (pear-shaped vertebrae) and the KNIEST-STICKLER group, characterised by disordered tubular bone growth producing 'dumbbell' deformities.
- Kniest dysplasia belongs to the Kniest-Stickler group; recognising the radiographic pattern guides diagnosis and multidisciplinary care.
Stickler syndrome, a COL2A1 collagenopathy in the spectrum with Kniest dysplasia and achondrogenesis type II: a three-case report
- Heterozygous COL2A1 defects cause a continuous spectrum of disorders affecting cartilage and bone, including Kniest dysplasia, achondrogenesis type II and Stickler syndrome type 1.
- These collagenopathies share ocular, auditory, musculoskeletal and orofacial manifestations.
- The shared COL2A1 basis explains the overlapping skeletal and extra-skeletal (eye/ear) features across the spectrum.
The COL2A1/type-II-collagenopathy basis, the 'dumbbell' Kniest-Stickler radiographic group and the association with vitreoretinal degeneration and hearing impairment come from the cited Handa review, and the COL2A1 spectrum (Kniest, achondrogenesis type II, Stickler) with its shared ocular/auditory/ musculoskeletal features from the cited Savasta report. The short-trunk phenotype, the histological 'Swiss- cheese' cartilage, the cervical-spine screening thresholds, the anaesthetic considerations and the supportive multidisciplinary management are standard, well-established teaching. (See also Skeletal Dysplasias, which covers spondyloepiphyseal dysplasia congenita and the severe end of the spectrum, Stickler Syndrome, Atlantoaxial Instability and Proteoglycans & Collagen.)